 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 7, No. 1, March, 2007, pp. 25-32 False teeth “ebiino” and millet disease “oburo” in Bushenyi district of Uganda Fred Nuwaha1,Joseph Okware 1,2, Timbyetaho Hanningtone3 Mwebaze Charles4
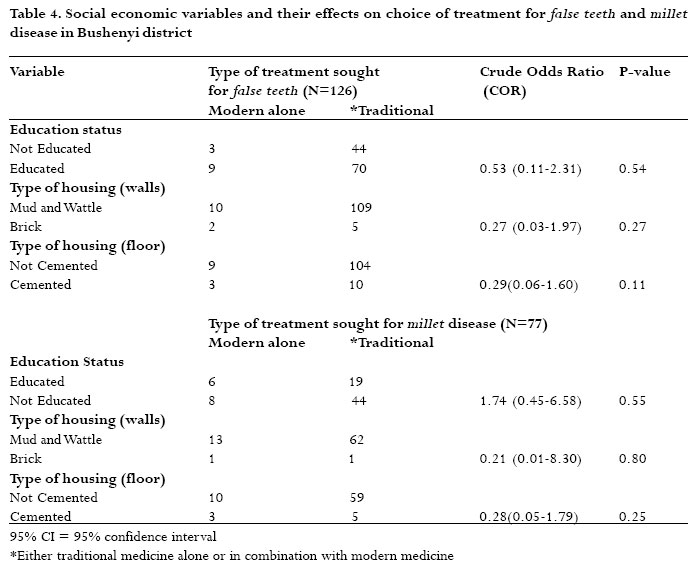
Correspondences: Fred Nuwaha Makerere University Institute of Public Health P.O. Box 7072 Kampala-Uganda Fax: + 256-41-531807; Phone: +256-41-372440 E-mail: nuwahaf@iph.ac.ug, fnuwaha@iph.ac.ug Code Number: hs07006 Abstract Background:“False teeth” (Ebiino) and “Millet disease” (Oburo, Tea-tea) have been reported in Uganda and other countries in Sub-Saharan Africa. These two perceived diseases are commonly reported in children under-five years of age. Anecdotal and published evidence suggests that these conditions are associated with moderate to severe childhood diseases such as malaria, pneumonia and diarrhoea and that most health seeking behaviour for the conditions is from traditional healers. Keywords: Malaria; Pneumonia; Diarrhoea; health seeking behaviour; access to health facilities; traditional medicine; health beliefs. Introduction “False teeth” (plastic teeth, Ebiino) and “Millet disease” (Oburo, Tea-tea) have been reported in Uganda1-7 and other countries in Sub-Saharan Africa.8-15 These two perceived diseases are commonly reported in children under-five years of age.1-15 Anecdotal and published evidence suggests that these conditions are associated with moderate to severe childhood diseases such as malaria, pneumonia and diarrhoea and that most health seeking behaviour for the conditions is from traditional healers.1- 15 This is clearly worrisome for several reasons. First the biomedical symptoms associated with false teeth and millet disease constitutes more than 75% of causes of underfive mortality in Uganda and many part of Africa.4-6Second seeking care from traditional healers may delay life saving care from modern health practitioners.2, 4Third modern treatment may be withheld in preference to traditional medicine particularly for severe disease.2, 3, 6 Fourth the methods used in traditional treatment for these disease conditions may lead to complications such as over-bleeding, septicaemia, aspiration pneumonia and risk of transmission of blood borne infections such as hepatitis B, and HIV.4, 6Finally the practices related to these disease conditions may be deeply rooted in people’s beliefs and therefore difficult to modify or change.14, 16 Thus the aims of this work is to estimate how common the two perceived disease conditions (false teeth and millet disease ) are in children in Bushenyi district of Uganda, to understand people’s health seeking behaviours and the perceived causes attributable to these diseases. Methods Design This was a cross sectional survey where data was collected using pre-tested semi-structured questionnaire. The questionnaire had both closed and open-ended questions. Data was collected during November and December of 2001. Study setting The study area was Bushenyi district located in southwestern Uganda that covers an area of 3949 square kilometers.The district with a total population of 800,000 people (projected from 2002 census) is divided into 7 health sub-districts (HSDs), 29 sub-counties, 170 parishes, and 2049 villages. The office of the district director of health services (DDHS) is responsible for delivery of health services to population. There are 79 health facilities and 215 immunization posts in the district that constitute the district health system. About 60% of the population is in a walking distance of five kilometers of a health facility. The major causes of mortality and morbidity in the district are malaria, acute respiratory infections, diarrhoea, malnutrition and perinatal conditions. These five conditions are responsible for more than 80% of the causes of death and ill-health in children less than five years. Other socio-economic indicators for health are not favourable in the district. There are shortages of drugs, diagnostic and other equipment, and health workers (with more than 40% of total establishment not filled). The safe water coverage stands at about 60% and latrine coverage at 75%. Sample size and sampling The sample of households for the interview was determined using the expanded programme on immunisation (EPI) cluster sample method17. The sample size was based on that required to determine the prevalence of the disease conditions in the population with a 5% level of significance and 80% power. This method is normally used to calculate immunisation coverage but was deemed adequate to estimate the prevalence of the two perceived diseases-“Millet disease and “False teeth”. A multistage sampling method was used to obtain an appropriate sample for the study. To obtain 210 households and thirty clusters from the district, the following procedures were followed. The 30 clusters were allocated to the seven health sub districts (constituencies) basing on their variations in population size. Five health sub districts of almost equal population were allocated 4 Clusters each and two health sub-districts with a higher population were allocated 5 clusters each to make a total of 30 clusters (villages). From each health sub-district, villages were randomly selected from a listing of all villages. In each village selected, 7 homes (starting from a randomly selected house) were visited and the head of household or the spouse was interviewed.The heads of households or their spouses were preferred for interview because they were considered to be knowledgeable about the health issues in their communities. When there was nobody to interview at the time of the visit or if the household did not have any child below five years, a neighbouring house was included. Data was collected on socio-demographic characteristics at the time of the interview, knowledge on cause, prevention, and treatment of the perceived diseases (false teeth and millet disease), and history of occurrence of false teeth or millet disease in a household and on type of health care offered to the patients of false teeth or millet disease. Data management and analysis The data collected was edited, coded and cleaned before analysis. Statistical packages Epi info 2002 (CDC, Atlanta Georgia) and version 8 of STATA for Windows (StataCorp LP) were used in the analyses. Frequencies were computed and univariate analysis with the chi- square or Fisher’s exact test using two-tailed tests was used to compare proportions. Crude odds ratios (COR) and their 95% confidence interval (CI) were calculated. The proportions were adjusted using STATA that took into consideration the cluster sampling technique. Quality control Threats to validity and reliability of data were minimized through training of all research assistants.The questionnaires were checked at the end of each day for omissions and inconsistencies.The questionnaires were pre- tested to ensure clarity and logical sequence.The principal investigators (JO and CM) closely supervised the research assistants. Furthermore, the questionnaires were translated in the commonly used language (Runyankole) and back to English. Ethical considerations Permission was got from Makerere University institute of Public Health Institutional review board (MUIPH), the Uganda National Council for Science and Technology (UNCST), and the DDHS-Bushenyi. Prior to data collection community leaders were informed about the study and gave their consent. Informed consent was also obtained from the respondents before the interviews. Results Social-demographic characteristics of respondents All the 215 respondents interviewed were adults. The youngest respondent was 18 years old and the oldest respondent was 100 years old with a median age of 38 years and the standard deviation (SD) being 18 years . The majority (60%) of the respondents were women but the study team interviewed almost as many heads of households (107) as spouses (104). Table 1 shows the comparison of various socio-demographic characteristics stratified by sex. Perceived occurrence of false teeth and millet disease Of the 215 respondents interviewed during the study 126 (58.6%) reported that at least one child less than five years in the household has ever suffered from false teeth in the last five years (Ebiino) and 74 (35%) said that at least one child had suffered from false teeth in the previous 12 months. Of the 215 respondents interviewed 77 (35.8%) reported that at least one child less than five years in the household has ever suffered from millet disease (Oburo) in the last five years and 50 (23.5%) said that at least one child had suffered from millet disease in the previous 12 months. Perceived cause of false teeth and millet disease Of the 214 respondents who said that they knew what false teeth is, 150 (70%) said they don’t know the cause(s) of false teeth, while 64 (30%) respondents attributed false teeth to a number of causes as shown in table 2. Of the 74 respondents who had at least one child under five years suffering from false teeth in last 12 months, 49 (67%) said that the cause of false teeth is prolonged or excessive diarrhoea. Similarly the majority of respondents 135 (63%) said that they did not know what causes millet disease. Only 80 (37%) mentioned causes of millet disease as shown in table 2. Of the 50 respondents who had at least one child under five years suffering from millet disease in last 12 months, 36 (72%) said that the cause of millet disease is difficulty in breathing (described as ebyemerero in Runyankole language). Treatment of false teeth and millet disease Out of the 126 respondents who said they ever had a child less than five years suffer from false teeth in the last five years, 12 (10%) said that they used modern medicine alone, 88 (70%) said that they used traditional medicine alone and 26 (21%) said that they used both modern and traditional medicine. Thus 114 (90%) at least used traditional medicine (either alone or in combination with modern medicine). Of the 74 respondents who said that at least one child in the family has ever had false teeth in the 12 months, 7 (9%) said that they treated the false teeth with modern medicine only, 47 (61%) said that they treated the false teeth with traditional medicine alone and 22 (30%) said that they treated the false teeth with both traditional and modern medicine. Thus 69 (93%) used at least traditional medicine for treating false teeth. All the 214 respondents were further asked whether in their own assessment or experience they believe that modern medicine could cure false teeth. Only 40 (19%) said that modern medicine can cure false teeth. The majority, 125 (58%) said that modern medicine cannot cure false teeth and the rest 49 (23%) were not sure whether modern medicine can cure false teeth. Out of the 77 respondents who said they ever had a child less than five years suffer from millet disease in the last five years, 14 (18%) said that they used modern medicine alone 44 (57%) said that they used traditional medicine alone and 19 (25%) said that they used both modern and traditional medicine. Thus 63 (82%) of the respondents at least used traditional medicine for treating millet disease. Out of the of the 50 respondents who said at least one child under five years in their family had millet disease in the last 12 months, 10 (20%) treated the millet disease with modern medicine alone, 17 (34%) used traditional medicine alone and 23 (46%) used both traditional and modern medicine. Thus 40 (80%) of them at least used traditional medicine (either alone or in combination with modern medicine) for treating millet disease. All the 215 respondents were further asked whether in their own assessment or experience they believe that modern medicine could cure millet disease. Of the 215 respondents, 109 (51%) said traditional medicine is the cure for millet disease, 42 (19%) said modern medicine is the cure for millet disease and 30 (14%) of the respondents said both types of treatment are equally good and the rest 34 (16%) said that they could not commit themselves to say what type of treatment cures millet disease. Almost all respondents 201 out of 214 (94%) said that traditional treatment (extraction) for “false teeth” (ebiino) involves a small incision in the gums of the child followed by removal of the “teeth”. The child is then started on a course of herbs (both orally and for cleaning the mouth) as postoperative treatment. Similarly the majority of respondents 153 (71%) said that traditional treatment (extraction) for “millet disease” (oburo) involves incisions on the chest of the child followed by removal of the “millet” grains (most likely blood clots mixed with body fat that resembles millet grains). The child is then started on course of herbs (both orally and by smearing on the wounds). Effect of socio-economic conditions on perceived occurrence of false teeth and millet disease Level of education of head of household and type of housing were used as proxies for socio-economic situation to gauge whether they influence ever having false teeth or millet disease in the last five years. As seen in table 3 the higher the level of education of the head of household the lower the likelihood of occurrence of false teeth in the household. Similarly living in a brick Similarly living in a brick walled house and having cemented floor reduced the chance of occurrence of false teeth in the household. The situation is similar for millet disease. Level of education, living in a brick house, living in a house with cemented did not favour occurrence of millet disease in the household. Effect of socio-economic conditions on choice of treatment for false teeth and millet disease We analysed socio economic conditions in relation to seeking modern or traditional treatment among households that had a child with false teeth or millet disease in the last five years. We compared those households who received modern medicine alone (the correct form of treatment) to those that received at least traditional medicine (traditional medicine alone or in combination with modern medicine). As seen in table 4, the level of education of head of household does not influence choice of treatment for false teeth. Similarly living in a brick walled house and having cemented floor did not influence choice of treatment for false teeth. The situation is similar for millet disease. Level of education, living in a brick-walled house, living in a house with cemented did not influence choice of treatment for millet disease. Discussion We found that the false teeth and millet disease were perceived to be very common in Bushenyi district of Uganda. An estimated one in two households in the district reported a patient of false teeth or millet disease in the last five years. Our data also indicate that the perceived causes of false teeth and millet disease are mainly attributed to natural causes (such as excessive or prolonged diarrhoea, difficulty in breathing and excessive or prolonged fever) rather than to supernatural causes (such as avenging spirits or witchcraft). These data also indicate that the predominant method of treatment for false teeth and millet disease is traditional medicine rather than modern medicine. We further demonstrated that whereas high socio-economic conditions do not favour perceived occurrence of false teeth or millet disease the high social economic conditions did not have any influence on use of traditional or modern medicine for the perceived diseases. A limitation of this study could have been recall bias, where respondents could have forgotten events that happened in the past. However, we think that both false teeth and millet disease are major life events in a family that are less likely to be forgotten. The perceived causes of false teeth and millet disease are related to common childhood disease symptoms (diarrhoea, fever and difficulty in breathing) in this district. An earlier study in a neighbouring district has established that about 85% of all deaths in children less than five years are attributable to malaria, pneumonia and diarrhoea18. Therefore respondents describing major childhood diseases in terms of their symptoms are not surprising. More than 60% of the respondents said that they did not know the cause of false teeth or millet disease. This is encouraging and suggests that health education has a big role to play. By developing appropriate education messages that take into community perspective of illness, it should be possible to influence the thinking and health seeking behaviour for false teeth and millet disease. This strategy had been tried and had some positive influences in neighbouring Mbarara district3. The proxies used for measuring social-economic status have been previously tested in this region and found reliable19. The perceived occurrence of false teeth and millet disease in the district is influenced by social economic status. A likely explanation for this observation is that lower social economic status in society are bound to have low access to preventive services and therefore are more likely to be over-burdened by childhood diseases20. Evidence from the Uganda demographic and health survey of 2000/01 (20) suggest that the high social economic class are more likely to: have lower total fertility (4.1 versus national average of 6.9), deliver in health units under supervision (76% versus national average of 36.6%); own a mosquito net (40% versus national average of 13%); and more likely to have better housing with adequate water and excreta disposal facilities. Thus improvement in access to preventive and curative health services particularly among people of low social economic status may reduce the prevalence of false teeth and millet disease. This study found that social economic situation did not influence choice of health care for false teeth or millet disease. One explanation could be that health seeking behaviour was assessed as an end point rather than a process in this study. Another possible explanation for this is that the majority of the people used traditional medicine and investigating the effect of social economic status on choice of treatment would have required a bigger sample size. It is also important to note that since high social economic status reduces occurrence of false teeth and millet disease most of the households with false teeth and millet disease are already of low social economic class and this reduces the power of the analysis further. We think that the most likely explanation for this is that moderate to severe childhood disease are difficult to treat in low income countries including Uganda (even with modern medicine) for various reasons including low quality of care, drug resistance and due to limited access of treatment21. When community members do not get a cure after attempting modern medicine, it is becomes more difficult to comprehend the reasons for failure and this encourages the belief that modern medicine is infective leading to resorting to traditional medicine. As these beliefs get rooted in the population they become more difficult to change thereby perpetuating the vicious cycle. Evidence for these assertions has been reported in Uganda16, 22-23 before with similar trends having been observed in other settings24. It is important to note that symptoms described by respondents in this study regarding false teeth and millet disease are either severe or prolonged. The choice of type of medicine by community members is however dynamic and varies with time and with improvement in the quality and quantity of modern health services as has been observed in Uganda and Tanzania23,25.We recognize that our study was not designed and could not adequately answer some of these questions. We thus propose additional research (probably using qualitative/anthropological methods and being longitudinal in design) to generate more data. Additional data is particularly needed on timing of health care and on possible interventions for addressing these perceived disease conditions. The results of this study are however, useful to clinicians and programme managers in several ways. First clinicians may actively question mothers or caretakers of children under their care about possible occurrence and treatment of false teeth and millet disease. By the clinicians successfully treating these disease conditions using modern medicine, the mothers or care takers would go back to their communities and spread messages that modern medicine is effective for treatment of the perceived disease23. Second this study provides data on beliefs (such as linking the perceived diseases with symptoms of childhood illness) where appropriate health education messages for confronting false teeth and millet disease could be based. Finally these data also suggest that the low social-economic section of the population requires targeting for prevention of false teeth and millet disease. Acknowledgements We are indebted to Mr. Mutungi Pantaleo and Mr. Babikunyamu Charles, for coordinating the data collection. We thank the district director of health services Bushenyi for support and for permission to publish. UNICEF and Bushenyi Local Government financially supported the study. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07006t2.jpg] [hs07006t1.jpg] [hs07006t4.jpg] [hs07006t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}