 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
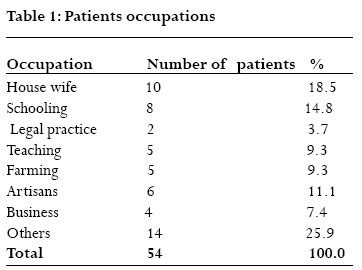
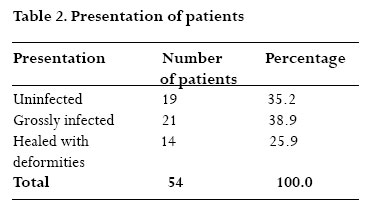
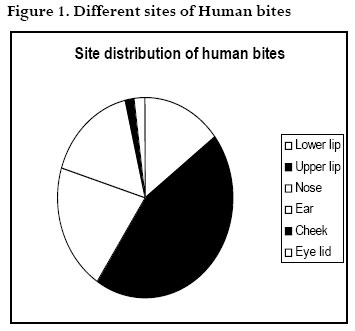
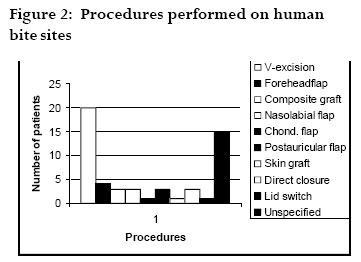
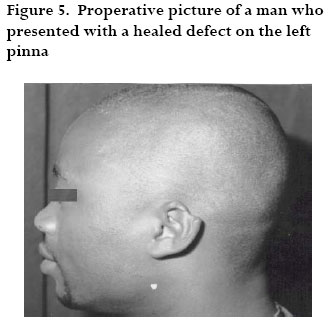
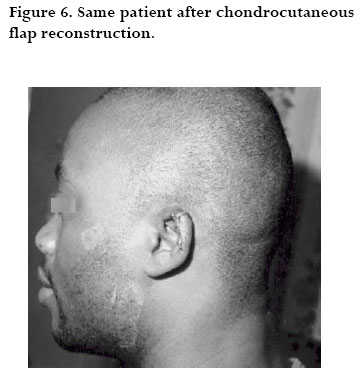
African Health Sciences, Vol. 7, No. 1, March, 2007, pp. 50-54 Management of human bites of the face in Enugu, Nigeria. 1Peter B. Olaitan; 2 Antonia O; Uduezue; 3 Godwin C. Ugwueze., 3Iheuko S. Ogbonnaya and 3Uche J.Achebe. 1Formerly of Plastic and Reconstructive Surgery Department, National Orthopaedic Hospital, Enugu, Nigeria; Correspondence P.B.Olaitan Dept of Surgery. Ladoke Akintola University ofTechnology Teaching Hospital, Osogbo, Osun state,Nigeria. E-mail:emiolaitan@yahoo.com Tel: 234 8033609292 Code Number: hs07011 Abstract Background: Human bites of the face present to the surgeon sometimes with a dilemma as to the method and timing of surgery. Often patients present with soft tissue defects as a result of the injury sustained. Reconstruction therefore becomes absolutely necessary to avoid psychosocial complications. Key words: Human bite, face, presentation, management, Enugu, Nigeria. Introduction Human bite injuries carry the risk of being infected with the bacteria flora of the oral cavity. This often leads surgeons to consider initial debridement and delayed closure because of the fear of wound infection. There have been several reports of facial bites from humans in the literatures1- 4 . Prophylactic antibiotic treatment and primary closure of bite wounds remain areas of controversy5. Opinions tilt towards the fact that Primary surgical repair is the treatment of choice for most clinically uninfected facial bite wounds, whereas delayed closure should be reserved for certain high risk or already infected wounds6. Bites on the face also present as a surgical challenge. More so when there is partial or total loss of important structure(s) of the face like the ears, the eyelids, the nose, the lips and other parts of the face. Avulsive injuries with significant tissue loss represent the most difficult cases for definitive management and are also those most likely to require hospitalization6 and possibly specialized reconstructive options. The cosmetic effects of such losses are profound and may affect the social and even sometimes economic live of the individual patient involved. Many of the patients who sustain human bite of the face present with healed wound but with disfiguring scars and deformed facial appendages also needing reconstruction. We report the presentation and management of patients who presented with human bites of the face to our centre over a 10-year period. The aim is to highlight the presentation, areas involved, reconstructive options, and complications observed in managing these patients in our centre. Materials and methods A retrospective study of patients with human bites of the face who presented between January 1994 and December 2003 was carried out using operation registers, case notes and attendant registers at the Accident and Emergency unit of our hospital.All the patients were treated in the Plastic Surgery Department of the National Orthopaedic Hospital, Enugu, Nigeria within the period. Information obtained on the patients includes age, gender, time of presentation after the injuries, nature and circumstances of the injuries, sites of injuries and treatment offered to the patients as well as the complication(s) observed. Data was recorded and analyzed using SPSS version 10. Results A total of 54 patients with human bites of the face were treated in our unit during the period under study.The age range of the patients was 16-54 years with a mean of 33.8±2.3 years and a peak age of 26-30years. Male victims were 33 and females 21 with a ratio of 1.6:1 respectively. Information on assailants’ sexes was present only in 42 patients with a M: F ratio of 15: 27 (or 0.6:1). Occupations of the victims were as shown in table 1 with house wives having the largest number. Fifty of the assailants were well known to the victims while 4 were total strangers. All the injuries were sustained during fights and the time of presentation ranged between 3 hours to 6months with an average time of presentation being 52±2.1days. Only 19 (35.2%) of the patients presented within 24 hours. All patients who presented within 24 hours had minimal debridement and primary closure of the defects while others with infected wounds were dressed till wounds were clean enough for closure and repair undertaken usually within one or two weeks. There were 19 (35.2%) and 21 (38.9%) patients with clean and grossly infected wounds respectively. Healing had taken place in the remaining 14 (25.9%) cases (table 2). Sites of injuries were (Fig.1) the upper lip 24 (44.4%), followed by the nose, 11 (20.4%), ear, 9 (16.7%), lower lips, 8 (14.8%), eyelid and cheek 1 (1.8%) each.The injuries were single in 38 (70.3%), multiple in 2 (3.7%) of the patients while the other 14 patients who had healed wounds had no information on whether the injuries were single or multiples.The parts of the upper or lower lip bitten off were also not documented in the case notes in most of the patients except 8 patients, with central part in 5 lips, the commisure in 2 patients and the right side of the lower lip in one patient. All patients with fresh or infected wounds were given antibiotics with Metronidazole and anti tetanus prophylaxis. Procedures performed were as shown in Figure 2 and included v-excision and closure of the lips in 20 lips (37.0 %), midline forehead flap cover in 4 (7.4 %) patients and composite auricular graft in 3(5.6 %) patients. Nasolabial flaps were used to reconstruct the nose in 3 (5.6 %) patients while chondrocutaneous flap was used in one ear, post auricular flaps in 3, skin grafts in one and direct suturing in 3 (5.6 %) patients while one (1.9 %) patient with eyelid injury had a lid switch. Complications of the procedures include a failed composite auricular graft and hypertrophic scars in the lips of 4 (7.4%) of the patients. The lip scars were treated conservatively with kenalog(triamcinolone) cream.The patients who had a lid switch had a notch for which he refused revision. Discussion The oral cavity harbors a wide range of bacteria flora with B-haemolytic streptococci and bacteroides species being the most frequent isolates and hence human bites are potentially infective. Septicaemias, infections with Human ImmunodeficiencyVirus and indeed deaths have been reported from human bites7-11.While the HIV status of our patients in this study was not assessed routinely in the earlier years of this study, we later commenced screening of the status of both the assailants and the victims with a view to commencing prophylaxis antiretroviral dugs where applicable. We did not have any reported case of HIV infection from the bites. Most of the bites from this study, inflicted mostly by women, were either as a means of defense or to deface the victims.There were no reported cases of passionate love bite, clinical vampirism/pseudovampirism, or cannibalism. Women form the larger number of patients in previous reports12-14. Datubo-Brown11 reports that most of his patients were semi-illiterate adult females in their third decades. Our study shows more male victims than females (1.6:1) while there were more female assailants than male. Our patients were also from various social strata –undergraduates, teachers, lawyers, etc and the injuries resulted from scuffles-4 of who were separating people fighting. Fifty (92.4%) of the assailants were known to the patients including husbands, wives, and sisters- in- law.This compares with Datubo-Brown13 and Odukwe’s14 series. Donkor and Bankas10 studied 30 patients who presented with human bites of the face and noted that a thorough debridement followed by primary closure; direct suturing, a local flap, or skin grafting on the day of presentation resulted in 90% complete wound healing. Obukwe14 reports that none of the bite injuries in his review became infected.This was attributed to early local wound care and systemic antibacterial therapy. It has been demonstrated that the pathogens in human bite infections differ considerably from those present in animal bites15 and higher prevalence of Staphylococcus aureus and Eikenella corrodens16 have been noted in human bites compared with animal bites. Phenoxymethyl penicillin has been suggested as the drug of choice in treatment ofinfections associated with cat and dog bites16. Prophylactic antibiotics and antitetanus were routinely used in our patients. None of the victims in Obukwe’s series planned to seek legal redress for the bite injuries as matrimonial conflict related to polygamy was the commonest reason for assault, with females predominating as assailants. Four of our patients in the current study however sought for legal redress needing the preoperative pictures for evidence in court. We therefore suggest that a good preoperative picture is mandatory in managing these patients as has been previously documented17. Uchendu4 has previously reported management of human bites of the lips by aggressive approach of primary wound closure in our centre. Our current study is not limited to the lips but also includes other facial structures such as the nose, the cheek, the ears, the eyelids and the lips. Treatment offered to patients in this study included wound debridement and direct suturing of wounds that were not grossly infected (Fig. 3 & 4). Patients who presented with freshly inflicted wounds had immediate debridement and reconstruction while those who presented with obviously infected wounds had debridement of the wounds with delay primary or secondary closure/reconstruction. Reconstruction of the defects/deformities were done for patients with healed wounds. Other complex procedures like a V-wedge excision, flap cover of the defects such as chondrocutaneous flaps (Fig.5 & 6), midline forehead flap, nasolabial flaps, composite auricular graft and skin grafts were also carried out in some of the patients. Complications observed in our patients include a failed composite graft, hypertrophic scars in 4 patients (on 3 of the lips and one ear). One of our patients who had an eyelid switch also had a notch. Infection was not observed as a complication of any of the wounds that were closed early. Conclusion We conclude that human bites of the face are still common in our society. The injury cuts across all social strata. Minimal debridement and primary closure is effective when patients present early. Some of the patients may need to have specialist care/reconstruction, which may only be provided by a surgeon who is skilled in reconstruction. Early referral of these patients to a Plastic, Maxillofacial, or any surgeon with reconstructive skills is therefore advocated in cases of extensive injuries. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07011f3.jpg] [hs07011f5.jpg] [hs07011f1.jpg] [hs07011t1.jpg] [hs07011t2.jpg] [hs07011f6.jpg] [hs07011f2.jpg] [hs07011f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}