 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
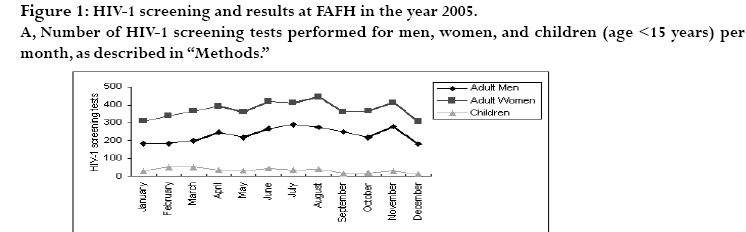
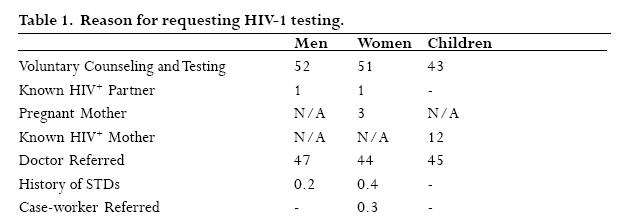
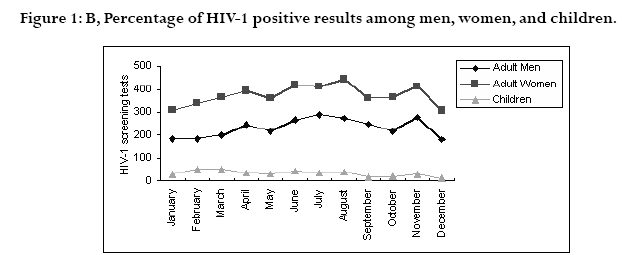
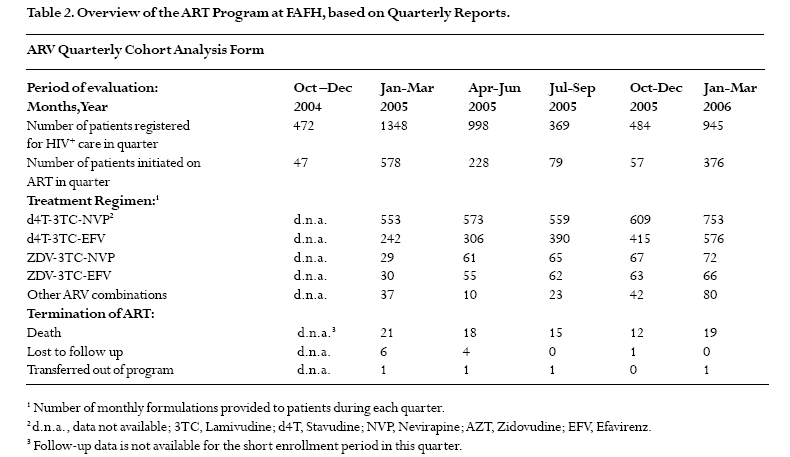
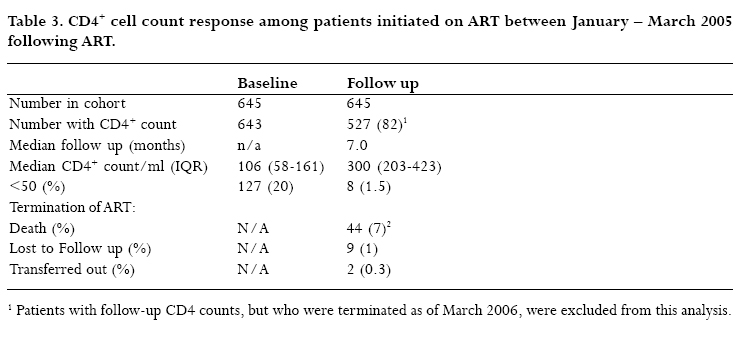
African Health Sciences, Vol. 7, No. 2, June, 2007, pp. 93 - 100 Expansion of HIV-1 screening and anti-retroviral treatment programs in a resource-poor setting: results from a faith-based organization in Jos, Plateau State, Nigeria Lum, Hillary1; Isichei, Christian 2 ; Isichei-Wakili, Mercy3; Redfield, Robert 4. University of Wisconsin School of Medicine and Public Health, Madison,WI1; Faith Alive Foundation Hospital and Department of Chemical Pathology, University of Jos, Jos Plateau State, Nigeria2. Faith Alive Foundation and Surgery Department, Jos University Teaching Hospital3; Institute of Human Virology, Baltimore, MD4; Correspondence: Christian Isichei Jos, Nigeria E-mail: Christian_isichei@yahoo.com Code Number: hs07019 Abstract Background: Until recently, availability of anti-retroviral therapy (ART) in Nigeria has been limited to government and universitybased programs.Through the United States’ President’s Emergency Plan For AIDS Relief (PEPFAR), additional funding has become available for the treatment of HIV-positive patients. Key Words:HIV;ART program;Nigeria,resource-poor IntroductionNigeria, Africa’s most populous country, has an estimated total population of 130-150 million. Based on national sentinel surveys, the prevalence of HIV among adults in Nigeria increased from 1.8% in 1991 to 5.8% in 2001 1, 2 and in 2003 at 5.0%.With more than 3.5 million people estimated to be living with HIV at the end of 2003 3 , Nigeria has the largest number of HIV/AIDS cases in West Africa. A recent study at Jos University Teaching Hospital (JUTH), in collaboration with the AIDS, Prevention in Nigeria (APIN) program, found that the prevalence of HIV among pregnant women was estimated to be 8.2% 4 . Furthermore, this study showed that the prevalence of HIV infection was as high as 10.9% in subjects ages 25-29 years old. In January 2002, the Federal Government of Nigeria initiated a national ART program. This program has provided over 9000 adults with a 3-drug ARV combination regimen consisting of the generic brands of lamivudine, stavudine, and nevirapine at a highly subsidized rate of $10 for the monthly treatment of a patient. The overall results within the first twelve months of treatment indicated an effective suppression of viral replication, the reconstitution of the immune system, and improvement of the physical well-being of the small lamivudine (Lamivir, Cipla), 150 mg twice daily, and stavudine (Stavir, Cipla), 40 mg twice daily, unless otherwise indicated. Prior to initiation of ART, clinical history and baseline data, including CD4+ cell count by flow cytometry, were documented. Patients with a suspicion of tuberculosis (TB) were assessed by chest x-ray, and any HIV-infected patients with concurrent TB infection underwent standard TB treatment for no less than two months before addition of ART. Critically-ill patients due to severe infections and/or malnourishment were not started on ART in an attempt to prevent deaths related to ARV intolerability or severe immune reconstitution syndrome. Patients had regular clinic visits every two weeks and then monthly as the patient’s health status improved and drug adherence was assured. CD4+ cell counts were obtained at baseline and between four and 13 months later. Multiple CD4+ cell counts within the first year of treatment were only available for 91 patients.Thus, the analysis of CD4+ cell count change was based on the first available measurement following initiation of ART. Adherence was monitored through interviewing at each scheduled clinic visit, and emphasized through regular teaching sessions to patients. Patients received nutritional support if needed, and antibiotic prophylaxis with trimethoprim/sulfamethoxazole (Bactrim DS 800 mg/160 mg) was provided according to WHO guidelines to HIV-positive patients until initiation of ART10 . Patient Counseling and SupportAll patients in the FAFH-PEPFAR program were counseled initially and monthly regarding the importance of medication adherence. Patients are strongly encouraged to disclose their HIV status to close family relations to increase adherence and to sign partnership contract forms with partners who help to encourage adherence. A mobile, multidisciplinary medical/ psychosocial team (home-based care) visited criticallyill patients approximately 5 days each week.This enabled FAFH staff to monitor ARV administration and adherence, as well as to assess the impact of factors in the home and family on treatment. A weekly patient-led support group of approximately 200 members meets to discuss issues pertinent to people living with HIV and AIDS. The FANOL Bank was available to provide patients with food as needed. Analysis of DataData collected for each patient at baseline and follow-up visits were stored in patient charts, entered into the HRSA CAREWARE medical record system, and individually recorded by each team. Quarterly reports were generated by FAFH Monitoring and Evaluation staff. Patients for the cohort analysis were drawn from each team, and confirmed by CAREWARE records. All the data were collated and analyzed statistically using Epi-Info version 6.04 (Centers for Disease Control,Atlanta, GA) and Stata version 6.0 (College Station, TX). The median and interquartile ranges were estimated for CD4+ cell count at baseline and at follow-up. Changes from baseline with respect CD4+ cell count were analyzed using the Wilcoxon matched-pairs signed-ranks test. Results HIV-1 Screening and Counseling FAFH is a major referral center for persons potentially infected and affected by HIV infection, especially among persons unable to pay for medical care. On-site VCT services are coordinated by Faith Alive Counseling and Laboratory personnel. Figure 1A shows the number of adult men, adult women, and children who were screened for HIV-1 serostatus in each month of 2005. A total of 7672 persons were screened over the twelve month period, and sixty-four percent of the population screened was female. Four hundred (5.2%) children were screened. Surveys administered by the FA VCT Counseling Section at the time of HIV-1 screening were used to determine the primary reason individuals requested testing among seven possible factors, shown in Table 1. Results from surveys of individuals requesting HIV-1 screening at FAFH in 2005. Data shown are percentages of total number of men, women, or children (age <15 years), who identified a specific factor as their primary reason for seeking testing. N/A = not applicable. For all three populations, VCT and doctor referral accounted for greater than 85% of cases. Among children, 12.2% were tested because their mother was HIV-infected. The percentages of HIV-1 results among each population tested are shown in Figure 1B. A total of 3869 people, or 50.4%, were found to be HIV-1 infected. The prevalence of HIV-1 positivity among individuals requesting screening at FAFH is significantly higher than the documented Nigerian average of 5.0% in 2003 (2). Faith Alive sees many patients who are at higher risk and impoverished. Also, its free medical and social services make care accessible to many who cannot afford care elsewhere. A second confirmatory screening test of UNIGOLD rapid test kit was required before a patient was registered in the FAFH-PEPFAR ART program and considered for ART. Enrollment in ART and initiation of ARV therapy. Enrollment in the FAFH-PEPFAR ART program began in December 2004, and resulted in significantly expanded HIV/AIDS services for HIV-infected individuals. The total number of HIV-infected individuals registered at FAFH increased significantly over the next several months, as shown in Figure 2A. From December 2004 to March 2006, the total number of patients registered at FAFH rose from 1330 to 5946 people. Based on figures at the end of the reporting period (March 2006), the majority (66%) of those enrolled were women, and only 2.2% were children less than 15 years old. Due to the high patient volume, most paediatric cases received at FAFH were referred to the ECWA/Evangel hospital ART program less than one mile away in Jos, which specializes the care of paediatric patients, and recently received PEPFAR funding. Additionally, since mother-to-child transmission is a common cause of paediatric HIV infection, many of these children receive HIV care through the PMTCT-specific APIN program at JUTH. HIV-1 infected patients in WHO clinical stages 3 or 4, or with a CD4+ cell count of less than 200/ml, were entered onto one of four patient care teams that opened in December 2004 and caters mainly for naïve patients. The total number of patients on ART during this expansion in care is shown in Figure 2B. Over a sixteen month period, the number of patients who received ART through the FAFH-PEPFAR program increased from 302 to 1667, of which seventy percent were women. HIV/AIDS Care Program at FAFH Monitoring the expansion of ART programs in resourcepoor settings has been shown to be effective through the use of Quarterly ARV Cohort Analysis Forms6. Thus, Table 2 presents data from the first six quarterly reports of the FAFH-PEPFAR ART program as a means of summarizing aspects of HIV/AIDS care provided at FAFH during the expansion of ART in this setting. The number of patients initiated on therapy greatly increased in the first two quarters of 2005, and then slowed as the four patient-care teams were filled. The significant increase in new patients on ART seen during the first quarter of 2006 resulted from the addition of three more patient-care teams (including a specialized team E which focuses on cases with co-infections, paediatric cases and complicated cases while the other teams provide care for naïve cases, i.e. Teams A1, A2, B1, B2, C, and D), increasing the total to seven, in this period. However, despite this expansion in clinical care capacity, the waiting list for patients seeking ART among patients enrolled at FAFH in March 2006 was between four and five thousand people. A majority of patients were started on first-line simplified HAART consisting of oral nevirapine, lamivudine, and stavudine, as described in the “Methods” section. Other regimens commonly provided at FAFH are shown in Table 2. The number of each ARV combination dispensed indicates the relative proportions of each combination prescribed, as well as the total volume of drugs provided during each quarter. ART patients who did not continue on therapy are reported based on death, no longer coming or unable to be contacted (i.e. lost to follow up), or transfer to another ART program,during each quarterly reporting period. Reasons for termination have not been noted for the first reporting period (Oct – Dec 2004) since patient enrollment began in December 2004 and subsequent clinic visits did not occur during this period. There were however about 266 patients on treatment through the $365/patient/year sponsored ART program before PEPFAR whose records were revealing in terms of good follow up and adherence. The quarterly reports of these early recruits into the PEPFAR program do not reflect deaths of patients who received care at FAFH, but were not initiated on ART. Investigation of this group of patients found concurrent TB infection to be a significant cause of mortality (data not shown). Furthermore, among patients who died while on ART, TB was a leading cause of death when the reason for death was known (data not shown). Cohort analysis of patients on ART for twelve months at FAFH. As one indicator of response to ART, a cohort of patients was analyzed for baseline and follow-up CD4+ cell counts while on ART. The cohort consisted of patients who began ART in the months of January, February or March of 2005. Prior to initiation of ART, clinical and biologic baseline characteristics of 645 patients registered and eligible to receive ART through the FAFH-PEPFAR program were recorded, and data obtained are shown in Table 3. The median CD4+ cell count at baseline was 106/ml, where 127 (20%) patients had a CD4+ cell count of less than 50/l. Throughout ART, patients received medical, social, and spiritual support as described in “Methods”. HIV-1 infected patients in WHO clinical stages 3 or 4, or with a CD4+ cell count of less than 200/ml, were entered onto one of four patient care teams that opened in December 2004 and caters mainly for naïve patients. The total number of patients on ART during this expansion in care is shown in Figure 2B. Over a sixteen month period, the number of patients who received ART through the FAFH-PEPFAR program increased from 302 to 1667, of which seventy percent were women. At least twelve months after initiation of ART for all patients in this cohort (April 2006), analysis of follow-up CD4+ cell counts was performed in patients still on ART (Table 3). A remarkable increase was seen after 7.0 months, the median time to follow-up for the cohort. Of the 527 patients in whom follow-up CD4+ cell counts were available, the median CD4+ cell count was 300/ml, with a median increase of 173/ml over the treatment period. The number of patients who terminated ART in this cohort is also shown in Table 3. Over twelve months after initiation of ART, 591 (91%) were still on ART, 44 (7%) had died, nine (1.4%) were lost to follow up, and two (0.3%) had transferred into other ART programs. Among those who died, at least 5 (11%) were also being treated for TB, and their deaths were attributed to complications due to this opportunistic infection (data not shown). Discussion This report documents the implementation and expansion of simplified HAART at a faith-based medical center in a resource-poor setting. Over the first sixteen months of ART program expansion, over 7500 people were screened for HIV-1 infection, enrollment in the HIV/ AIDS care program increased by over 400 percent to nearly 6000 patients, and more than 1300 new patients were initiated onto ART. In addition to PEPFAR-provided funding for ARVs, this increase in care reflects significant support through private donors, such as the Mennonite Central Committee and the Faith Alive Foundation, as well as substantial commitment by FAFH staff, many of whom volunteer a portion of their time. Altogether, FAFH is a rare model of sustained HIV/AIDS holistic care that is available at no-cost to the patient. The team approach to care is unique and allows continuity of patient care. The response to ART seen in patients at FAFH compares well to that of other sub-Saharan studies also carried out in resource-limited settings. Optimal response to effective ART is indicated by a median rise in CD4 cell count of 100-200/ml within the first year of treatment 11 . In Malawi, a study including 1266 individuals at baseline showed a median increase in CD4 count of 165/ml and nineteen percent mortality after a median follow-up time of 8.3 months 12 . The Nigerian national government study of 50000 patients receiving ART showed an increase in median CD4+ cell count from 260/ml at baseline to 370/ml at six months 5 . As presented here, the median increase in CD4+ cell count in FAFH patients was 173/ml at seven months of followup. Interestingly, the median CD4+ cell count of these patients at baseline (106/ml) was substantially lower than seen in these other study populations or a healthy population. A recent analysis of healthy HIV-negative adults performed in Jos, Nigeria found the mean CD4+ cell count to be 828 cells/ml 13 . Along with the very high rates of HIV-1 infection among patients seeking HIV screening and care at FAFH, we infer that patients at FAFH are a particularly vulnerable population with relatively advanced stages of disease. Nonetheless, in agreement with an analysis that showed attainment of similar increases in median CD4+ cell count among ART programs in low- and high-income settings following 6 months of drug therapy 12 , barriers to HIV care in this resource-poor setting did not significantly affect patient outcomes in this study. Despite the small, but significant, success we have shown in the delivery of ART in this resource-limited setting, this review of our program has also emphasized the increased efforts that are needed to improve the care we provide in prevention, screening, and treating HIVpositive individuals. Specifically, women are nearly twothirds of the total screening population, raising the question of how can men in this community be more effectively reached. Significant issues, including stigma, pride, and fear of losing one’s job or family, are commonly cited reasons with respect to why men are less willing to be tested. Unfortunately, many women come to be tested at FAFH after their husbands have already died of AIDS. In this study, we have shown achievement of increased CD4+ cell count, one biologic endpoint that strongly supports the efficacy of ART in the restoration of the immune system in poor resource settings that do not have access to viral load analysis. In the future, more comprehensive analyses of outcomes of patients treated with ART at FAFH are needed, including changes in viral load, body mass index, and rate of opportunistic infections. It has been shown that the provision of treatment free of charge in low-income settings was associated with lower mortality (adjusted HR 0.23; 95% CI 0.08-0.61) 14 . Further analysis of several ART programs in resource-poor settings found that the provision of medications free of charge was associated with a significantly increased probability of virologic suppression at months six and twelve of ART than when patients were required to pay part or all of the cost of therapy12. In our experiences at FAFH, patients not only require provision of ARVs,but also appropriate treatment of any opportunistic infections, coverage of clinic visit costs, and emergency in-patient care if needed along with provision of some basic Therefore, we have observed that the provision of ART and medical care in a completely no-cost setting, in conjunction with consistent counseling and teaching, positively contributes to ART response and survival among patients seen at FAFH. AcknowledgementsThe authors thank the US PEPFAR program and the Faith Alive Foundation for provision of funding for ART, the Mennonite Central Committee for provision of HIV1 screening tests, and the Faith Alive Foundation for provision of additional medications, programs, and support that enable the provision of holistic medical care. Additionally, we are grateful to the patients who chose to seek their care at FAFH. We also thank the many clinical and support staff of FAFH who were involved in the care of these patients. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07019f2.jpg] [hs07019f1b.jpg] [hs07019f1a.jpg] [hs07019t3.jpg] [hs07019t2.jpg] [hs07019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}