 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
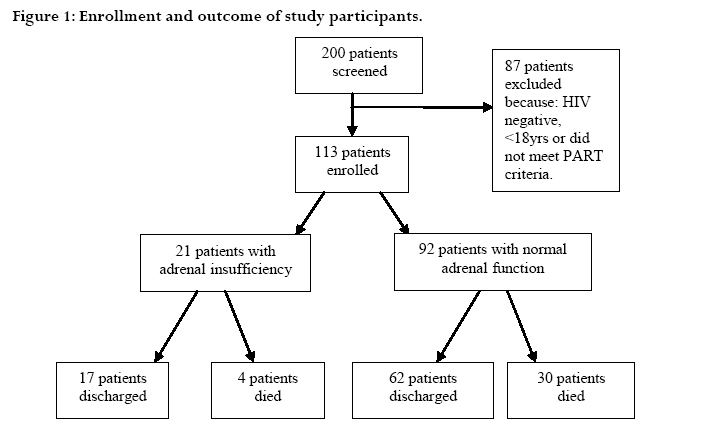
African Health Sciences, Vol. 7, No. 2, June, 2007, pp. 101-107 Functional adrenal insufficiency among critically ill patients with human immunodeficiency virus in a resource-limited setting David B Meya1,2, Elly Katabira1, Marcel Otim1, Allan Ronald2, Robert Colebunders2, 3, Denise Njama1, Harriet Mayanja-Kizza1, Christopher C Whalen4, Merle Sande2 1Makerere University, Faculty of Medicine, Kampala, Uganda Code Number: hs07020 Abstract Background: Functional adrenal insufficiency (FAI) is associated with increased mortality and is defined as subnormal cortisol production during acute severe illness. Key words: Functional adrenal insufficiency, HIV, Uganda List of abbreviations: FAI - Functional adrenal insufficiency, HIV - Human immunodeficiency virus, AIDS - Acquired immunodeficiency syndrome, ACTH - Adrenocorticotrophin hormone, PART - Patient-at-risk team Introduction Adequate adrenal function is essential to survive critical illness1 . Deficiency of cortisol during critical illness, so called functional adrenal insufficiency (FAI), is associated with increased morbidity and mortality2 . Cortisol facilitates the delivery of glucose to cells making it an essential hormone in the metabolic response to stress 3 . The use of low dose corticosteroids in doses of 200-300 mg/24 hours of hydrocortisone improves the prognosis of critically ill patients, especially if given early during the course of Gram negative infections3, 4 . Patients with HIV/AIDS have an increased prevalence of FAI. Marik and colleagues showed that the prevalence of adrenal insufficiency was 75% among severely ill HIV patients admitted to the intensive care unit using a basal stress total serum cortisol threshold of <25 ì g/dl prior to corticotrophin stimulation testing 3 . Potential mechanisms for the development of adrenal insufficiency in patients with HIV infection include: HIV infection of the adrenals or co-infection with cytomegalovirus or mycobacteria5 ; destruction of the adrenal glands by tumor (lymphoma, Kaposi’s sarcoma); adrenocortical hemorrhage secondary to coagulopathy 6,7 ; diminished adrenal secretion as an effect of cytokines such as tumor necrosis factor-á 8,9 ; inhibition of the 11-ß hydroxylase enzyme necessary for steroid synthesis by drugs such as ketoconazole10,11 and rifampicin stimulation of cytochrome P-450 enzyme activity with increased metabolism of cortisol12 . Studies examining the relative role of FAI in HIV/AIDS patients with sepsis and other severe illnesses have not been done in resource-limited settings. Here, we report a prospective study examining the prevalence and factors predicting FAI, as well as the outcome in acutely ill HIV/AIDS patients presenting to Mulago National Referral Hospital in Kampala, Uganda. It is hoped that a better understanding of the frequency and adverse effects of adrenal insufficiency will contribute to future interventional studies among this population of patients to improve outcomes. MethodsThis prospective longitudinal study was conducted in the medical emergency unit of Mulago Hospital, a 600bed tertiary care, referral hospital located in Kampala, Uganda. Patients are admitted for up to 24 hours, after which they may be transferred to the medical wards or discharged after treatment.The prevalence of HIV infection among patients admitted to the medical emergency unit is 46% 13. SubjectsEthical approval was granted by the Makerere University Faculty of Medicine Ethical and Scientific Review Board and the Uganda National Council for Science and Technology. Patients gave informed consent for participation in the study. For patients who were too ill to give individual written consent, the closest relative available gave written informed consent on behalf of the patient. During the period of October to December 2004, 200 consecutive patients were admitted to the emergency ward, gave informed consent, were evaluated using the modified patient-at-risk-team (PART) criteria 14,and were screened for HIV infection.We enrolled 113 HIV-infected patients above 18 years who gave informed consent and had three or more of the following PART criteria: respiratory rate ≥25 breaths /min or < 10 breaths /min; arterial systolic pressure ≤90 mmHg; heart rate ≥110 beats /min or <55 beats /min; not fully alert or orientated; oxygen saturation ≤90% and temperature ≥38°C or <35°C. History and a physical examination were done; presence of any opportunistic infections was documented. Pregnant or lactating mothers, patients who had a known history of primary adrenal insufficiency or had used corticosteroids for more than three weeks prior to admission and any patients who were given corticosteroids by the attending medical team between the time of enrollment and sampling of blood (8-9am) were excluded (n=87). Patients were classified as having FAI if they had single morning cortisol level of ≤ 25 µg/dl. Blood was drawn between 8 and 9 AM the day after admission to determine serum sodium, potassium, albumin, blood sugar, complete blood count and total serum cortisol (BioChem ImmunoSystems Italia SPA, Italy). The mean intra-assay and inter-assay coefficients of variation for measurement of serum cortisol as reported by the manufacturer were 3.1 and 5.7%. Patients were followed-up after admission to the medical wards and clinical information was collected through chart review using a standard data collection form until either discharge or death. Electrolyte concentrations, blood pressure measurements and blood counts used in the analysis were obtained at point of study enrollment. Data collection and analysisThe main outcome was the prevalence of FAI. To identify potential predictors of FAI, we compared patients with and without FAI. Chi-square analysis with Fisher’s exact test (where appropriate) was used to compare categorical data; continuous data were compared using Student’s ttest. Statistical significance was declared for probability values of = 0.05. Univariate predictors were then used in a conditional multivariate logistic regression analysis to define independent factors associated with FAI in this study population. ResultsOf the 200 patients screened, 113 critically-ill HIVinfected patients were enrolled into the study (figure 1). The patients’ mean age (Standard Deviation, SD) was 35 (9) years; 63 (56%) were female. Of the 113 patients enrolled, 21 patients (19%, 95% CI 11-26%) had FAI. Pulmonary infections and cryptococcal meningitis were the most common opportunistic infections in the study population, regardless of FAI (Table 2). Table 1 showing characteristics of patients with FAI compared to patients with normal adrenal function
Table 2. Major diagnoses and opportunistic infections in critically ill HIV-infected patients with and without FAI diagnosed by stress cortisol level ≤25µg/dl.
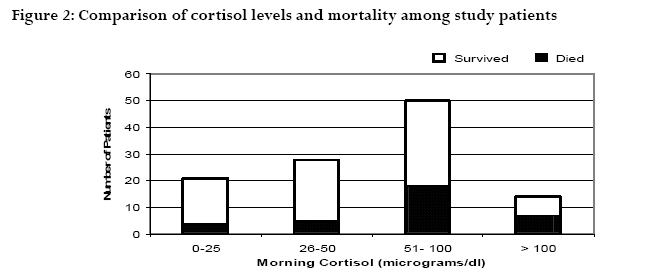
Fatigue, anorexia, weight loss and vomiting occurred with similar frequency among patients with and without FAI. Forty percent of patients reported having had symptoms for more than 14 days prior to admission while 34% reported symptoms lasting between 2-7 days prior to admission. Half the patients were taking trimethoprim-sulphamethoxazole for prophylaxis against opportunistic infections; 9 (8%) patients were taking rifampicin as part of treatment for tuberculosis. Forty four percent of the patients had a Karnofsky score less than 50. Mean electrolyte levels were normal among patients with and without FAI, while the main outcome measure, cortisol, had a median level of 55 µg/dl (3-295 µg/dl) [Table 3].The majority of patients had morning cortisol levels ranging from 51-75 µg/dl (figure 2). Overall, 29% of study patients had eosinophilia greater than 3% of total white blood cells. Hyperkalemia, hypoglycemia and hyponatremia were not found to be associated with FAI. Five (24%) patients with FAI were being treated for pulmonary tuberculosis with rifampicin compared to 4 (4%) of those with normal adrenal function (p-value 0.011, OR 7, 0.035-0.601). Of the 46 patients with clinical suspicion of active tuberculosis, 8 (17%) had FAI (Table 2).Treatment with ketoconazole was not associated with FAI. Of the 21 patients with FAI, 12 (57%) had stage IV HIV disease (WHO criteria) compared to 31 of 92 (34%) patients with normal adrenal function (p= 0.046) [Table 1]. Table 3. Laboratory characteristics of study patients
There was no difference in the occurrence of hypotension when patients with FAI were compared to those with normal adrenal function. Sixty-six (72%) patients with normal adrenal function had an axillary temperature >37.5°C while only 10 (48%) patients with FAI were febrile at admission (p=0.034). Eleven of twenty-one (52%) patients with FAI had eosinophilia while only 22 of 92 (24%) patients with normal adrenal function had eosinophilia (p-value 0.010, OR 3.5, 1.31-9.34) (Table 1). The majority of patients who died in hospital had morning cortisol levels between 51-75 µg/dl (fi-gure 2).There was no significant difference in the mortality when the two groups of patients were compared; while 4 (19%) patients with FAI died, 30 (33%) of those with normal adrenal function died (p=0.221).The mean cortisol level among patients who died (80.5 µg/dl) was significantly higher when compared to the mean cortisol concentration among patients who were discharged (56.5µg/dl) (p= 0.016). Two of the four patients with FAI who died had a diagnosis of cryptococcal meningitis with intracerebral edema while two others died of respiratory failure as a complication of pulmonary Kaposi’s sarcoma. On bivariate analysis, factors that predicted FAI included: use of rifampicin, HIV stage IV disease, and eosinophilia. Neither systolic hypotension nor ketoconazole use were associated with FAI. It appeared that trimethoprim-sulphamethoxazole administration and tachycardia (>110/min) were associated with decreased prevalence of FAI in this patient population. On multivariate analysis, only the use of rifampicin (pvalue 0.004, OR 11.4, 2.15-60.34) and eosinophilia (pvalue 0.008, OR 5.2, 1.53-17.61) were independently associated with FAI (Table 4). Table 4. Factors associated with FAI on multivariate analysis
Discussion In this prospective study, the prevalence of FAI among critically-ill HIV patients was 19%, and FAI occurred 11-fold more often in patients taking rifampicin.The 19% prevalence of FAI observed in this African cohort compares closely with results of a study by Casado and colleagues who found adrenal dysfunction with a prevalence of 22% among patients with AIDS in Spain 15. In an optimal setting, adrenal function is measured using a stimulation test where a standard dose of ACTH is given and adrenal response is measured after 30 and 60 minutes.This testing procedure is expensive, time consuming, and not logistically feasible in most resource-limited settings. Casado and colleagues suggest that an isolated morning basal cortisol level can be useful for the diagnosis of adrenal insufficiency in AIDS patients when a stimulation test is not available15 . Adrenal function in our study was assessed by a single total serum cortisol assay without a stimulation test at a cost of 11 USD. Rifampicin use was associated with FAI in this study population. The possible explanations for this observation include; Mycobacterium tuberculosis infection of the adrenal gland or induction of the cytochrome enzyme system which enhances the metabolism of cortisol. Mycobacterium tuberculosis infection has been associated with FAI when the adrenal gland is involved in disseminated infection16 . Studies in Kenya by Hawken and colleagues, however, did not show any increased prevalence of adrenocortical insufficiency in HIVassociated tuberculosis17 . Of the 46 patients with clinical suspicion of tuberculous disease, 8 (17%) had FAI in our study. Adrenal gland involvement was found to be more common in late stages of HIV infection, with WHO stage IV disease. These findings were similar to those reported by Hoshino18 . Eledrisi and colleagues suggest that postural hypotension may be a more specific manifestation for adrenal insufficiency19 . About a fifth of our study patients had postural hypotension, however, no association was observed between postural hypotension and FAI. No differences in the mean sodium and potassium levels were noted among patients with and without FAI. The overall mortality rate among study patients was high (30%). However, the mortality rate among patients with FAI was not significantly higher than among patients with normal adrenal function, but the small sample size precludes a definite statement about mortality differences. Furthermore, although the numbers were small, patients with FAI who received steroids in hospital all survived whereas 30% of those with FAI who were not given steroids in hospital died, suggesting a potential benefit of corticosteroid administration in a population of patients with risk factors for adrenal insufficiency. Of note, patients who died had a higher mean cortisol concentration when compared to those who were discharged. Others have also found that very high cortisol levels may be associated with a poor prognosis 20. Patients who died may have had an exaggerated cortisol response. Various studies suggest that patients with septic shock who fail to clear cortisol from the circulation (due to tissue defects in uptake and binding) have a higher mortality rate compared to patients who metabolize cortisol at normal rates21-22. Very high cortisol levels may also have been markers of severe disease. Eosinophilia was associated with FAI in our study, similar to the findings in other studies23, 24. Rothenberger describes the mechanism of eosinophilia as a result of decreased transition time of eosinophils to peripheral tissues when there is diminished expression of adhesion and ligation factors during states of hypocortisolemia25. One of the limitations of this study was the lack of corticotropin stimulation testing. Patients with a stress cortisol response to critical illness of < 25µg/dl may have an adequate adrenal response if corticotropin stimulation testing is done and therefore provocative adrenal testing would be required in some critically ill patients with low basal cortisol concentrations. Definitive etiologies of FAI were also not determined due to limitation of available investigations. Ideally, we would have liked to compare persons with the same disease severity, with and without FAI. We considered several clinical measures of the extent of disease. However, it is challenging to control for disease severity accurately and this limitation may explain the association of greater cortisol levels with mortality. In conclusion, we believe that critically ill HIVinfected patients in our setting who are using rifampicin or who have unexplained eosinophilia could be evaluated for FAI using a single morning total serum cortisol assay. Prompt assessment and treatment of critically ill HIVinfected patients should be expedited in order to reduce mortality rates. Finally, further studies are needed to investigate the role of corticosteroids in critically ill HIVinfected patients with risk factors for adrenal insufficiency in this setting. AcknowledgementsAll the listed authors have no commercial or other association that would pose a conflict of interest. Financial support for this study was obtained in part from the Academic Alliance for AIDS care and prevention in Africa and the Fogarty International Center- Ellison Foundation Overseas Fellowship through the AIDS International Training and Research Program at Case Western Reserve University, NIH Research Grant D43 (TW00011). References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07020t2.jpg] [hs07020t1.jpg] [hs07020t4.jpg] [hs07020f1.jpg] [hs07020f2.jpg] [hs07020t3.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}