 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
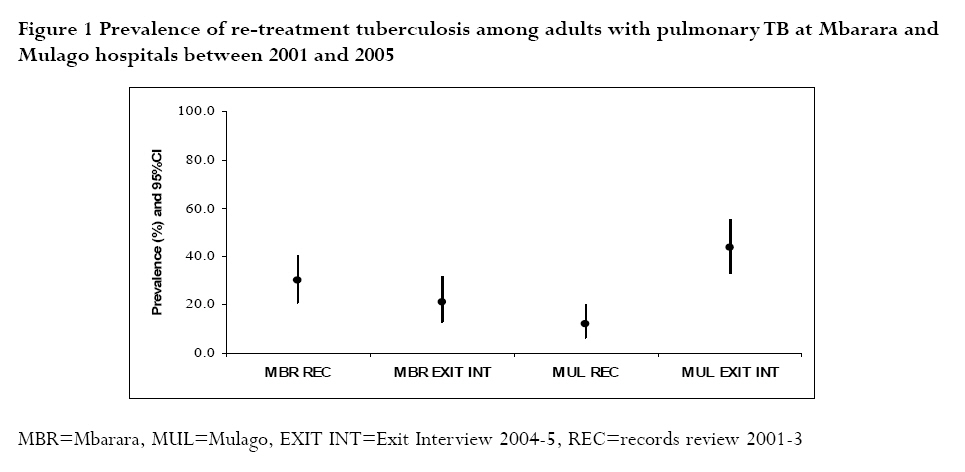
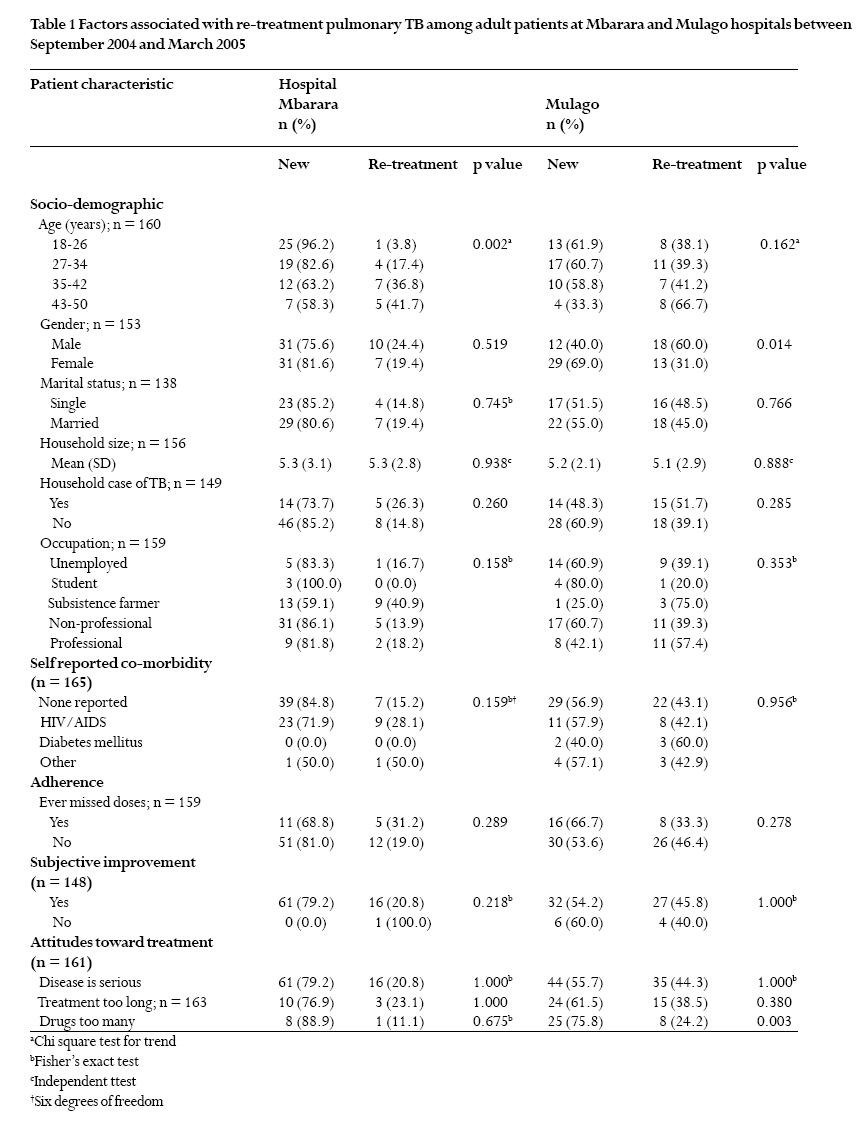
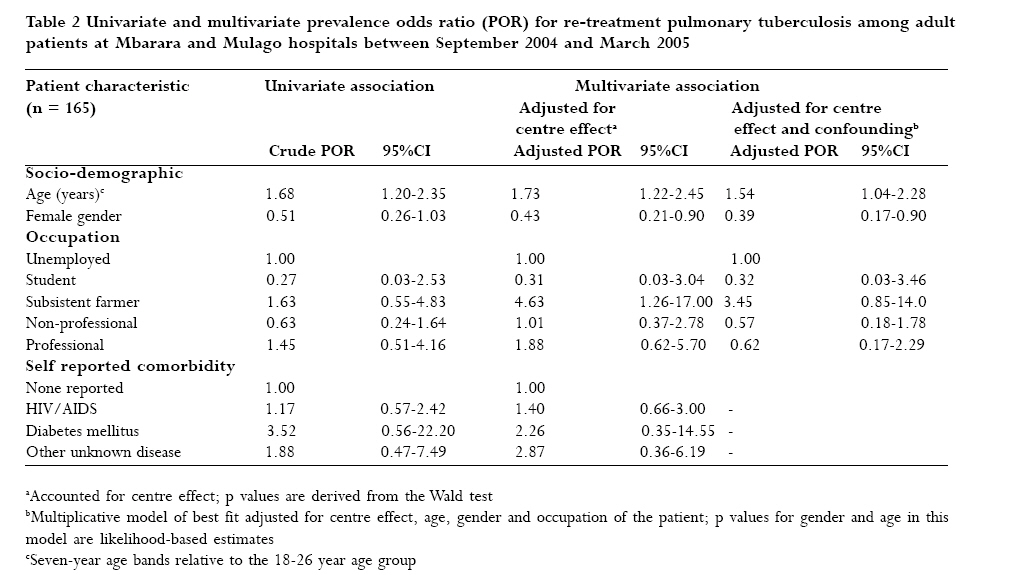
African Health Sciences, Vol. 7, No. 3, June, 2007, pp. 136-142 The challenge of re-treatment pulmonary tuberculosis at two teaching and referral hospitals in Uganda Norbert Anyama1, Simon Sseguya1, Alphonse Okwera2, Wael A El-Naggar3, Fred Mpagi4, Erisa Owino1 1Department of Pharmacy,Faculty of Medicine, Makerere University, Uganda, 2Tuberculosis Treatment Centre,Department of Medicine, Mulago Hospital, Uganda, 3Department of Microbiology, Faculty of Pharmacy, Mansoura University, Egypt, 4Department of Medicine, Mbarara Hospital, Uganda Author for correspondence: Norbert Anyama, Department of Pharmacy, Faculty of Medicine, Makerere University, Uganda. Email: nanyama@med.mak.ac.ug. Tel: 256-41-532389 Code Number: hs07028 Abstract Background With an annual tuberculosis (TB) incidence of about 350 cases per 100,000 of the population, Uganda is a high burden country. Moreover, it is evident that some TB patients have been treated for a previous episode of the disease. Keywords Tuberculosis, pulmonary, re-treatment, prevalence Introduction Tuberculosis (TB) remains one of the leading causes of ill health and death in developing countries, where comorbidity with human immunodeficiency virus (HIV) has increased the disease burden. With an estimated annual incidence of 350 new cases per 100,000 of the population, Uganda is one of the high-burden Sub Saharan countries in the world.1 The TB treatment strategy in the country is predominantly community-based directly observed treatment with short course chemotherapy (CB-DOTS) and is free of charge. Early detection of TB and expeditious antituberculosis chemotherapy are critical for effective TB control2. The target is to achieve at least 70 percent detection of sputum smear positive cases and to successfully treat 85 percent of patients1,3. In Uganda, the case detection rate is reported to have dropped below 50 percent and treatment success, approximately 68% of sputum smear positive cases1,4,5. Moreover, it is evident that some TB patients at Mbarara and Mulago teaching and referral hospitals have been treated for a previous disease episode. The problem of re-treatment TB has also been highlighted elsewhere6-8. Re-treatment tuberculosis Re-treatment is inevitable for patients with recurrent TB, those who defaulted on previous therapy and in cases were initial treatment has failed. In 2004, approximately 891 (2.0%)5 case notifications in Uganda were reported as re-treatment cases with the exclusion of relapse. However, the case classification and pathogenesis of recurrence are still obscure9-11. In general terms, recurrence of TB may be a result of relapse in patients otherwise previously treated successfully, or reinfection. Many studies12-15 indicate that a significant proportion of recurrent TB may be attributable to relapse with the same Mycobacterium tuberculosis strain, particularly following recent completion of treatment. Lambert et al9 in a systematic review suggest that reinfection per se may have few implications for TB control except in settings with considerably high incidence, while immunocompromised patients are reported to be at greater risk of re-infection TB16 Poor patient compliance, increasing age, emergence of multi drug resistant mycobacteria, comorbidity and chronic alcoholism6,17-19 have been associated with re-treatment. Additionally, HIV seropositive patients have generally been shown to have more frequent episodes of recurrence12,14,20,21 compared to seronegative patients. We carried out a study to highlight the burden of re-treatment pulmonary TB and to examine patient factors associated with re-treatment at two teaching and referral hospitals, Mulago and Mbarara. Mulago hospital is a 1,500 bed national referral hospital located in Kampala, in Central Uganda, while Mbarara hospital has about one-fifth the capacity of Mulago and is a regional referral hospital in the South Western part of the country. These hospitals are active TB treatment centres and about 50 percent of TB patients attending clinics have HIV coinfection. Methods Study design and participants This was a cross sectional design involving review of selected records and hospital exit interviews of a simple random sample of adult patients. Participants were new or re-treatment ambulatory patients attending TB clinics at Mulago and Mbarara hospitals, irrespective of the level of compliance to previous anti-tuberculosis treatment. We included patients who had been on treatment for four months or less and were aged 18-50 years. Patients with extra pulmonary tuberculosis and those who did not consent to the exit interview were excluded from the study. Data collection At Mulago and Mbarara hospitals, diagnosis of pulmonary TB is made on the basis of clinical examination, chest radiography and sputum smear microscopy. Following diagnosis, DOTS is initiated and supervised by health workers for institutionalised patients during the initial intensive phase, while CB-DOTS is undertaken in collaboration with family, community and health volunteers. Such CB-DOTS treatment supporters perform the duties of directly observing anti-tuberculosis medicine administration and of reminding patients to obtain refills. We systematically selected medical records from those archived between January 2001 and December 2003 for review of pulmonary TB cases. Sociodemographic, clinical, microbiological, and re-treatment data were extracted from 101 records at Mbarara hospital and 100 at Mulago hospital using structured forms. Eighty-two pulmonary TB patients were interviewed from Mbarara and 83 from Mulago hospital. Patient data, which was collected between September 2004 and March 2005, included socio-demographic characteristics, self-reported co-morbidity, drug treatment, and attitudes toward TB treatment. We considered a patient with re-treatment pulmonary TB as one who had been previously treated for TB but subsequently determined by a clinician as having active pulmonary TB and commenced on antituberculosis therapy. This non-specific definition included cases of relapse, re-infection, re-treatment TB after failure and re-treatment TB after default.A new TB patient was defined as one who had never received treatment for TB; relapse as a patient previously treated for TB and declared cured or who completed treatment, and was diagnosed with sputum smear positive TB; re-treatment TB after failure as a patient previously treated for TB but who remained sputum smear positive at five months or later during treatment; and, re-treatment TB after default as a patient previously treated for TB but who had interrupted treatment for two or more consecutive months22. Previous episodes of TB were ascertained from physicians’ cases notes or by reports of study participants. Data analysis We calculated the prevalence of re-treatment pulmonary TB based on records and patient interviews and computed binomial confidence intervals for these estimates. The frequencies of characteristics of interviewed patients were compared between the two hospitals. Furthermore, new TB patients and those on re-treatment were compared for socio-demographic and clinical characteristics, attitudes towards treatment and co-morbidity, including self-reported HIV serostatus. Factors associated with re-treatment were analysed using logistic regression. Initially, we accounted for centre effect and then examined confounding and effect modification through the inclusion of variables with a p-value of 0.2 or less during univariate analysis. The final model included only those variables found to be independent factors. A p value of 0.05 or less was considered statistically significant. Analyses were performed using STATA 8. Ethical considerations This study was approved by the Research and Ethics Committee of the Faculty of Medicine, the Institutional Review Boards of Mbarara and Mulago hospitals and registered with the Uganda National Council for Science and Technology (UNCST). Results Prevalence of re-treatment pulmonary tuberculosis Figure 1 shows the prevalence estimates of re-treatment pulmonary TB. Prevalence from exit interviews was lower at Mbarara hospital and higher at Mulago hospital. episodes, recurrent illness most often occurred within Although few records reported the time eight months of the previous disease episode; 15 (83.3%) interval between previous and current pulmonary TB at Mbarara and 12 (80.0%) at Mulago hospital. Factors associated with re-treatment pulmonary tuberculosis Table 1 shows the association between sociodemographic, clinical and treatment-related factors and re-treatment pulmonary TB in adult patients. Re-treatment pulmonary disease was more frequent amongst older patients at Mbarara hospital. Males at Mulago hospital were also more likely to have had a previous episode.Additionally, new pulmonary TB patients at Mulago hospital’s TB unit were significantly more likely to point out a greater pill burden compared to previously treated patients. Amongst the re-treatment pulmonary cases, 5 (29.4%) at Mbarara and 14 (38.9%) at Mulago pointed out that they did not complete their previous antituberculosis treatment. Univariate and multivariate prevalence odds ratios (PORs) for socio-demographic characteristics and comorbidity are presented in Table 2. Univariate analysis indicated a significant association between age (POR = 1.68; 95%CI: 1.20-2.35; p = 0.002) and re-treatment pulmonary TB.After partial adjustment for centre effect, increasing age remained significant (POR = 1.73; 95%CI: 1.22-2.45; p = 0.002) while female gender was protective (POR = 0.51; 95%CI: 0.21-0.90; p = 0.025) against re-treatment. Furthermore, subsistence farmers were 4.63 fold (95%CI: 1.26-17.0; p = 0.021) more likely to have re-treatment TB compared to unemployed patients. Multivariate analysis with adjustment for occupation and centre effect showed that increasing age and male gender were independently associated with re-treatment pulmonary TB amongst adult patients. Compared to the 1826 year age category, the prevalence odds ratio for a seven-year increase in age was 1.54 (95%CI: 1.04-2.28; p = 0.027), while female patients were 0.39 (95%CI: 0.17-0.90; p = 0.025) times less likely to have re-treatment disease than males. Discussion Re-treatment pulmonary TB accounted for 12 to 44 percent of cases, with different estimates of prevalence derived from records and patient interviews at Mulago and Mbarara referral hospitals. Prevalence based on exit interviews might have been influenced by the frequency of hospital visits of re-treatment cases compared to new patients. The record of patients attending the TB clinic is enumerated once, while at any one time, a patient who was previously registered could have visited the facility during the time of the study. If patients with re-treatment TB visit the facility more often because of the need for more frequent clinical and microbiological assessment, then there is a possibility that the prevalence estimate could be slightly higher. Conversely, if treatment seeking habits of re-treatment cases are poor, then the prevalence, based on interviews would correspondingly appear low compared to that derived from medical records. Nevertheless, re-treatment TB appears to be of major concern, making an important contribution to the burden of pulmonary disease at the two hospitals.This particularly raises questions regarding the effectiveness of TB treatment and patient follow up at lower levels of care. We broadly defined re-treatment pulmonary TB to include treatment failure, default and recurrence, as it was not possible to distinguish between these categories in the design. Appropriately applied, TB treatment is often efficacious and failure rates, low. However, some patients default on their therapy. In 2003, 0.4 percent of TB patients in Uganda were reported to have failed treatment, 19 percent were reported to have defaulted on treatment5, while the contribution of recurrence is not well quantified. One study based in Uganda by Johnson et al23 found a relatively low recurrence rate of 3.1 per 100,000 person years, which rate was influenced by HIV co-infection. However, this recurrence rate was for a nine-month rifampicin containing regimen while the current standard treatment for a new case of pulmonary TB is an eight-month ethambutol-containing regimen. In addition, close monitoring for adherence and exclusion of patients who did not complete treatment make this estimate less pragmatic. Recurrences of pulmonary TB have been reported to be especially more frequent among HIV-infected patients with low CD4 lymphocyte count8,24 and in carriers of homozygous haptoglobin with residual lung changes following initial disease episodes25. However the latter findings have not been adequately corroborated. One could argue that the short interval between TB episodes suggests that a majority of patients previously defaulted or had a recurrent TB episode arising from relapse of the previous infection.This is further supported by the relatively high proportion of patients with re-treatment pulmonary TB who reported not having completed their previously prescribed therapeutic regimen. In this study, older adult males were more likely to report re-treatment pulmonary TB. Male patients however, were less likely to report HIV co-infection. Older adult male patients might have therefore been more likely to default on previous TB treatment, and also at greater risk of recurrence. However these findings may also suggest poorer help seeking behaviour among female patients with re-treatment TB. Relapse per se, is said to occur if there is insufficient bacteriological cure of previous disease. It can be considered a measure of the efficacy of the antituberculosis drug regimen having accounted for other patient and health system factors6 Connolly et al26 found a 5 percent frequency of relapse at 18 months following DOT regardless of HIV co-infection and previous treatment history, while the rate of sputum smear conversion was not predictive of relapse.Various influences have been reported to increase the risk of recurrence due to relapse; poor treatment regimens, for example those formerly involving thiacetazone23, too short a duration of treatment, primary or acquired drug resistance9,27,. The high frequency of re-treatment amongst older patients in this study is expected, but also suggests that re-infection may have a role to play. There is an increase in the risk of new infection with age in this high incidence setting. Moreover, HIV infection together with progressive immuno-suppression with age, which is common among TB patients, increase the rate of breakdown to active disease following re-infection with mycobacteria16. Of particular concern are settings where the background risk of infection or re-infection is high or among very close contacts of infectious index cases28. This underscores the significance of spatial clusters in re-infection TB. A systematic review of studies on recurrent TB by Lambert et al9 indicated that the proportion of recurrences due to re-infection could be at both extremes (0 to 100 percent), with its importance varying by setting. Notable from our findings was that the presence of a known household case of TB was not associated with re-treatment. However, it is possible that patients were not aware of a case of TB in the household since case detection is on the basis of passive reporting other than active surveillance to identify contacts with the disease. More robust evidence on re-treatment and recurrent TB can be obtained by a prospective analysis with repeat clinical and microbiological assessments and adjustments for various patient, treatment-related and health system factors. Molecular identification of mycobacterial strains would be necessary to examine the significance of relapse, re-infection and mixed infections29. In addition, the contribution of primary, acquired and extensive antimycobacterial drug resistance is of considerable interest. Limitations No data were readily available on repeat sputum smears. Therefore, the proportion of re-treatment TB attributable to treatment failure could not be quantified. However, pulmonary TB patients were reported to normally “dry up” quickly, implying that production of sputum ceases soon after initiation of treatment. Treatment failure therefore appears to contribute little to the problem of re-treatment TB. Another drawback was that we could not ascertain recurrence using molecular techniques because of the cross sectional design and the lack of historical data on mycobacterial strains. Conclusion Re-treatment pulmonary TB is frequent at the two teaching and referral hospitals. It is therefore of public health concern and efforts should be geared towards its prevention.The need for rigorous management of new TB cases should be re-emphasised, particularly at lower levels of care. Furthermore, potential benefits of long-term follow up of previously treated patients at risk of requiring TB re-treatment should be explored. Acknowledgements The study was funded by Sida/SAREC through the research programme of the Faculty of Medicine, Makerere University. We thank Sam Nyole and staff members at tuberculosis units and records departments of Mulago and Mbarara hospital. We also acknowledge the research assistance from Amos Atumanya and Assumpta Nakalanzi References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07028t1.jpg] [hs07028f1.jpg] [hs07028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}