 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
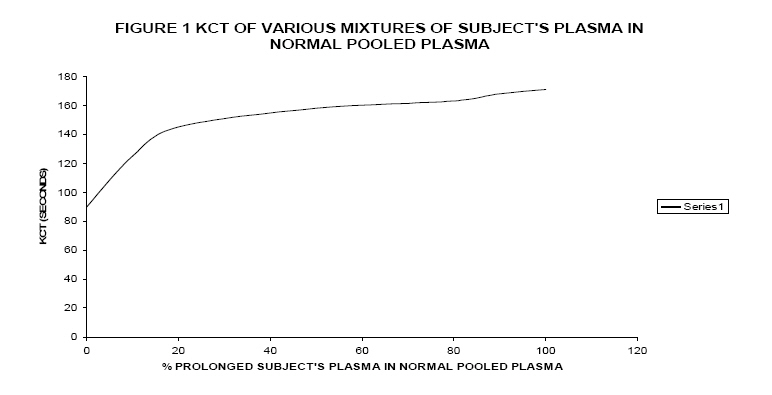
African Health Sciences, Vol. 7, No. 3, June, 2007, pp. 182-184 Presence of lupus anticoagulant in an asymptomatic Nigerian * Edeghonghon E. Olayemi, ** Godwin N. Bazuaye *Department of Haematology and Blood Transfusion, OACHS, Olabisi Onabanjo, University, P.M.B. 2022, Sagamu, Ogun State. Nigeria, ** Department of Haematology and Blood Transfusion, University of Benin Teaching Hospital, P.M.B.1111, Benin City, Edo State. Nigeria Correspondence author: Olayemi, Department of Haematology and Blood Transfusion, OACHS, Olabisi Onabanjo University, P.M.B. 2022, Sagamu, Ogun State. Nigeria. Email: yemiede@yahoo.com Code Number: hs07035 Abstract Background:The lupus anticoagulant (LA) is one of the antiphospholipid antibodies (aPL), which prolong phospholipid- dependent coagulation tests by interfering with coagulation reactions that depend on protein - phospholipid complexes in vitro. Introduction The lupus anticoagulant (LA) is one of the antiphospholipid antibodies (aPL), which prolong phospholipid- dependent coagulation tests by interfering with coagulation reactions which depend on protein - phospholipid complexes in vitro1 ; isotypes include immunoglobulin G (IgG), immunoglobulin M (IgM), immunoglobulin A (IgA) or combinations of these 2. The presence of the lupus anticoagulant has been associated with certain clinical manifestations such as recurrent abortions, arterial and venous thrombosis, and thrombocytopenia3. Cutaneous symptoms of this syndrome include leg ulcers and livedo reticularis4. Neurological disorders such as dementia, epilepsy, chorea and migraine5 can also occur. The first antiphospholipid antibody was detected in patients with syphilis in 19066 while the lupus anticoagulant (LA) was first described in 19527. The most commonly detected antiphospholipid antibodies are lupus anticoagulant, anticardiolipin and anti-beta 2 glycoprotein 1(â-2GP- 1) antibodies1 . LA antibodies are identified by coagulation assays, in which they prolong clotting times while anticardiolipin and anti â-2GP-1 antibodies are detected by immunoassays that measure immunologic reactivity to a phospholipid or a phospholipid - binding protein. Current criteria for detection of LA antibodies include prolongation of at least one phospholipid - dependent coagulation assay1.KCT has been shown to have a specificity of up to 93% for LA 8 and it is able to detect LA at a much greater dilution in normal plasma than the tissue thromboplastin inhibition test (TTI) or the dilute Russell’s viper venom time (DRVVT )9. KCT is also more sensitive to the presence of LA than TTI10 . Case Report O.U. a 25 year old male Nigerian who was a final year student in one of the universities in the south-south geopolitical zone of Nigeria; volunteered to have his plasma used to prepare normal pooled plasma in a study approved by the University of Benin Teaching Hospital ethics committee. As a pre-condition to having his plasma pooled along with those of other volunteers we had to carry out tests to ensure that he did not have any clotting abnormalities, this included platelet count, prothrombin time (PT) and kaolin clotting time (KCT). It was during this that he was detected to have a prolonged KCT and slightly prolonged PT. On further investigation O.U has lived a relatively healthy life, there was neither any past history of thrombosis nor family history of thrombosis, both parents and all his siblings are alive and well. The patient had not been previously transfused; he is not a known epileptic neither has he ever suffered from migraine headaches. He has never taken any drug such as phenytoin or chlorpromazine which have been associated with LA. On general examination he was a healthy young man, he was not pale, was afebrile and anicteric, he had no lymphadenopathy, did not have any petechiae or echymotic spots. His chest was clinically clear, pulse rate was 78/ minute, regular and of good volume. Only the first and second heart sounds were present and his blood pressure was 110/70 mmHg. No abdominal organs were palpable. He had no neurological deficits. Method and Reults Kaolin clotting time (KCT) was performed as described previously11,12 .The procedure was carried out in duplicates and the average was taken as the clotting time. Due to the prolonged KCT, we decided to carry out mixing tests on his plasma using the KCT; in the following proportions of normal plasma (NP) and subject’s plasma (SP). NP/SP: 100/0, 90/10, 80/20, 50/50, 20/80, 10/90 and 0/100 as earlier described 12 . he KCT index, which is the ratio of KCT at 20% subject plasma to KCT at 100% normal plasma was then calculated as shown below.
A ratio of greater than or equal to 1.2 was taken to signify the presence of LA12. Normal KCT and PT in our laboratory is 60-110 seconds and 10 -14 seconds respectively. Results of laboratory investigations carried out are shown in table 1. A graph of KCT of various mixtures of SP in normal pooled plasma was also plotted, this curve was convex in the left axis, and in keeping with earlier studies by Exner et al 11, such a shape is suggestive of the presence of LA ( Figure 1). Table 1: Results of Laboratory Investigations
Figure in brackets is the repeat laboratory investigations after 3 months Discussion LA is commonly associated with patients who have systemic lupus erythematosus (SLE) and other autoimmune disorders, though recently, it has been shown that LA may be responsible or at least play a significant role in recurrent foetal loss. LA and other aPL have been previously described in asymptomatic subjects from other parts of the world. In fact, it has been said that up to 2% of the normal population may be positive for aPL and it is not known what percentage of this would go on to develop thrombosis or other signs and symptoms of antiphospholipid syndrome (APS); though only about 0.2% have high titres13. Like other autoantibodies, prevalence increases with age14 .LA has been described in children15 . In patients with SLE, the prevalence of aPL is much higher, ranging from 12-30 % for anticardiolipin antibodies16 and 15-34 % for LA 16,17. In our environment, LA has been described in women with pre-eclampsia 18; multiparous women 19, as well as in sickle cell disease patients 20; we believe that this is the first time LA is being reported in an asymptomatic male Nigerian. Patients may have laboratory evidence of aPL without clinical consequences 1.The presence of LA in a healthy subject may lead to confusing results of the clotting profile as the presence of LA is known to be capable of prolonging the PT, APTT, KCT and other measures of haemostasis.Also it may lead to endless and often expensive investigations in an attempt to uncover the presence of APS, SLE or other cause. It is for these reasons that we are reporting this case to create awareness of this possibility in our environment and save otherwise healthy patients from unnecessary laboratory investigations and anxiety. Three months after the subject was detected as having LA, his KCT was still prolonged with an index of 1.4 (Table1). However he has remained healthy and has since completed his tertiary education and is currently in paid employment. In conclusion, LA has been described in healthy subjects from other parts of the world we have here reported its presence in a healthy male Nigerian. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07035f1.jpg] |
| |||||||||


{kind=link}