 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 7, No. 4, December, 2007, pp. 197-201 Outcome of a working diagnosis of "psychosis" in relation to DSM-IV diagnostic criteria in a Kenyan in-patient cohort at Mathari hospital, Nairobi *David M Ndetei1, Lincoln I. Khasakhala1, Francisca A. Ongecha2, Victoria Mutiso1, Donald A. Kokonya3 1. Department of Psychiatry, University of Nairobi, Kenya, Africa Mental Health Foundation (AMHF) This work should be attributed to: The Department of Psychiatry, University of Nairobi and the Africa Mental Health Foundation Code Number: hs07039 AbstractBackground: When a patient presents with mental illness and displays psychotic symptoms which are not clearly delineated, a
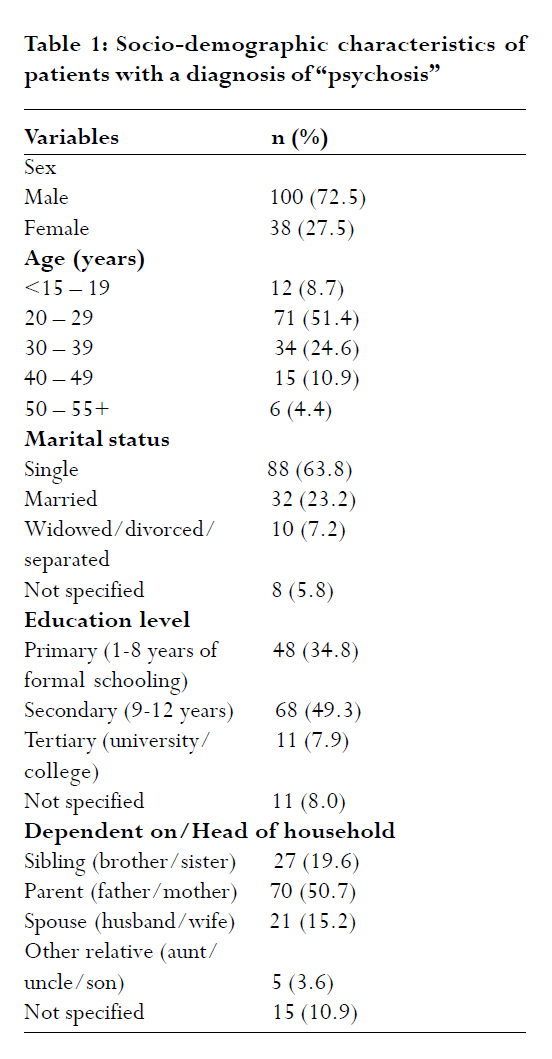
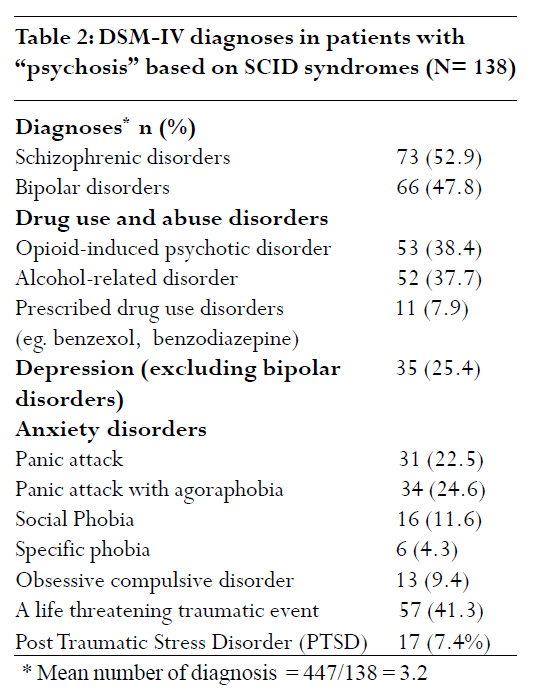
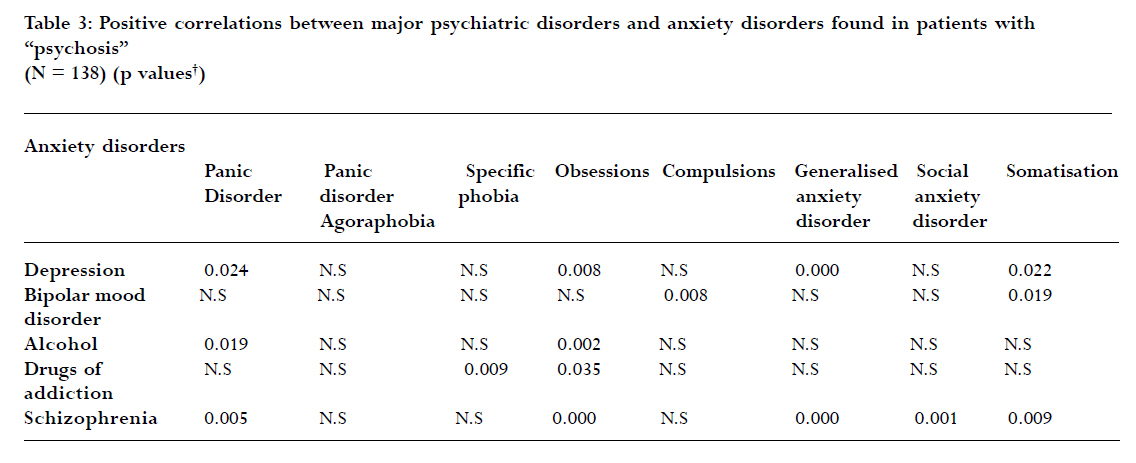
clinical diagnosis of psychosis is usually entertained. Introduction It is important to make reliable working diagnoses of schizophrenia and other disorders at first presentation because early treatment and psycho-education of patients and their families may improve the course of the illness 1-3. However, in practice, this may not be final at first presentation: it may, in fact, be difficult to elicit reliable clinical diagnostic information at the initial interview; also, psychiatric disorders tend to be pathoplastic and their presentations may change over time in the same patient. This has been shown to be the case, even in well endowed psychiatric facilities. For example, Veen et al.4 in a Dutch study found that up to 49% of the patients with an initial diagnosis of psychosis rather than schizophrenia were diagnosed with schizophrenia 30 months later. A working diagnosis of "psychosis" is common at Mathari hospital and is made on patients when the definitive diagnosis is not clear, mainly for the reasons mentioned above. No systematic study has been carried out in Kenya to delineate the specific Diagnostic and Statistical Manual of Mental Disorders-Fourth edition (DSM—IV)5 diagnoses in the patients who are given this clinical diagnosis of "psychosis." This information is useful in facilitating an early definitive diagnosis and initiating early appropriate treatment. Making a proper first diagnosis is also critically important in a human resource set-up with limited psychiatric services where it is junior doctors who perpetuate the initial diagnosis. There are several but complementary ways to do this. Improvements in diagnostic practice will assume that senior doctors will be available at all times, a situation which is unlikely because of a shortage of such doctors at Mathari hospital. Junior doctors need to be trained to make reliable diagnoses, but again, this is limited by the reasons previously discussed. A third and most cost-effective way is assisted diagnoses using diagnostic instruments/questionnaires. Methods Subjects All the inpatients at Mathari Hospital during the month of June who were able to give informed consent participated in the study. Considered for inclusion therefore, were all the patients admitted prior to and during the specified period. A total of 691 patients met these criteria. These patients were drawn from the city of Nairobi and its environs, which is the hospital's main catchment area. Although Mathari is the national referral hospital, availability of psychiatrists at all provincial hospitals means that there is hardly the need to refer patients from these units which are at a lower level than the national hospital. A major determinant for admission into the hospital was availability of bed space. This being the case, it was considered that since there would be no month on month differences in admission patterns, sampling patients admitted during one month would yield a representative sample. This was a cross-sectional descriptive study. It was explained to the patients that the study sought to describe the pattern and types of psychiatric disorders diagnosed at the hospital. The patients were also told that information would be extracted from their clinical notes and that they would undergo a session in which a detailed history would be taken in order to elicit their symptoms, as would be the case in an ideal situation. Clearance to conduct this study, which was basically aroutine clinical examination supplemented by an instrument to assist in a detailed and structured mental state examination, was sought and obtained from the Mathari Hospital Research Committee. Setting This study was conducted at the Mathari hospital which is a national, referral and teaching psychiatric hospital in Nairobi, Kenya. It is located about five kilometres (8 miles) from the centre of the capital city, Nairobi. The hospital is a 600-bed facility and one-third of the beds are designated for females. It is served by seven psychiatrists, two of whom carry out administrative duties. The hospital is a stigmatised institution that admits mainly those who are too disturbed to be managed within the community, and who cannot afford treatment at a private facility. Instruments A structured questionnaire was used to record the socio-demographic characteristics and details from clinical notes of the patients as obtained at the time of the admission. The hospital working diagnoses were also extracted from the clinical notes. Senior psychiatric charge nurses were first trained on the administration of the Structured Clinical Interview for DSM-IV (SCID) (6). This training was done for one day to ensure that the nurses understood the concepts of the instrument in both English and Kiswahili, two languages which are used interchangeably at the hospital during all clinical interviews. The use of the instrument was then piloted on patients who were not part of the main study so that the charge nurses could familiarise themselves with actual administration. Since this was a clinician-administered instrument, the nurses were able to ask the questions in a consistent manner for all the patients. Analysis of data The data were analysed using the Statistical Package for the Social Sciences (SPSS) version 11.5. Pearson's 2-tailed correlation tests were performed to establish correlations between the various DSM-IV diagnoses and psychotic disorders. Results Twenty percent (n = 138) of the 691 inpatients had a working diagnosis of "psychosis" as extracted from their clinical notes. The remaining patients had the following working diagnoses: Schizophrenia (n = 234, 33.9%), bipolar mood disorder (n = 159, 23.0%) and schizo-affective disorder (n = 29, 4.2%). No further results are presented for these other patients as this paper was focussed only on those patients who had a working diagnosis of "psychosis." The socio-demographic characteristics of the 138 patients with a working diagnosis of "psychosis" are summarised in Table 1. Up to 60.1% of the patients were aged below 30 years, 63.8% reported that they had never been married and all except 11 patients (who did not specify their education level) had attained different levels of education. Nearly 90% (89.1%) were dependent on another person for their livelihood. A similar diagnosis of "psychosis" had been made in 35.5% of the patients in a recent past admission. During the third, fourth and fifth previous admissions (starting with the most recent diagnosis), 12.3%, 7.2% and 2.2% of the patients, respectively, had the same diagnosis as the current one. The differential diagnoses that were made in the 138 patients included bipolar mood disorder (8.7%; n = 12), schizophrenia (10.1%; n = 14)), substance abuse disorder (3.6%; n = 5), adjustment disorder (2.2%; n = 3) and schizo-affective disorder, sexual abuse and epilepsy (each 0.7%; n = 1). No other diagnoses were made in the remainder of the patients. A summary of the DSM-IV diagnoses is presented in Table 2. There were 447 diagnoses made in 138 patients giving an average of 3.2 diagnoses per patient. This suggests co-morbidity of DSM-IV diagnoses in "psychosis" patients. The most commonly made DSM-IV diagnoses were schizophrenia, bipolar mood disorder, substance abuse disorders, depression and various types of anxiety disorders. Table 3 summarises the significant correlations between the major DSM-IV psychiatric, psychotic, substance abuse and anxiety disorders. Schizophrenia and depression were found to be the most frequently correlated with anxiety disorders. Discussion The inpatients included in this study were typical of patients admitted into public psychiatric facilities, not only in the rest of Kenya, but across other sub-Saharan African countries with similar socio-cultural contexts and resource-limited facilities. The findings of this study should therefore find clinical relevance in such similar countries. There are several caveats in the interpretation of these results, the most important of which is how a clinical diagnosis of "psychosis" is made. "Psychosis" is normally given by admitting doctors and psychiatrists as a working diagnosis when it is not clear what kind of disorder one is dealing with. This means that the diagnosis is not necessarily made on the basis of an acute or transient psychosis disorder (ATPD) as defined by the International Classification of Diseases-version 10 (ICD-10) 7 or the DSM-IV, both of which are different. Some of the reasons for this working diagnosis of "psychosis" have been mentioned under the introduction. All these, together with potential steps to minimise this diagnosis, underline the need for a minimum standard of clinical practice that ensures that working diagnoses are made on the basis of diagnostic criteria, which should be elicited to support whatever working diagnosis is made. Front line clinicians making the first diagnostic impressions should therefore have sufficient background information that they need in taking psychiatric history, making appropriate mental status assessments and documenting these in patients' clinical files. However, while this is possible in resource-sufficient centres, the same may not be so in resource-limited centres and therefore the need for routine use of structured clinician-administered check lists that assist in diagnosing disorders in patients. These structured check lists should be used in all the patients by the clinicians (including nurses) and administered serially in order to monitor changes in the clinical patterns in the same patient. Such objective instruments are cost-effective after the initial training of the ward personnel. However, it is important to emphasise complementary and not exclusive use of such check lists in making diagnoses. The second major caveat is that in the Kenyan context, with a dearth of mental health resources, most patients on their first visit to Mathari hospital will be making contact with psychiatric services for the first time although they may have visited other non-mental health professionals. No formal referral system exists so patients, or mainly relatives, determine the need for admission mainly on the basis of inability to cope at home or being unable to afford private treatment. This means that a patient could be suffering from an undiagnosed mental disorder for a much longer time than that set in the ICD-10 or the DSM-IV. The ICD-10 specifies a 2-week period of onset of ATPDs while the distinguishing feature in the DSM-IV is a less than 6-month duration of psychosis. As a result, there is a limitation on the comparison that can be made between the findings from this study and reports that relied on the ICD-10 criteria for ATPD. However, there is little empirical evidence to justify the duration of onset and remission criteria used to delineate acute non-affective psychoses in the two classification systems. The issue arising is not only the accuracy of the diagnoses according to the ICD-10 or the DSM-IV criteria, but the practical reality of the working diagnosis in a given contextual setting. The evidence hereby adduced is that clinicians in this and similar settings must be alert to the pitfalls of making such a diagnosis and the implications of using structured diagnostic instruments in clinical practice. Furthermore, the term ATPD refers to the mode of onset of the particular illness episode, its course and duration before full recovery. It is not clear whether or not clinicians making the diagnosis of ATPD take other illness features, such as symptom profiles and mental status examination findings into consideration at the time of making the diagnosis. There is therefore need to not only harmonise the ICD-10 and DSM-IV in future revisions, but also to take into account other symptom profiles, rather than merely the duration of the illness which in itself may be difficult to delineate precisely in all contexts. This Kenyan study highlights these concerns that do not seem to have been adhered to in current and past DSM-IV and ICD-10 criteria. Another caveat, which is pertinent to the Kenyan context and to those of similar developing countries, is the possibility of a diagnosis of organic psychosis in a situation where patients are likely to be taken to a mental health institution if mental disturbance is the only presenting complaint. Bearing in mind these caveats, the results provide a basis for clinicians to be proactive when handling patients with any mental disorders and whose presenting symptoms do not clearly fit into the ICD-10 or the DSM-IV diagnostic criteria. This could be done by either ruling out organic conditions at the first contact or using psychometrically sound screening tools (even for organic conditions) or diagnostic instruments/check lists to ensure comprehensive elicitation of all psychiatric symptoms. The next step would then be to initiate appropriate management of the condition at the earliest possible opportunity on the basis of having derived clinical features and evidence for any therapeutic approach. The target population for this study was relatively young, suggesting onset of psychosis at a young age. The predominance of male patients is a reflection of the disproportionate allocation of beds at the Mathari hospital. This anomaly could be corrected by making it possible for both genders to have equal access on the basis of demand rather than being restricted by pre-determined bed allocation. The finding that schizophrenia was a definitive diagnosis in 52.9% of the patients is similar to that of 49% found by Veen et al4. Some of the factors associated with psychosis found in this study have been reported in other studies: Substance use 8, 9, neurotic symptoms 9, 10 and adverse life events 10, 11. A high association was found in this study, between opioid-induced disorders and psychosis. This is not to suggest that clinicians in this hospital would equate opiate use with psychosis but rather that opiate use is co-morbid with psychotic conditions such as schizophrenia and severe mood disorders. Therefore, a comprehensive elicitation of all psychiatric symptoms in a patient will help in not only diagnosing all the co-morbid disorders and manage them accordingly at the earliest opportunity, but also in the process, improve the overall prognosis. The DSM-IV diagnoses made in this study are a significant finding as it has been reported elsewhere that provision of specialised care early on at the onset of psychosis can achieve better outcome3. It has also been reported psychosis which is left untreated for a longer duration is significantly associated with poorer functional and symptomatic outcome 4 years later, especially in relation to schizophrenia and schizophrenia form disorder12. This study showed that in addition to depression, mood disorder, schizophrenia and substance abuse disorders, there was a high prevalence of neurotic symptoms in patients with psychotic conditions. There are two possible explanations for these observations on co-morbidity. One is that the combined disorders are independent of each other in aetiology. The other is that they are a continuum or they are related with for example, anxiety disorders, pre-existing schizophrenic illness or anxiety caused to the patient by the symptoms of schizophrenia, especially in the early stages of schizophrenia. Conclusion Psychosis as a clinical diagnosis can lead to a delay in proper diagnosis and appropriate management. Attempts should therefore be made to elucidate the underlying psychiatric and physical conditions so as to initiate early treatment even in patients already admitted in a psychiatric hospital. Furthermore, the diagnosis of "psychosis" should not be used loosely for clinical management purposes. This study highlights the natural course and outcome of "psychotic" illnesses and any final diagnosis should not be made until after sufficient observation over an adequate period of time has been made. The presentation of mental illness follows an evolutionary and pathoplastic pattern and changes over time even for the same individual. This calls for a regular re-evaluation of the patient, aided by the use of a structured check list. Acknowledgements The Africa Mental Health Foundation (AMHF) provided financial, administrative and logistical support for this study. The authors would like to thank Grace Mutevu of AMHF for analysis of the data and preparation of the paper, and Patricia Wekulo for editing the paper. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07039t1.jpg] [hs07039t3.jpg] [hs07039t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}