 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 7, No. 4, December, 2007, pp. 214-222 The sensitivities to first-line antibiotic therapy of the common urinary tract bacterial infections detected in urine samples at a hospital in metropolitan Kampala (Uganda) 1Kyabaggu D, 2Ejobi F 3*Olila D 1Faculty of Veterinary Medicine, Makerere University, P.O.Box 7062,Kampala; Code Number: hs07041 Abstract Background: Urinary tract infections (UTIs) are among the most common human infections. Many urinary tract bacteria are
capable of expressing drug resistance. Resistant bacteria may be present from the commencement of the infection or may develop
during treatment. This study focused on the problem of antibiotic resistance to the first-line drugs that were used to treat patients
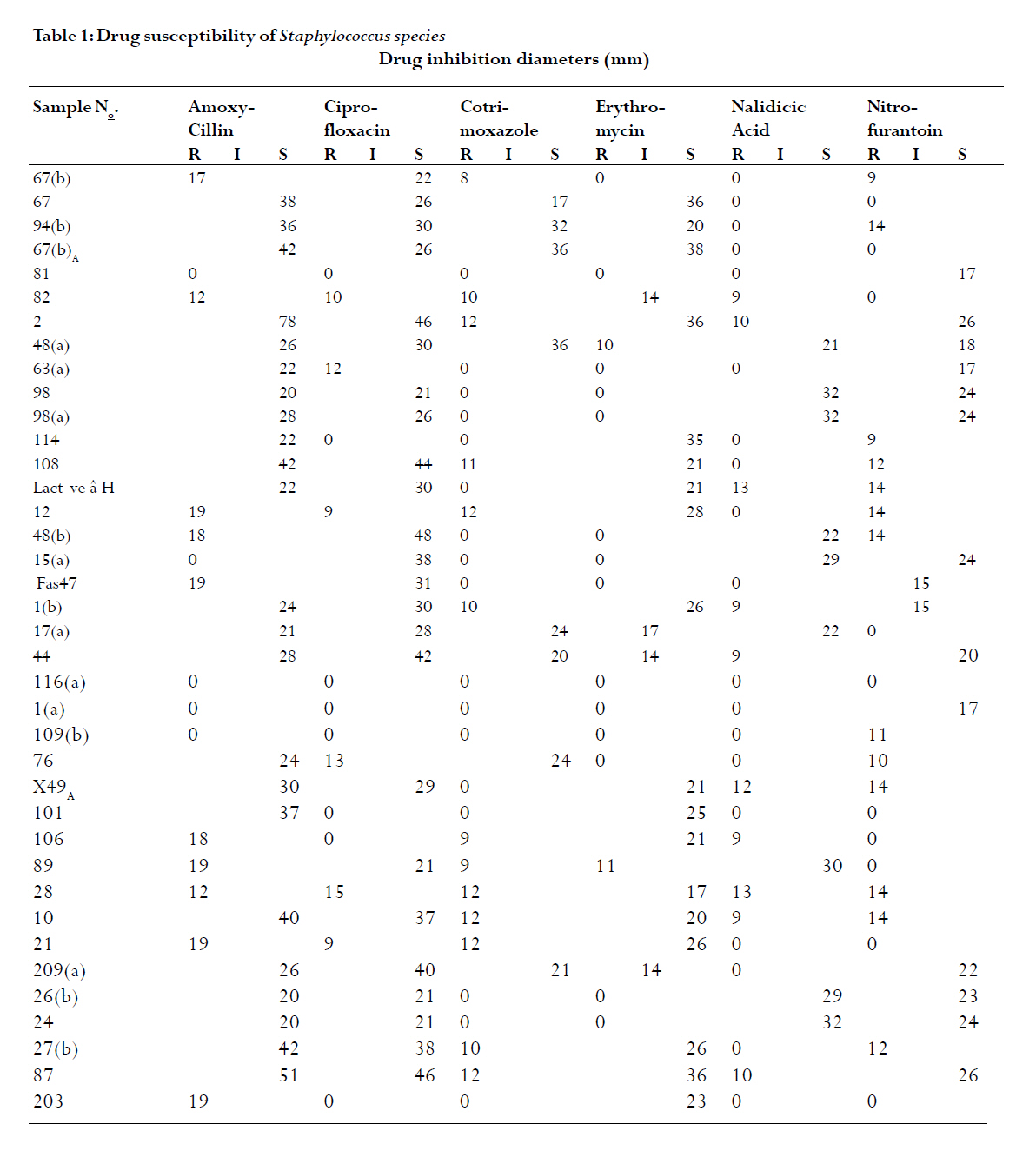
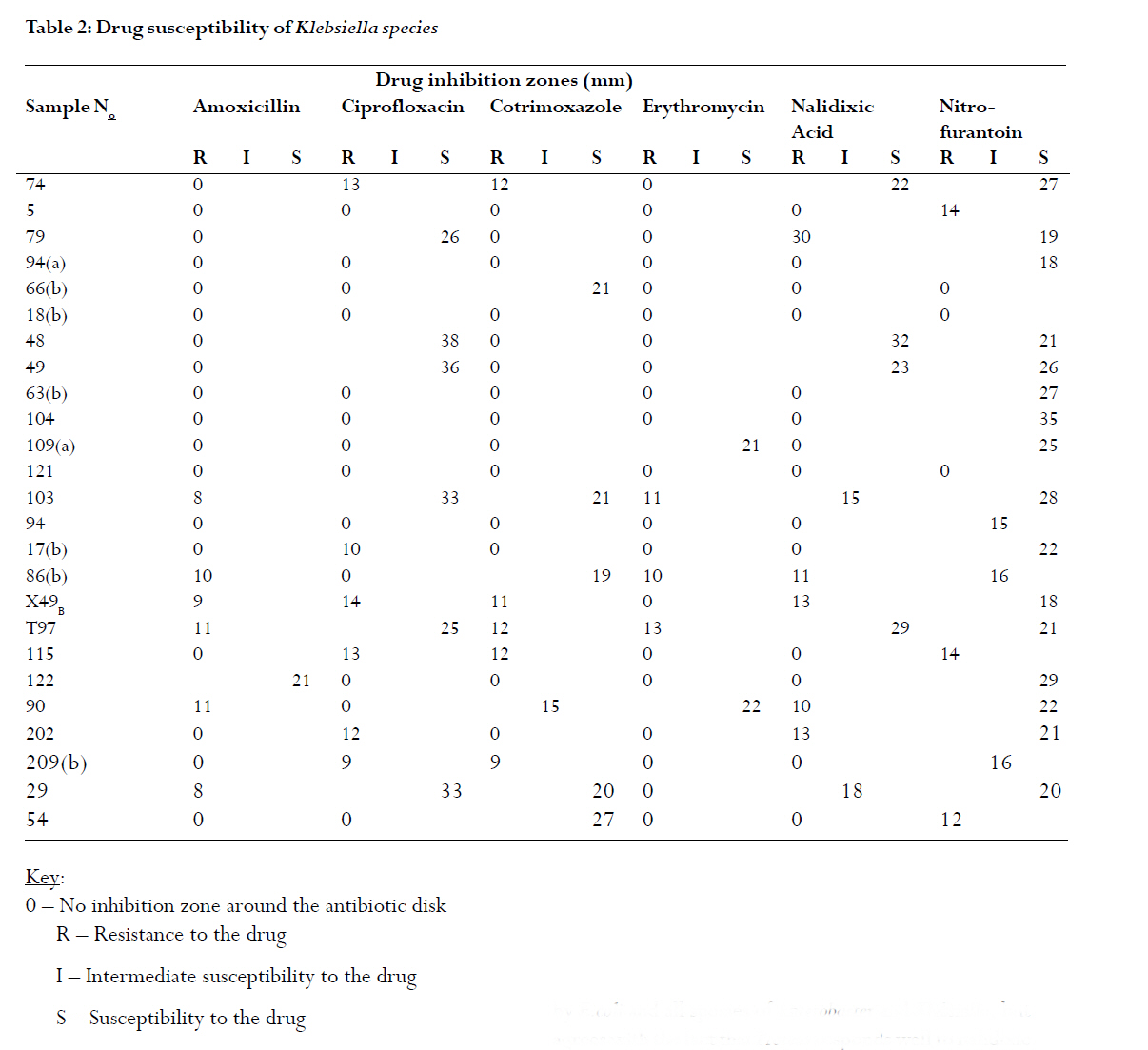
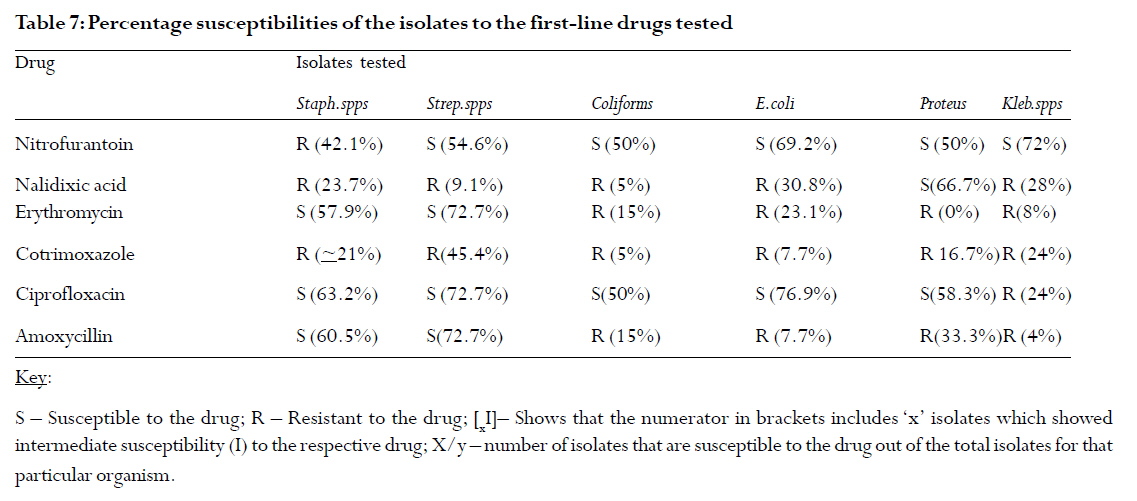
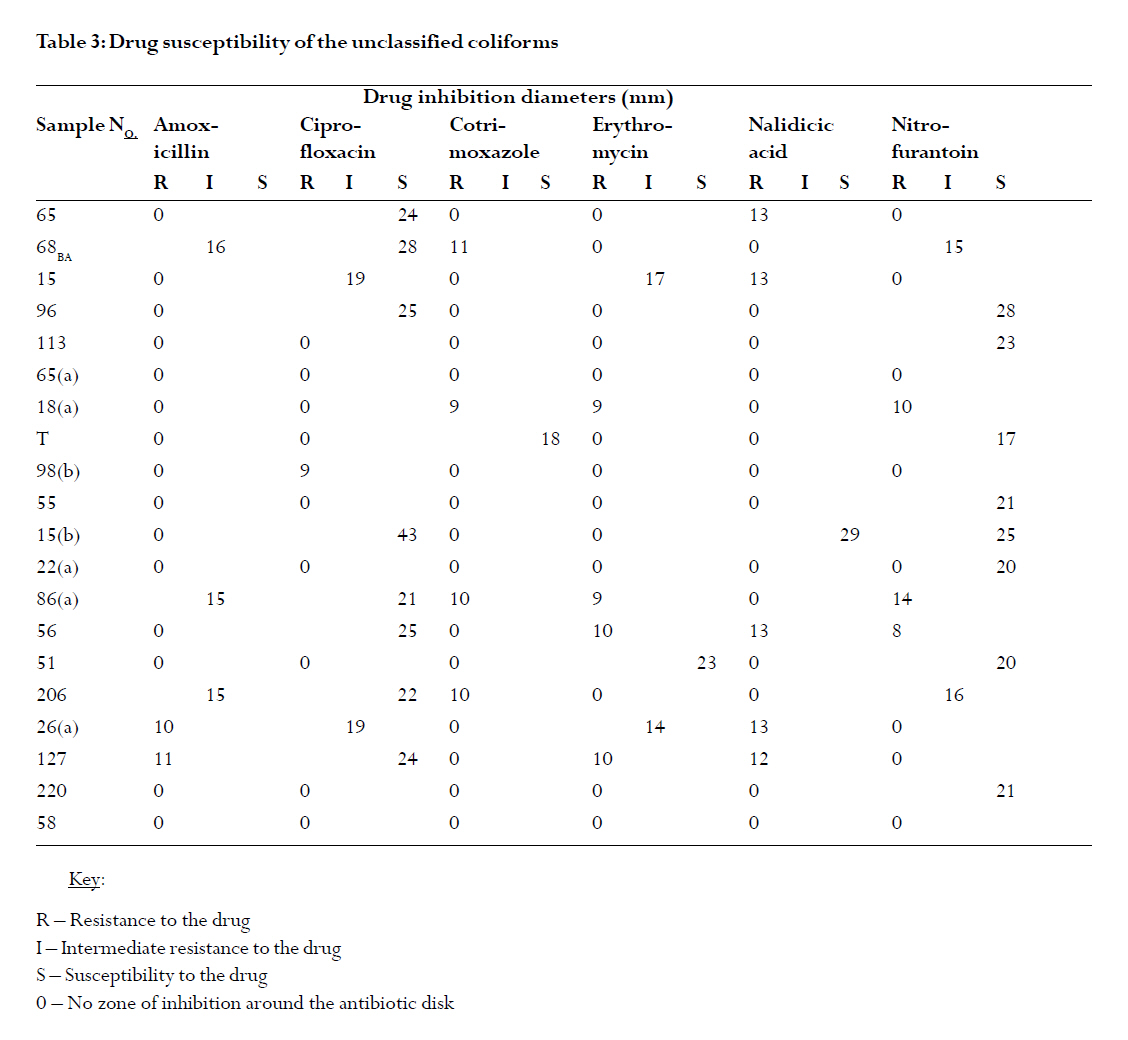
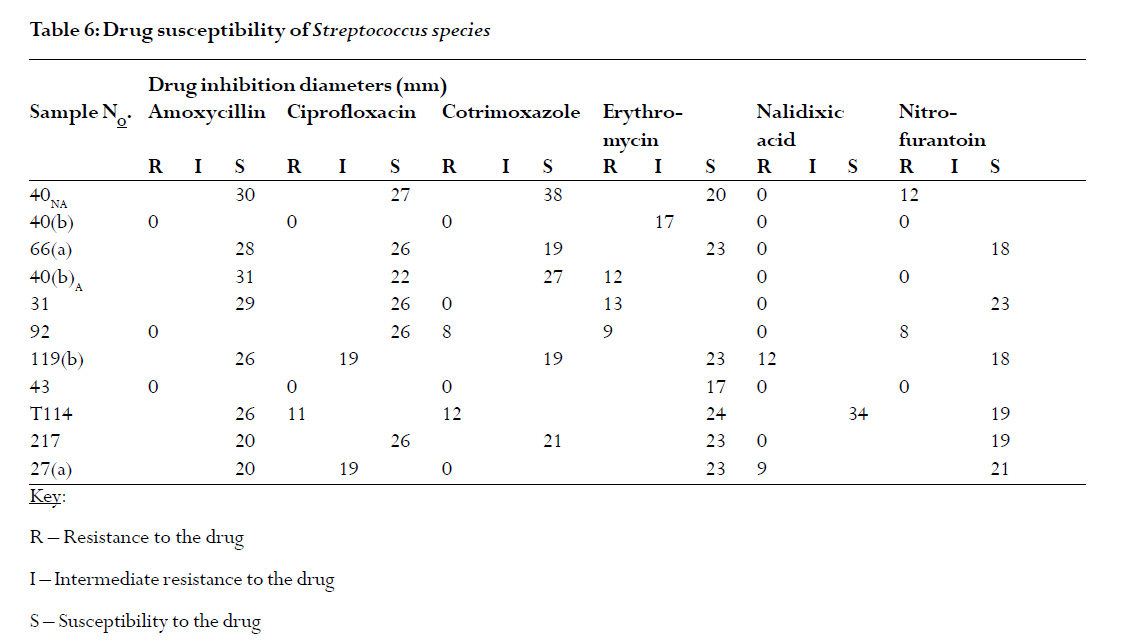
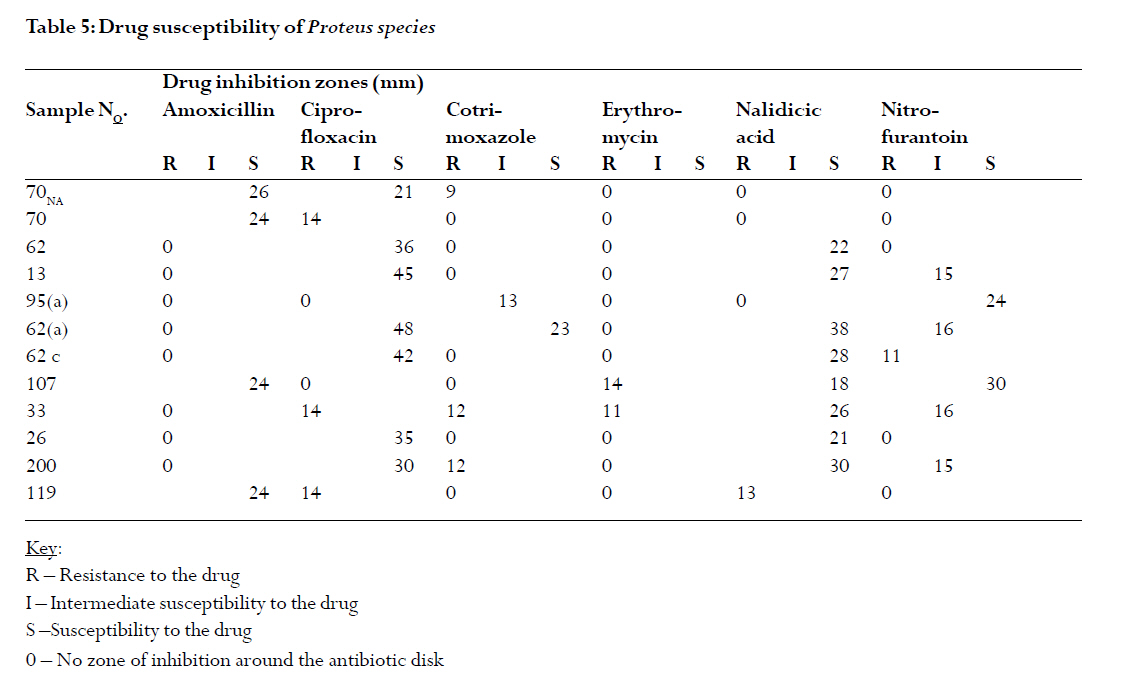
presenting with urinary tract infections at Rubaga hospital in Kampala, Uganda. Keywords: Urinary Tract Infections (UTI), resistance, drug sensitivity, ciprofloxacin, nitrofurantoin Introduction Urinary tract infections (UTIs) are among the most common human infections. In an average practice of 2000 patients, approximately 50 will consult annually for acute urinary tract infection1. Certain persons seem to be particularly susceptible to UTIs. In some cases this may be the result of anatomic abnormalities, but there is no plausible explanation in others2. The female appears to be much more prone to such infections than is the male. This can probably be explained by the shorter urethra in the female2. About 20% or more of women have asymptomatic UTI at least once; and beyond the age of 6 months, UTI is much less common in males than in females1. It becomes more common in older males due to obstruction of urinary outflow related to prostatic hypertrophy. One of the most difficult problems confronting the physician dealing with urinary tract infections is that of microbial resistance to antimicrobial agents. Many urinary tract bacteria are capable of expressing resistance in one form or another3. Some bacteria causing several kinds of human urinary tract infections are becoming resistant to multiple antibiotics, and are continuing to increase. Resistant infections confront and thwart the treatment of UTIs in the community as well as in the hospital. The resistant bacteria may be present from the commencement of the infection or may develop during treatment, and, therefore, a study of this kind is helpful in managing UTIs much better. This study focused on the problem of antibiotic resistance to the first-line drugs that were used to treat patients presenting with urinary tract infections at Rubaga hospital in Kampala, Uganda. The main objective was to isolate the major bacterial pathogens associated with UTI among patients at Rubaga hospital and then establish the antimicrobial susceptibility patterns of these isolates to first-line drug treatment in order to identify the first line drugs that were still relatively effective against resistant urinary tract bacteria. Materials and methods Study site and ethical issues: The study was conducted among patients presenting with UTI at Rubaga hospital, and on patients who were requested to provide a urine sample by the physician(s) and found to have significant bacteriuria. Permission to carry out this study was sought and obtained from the management of Rubagga Hospital. Study population: Patients were recruited for the study using a systematic sampling procedure irrespective of history of UTI. Mainly outpatients were examined; in-patients having in-dwelling catheters were excluded from the study; because their inclusion would complicate the analysis. Sample size was estimated according to a standard formula4. Specimen collection and handling: Standardized procedures for collecting urine were followed5. The specimens were refrigerated at 40C soon after collection and transported to the microbiology laboratory in leak-proof containers for microscopy and subsequent culture. Microscopy, culture and identification: A wet preparation of fresh-centrifuged urine was made from each urine specimen following established procedures6. Urine that was found to contain more than 5 pus cells/HPF was cultured. The white blood cells (WBCs) were reported as the number per high power field (HPF), i.e. less than 5,6-20, or 21-40 WBC/HPF, or as full field. Culturing of the specimens was done according to standard procedures7. The biochemical identification of the urinary tract bacteria was done according to standard guidelines6. Antibiotic susceptibility testing: The Kirby-Bauer8 test system was used. This was a highly standardized technique for antimicrobial susceptibility testing using the single-disk method; the amount of antimicrobial agent contained in the disk was specified as well as the test medium, size of the inoculums, conditions of incubation, and other details. A plate of Mueller Hinton agar was used for each specimen to test for the susceptibility or resistance of the isolates to the antibiotics being used. All organisms isolated from urine specimens as single organisms were tested using standard procedures9. Data analysis: The summary statistics obtained in the study were reported and compiled. The Chi-square test (p-value) was used to test the hypothesis. Significance was set at á = 0.05. Results The bacteria isolated from urine cultures A total of 97 urine samples with confirmed urinary tract infection (UTI) were obtained, as described in the methodology, without regard to the age or sex of the patients. Of these, 22 patients (22.7%) had UTIs that were associated with multiple infections. However, no more than two isolates were obtained from any of the 22 urine specimens, and 21 of these specimens were from in-patients admitted to the hospital; only one outpatient had a multiple infection. The total number of isolates obtained from the 97 urine specimens was 119. Six different genera of causal organisms of UTI were identified from the urine specimens obtained from patients. The isolates were classified as Staphylococcus species, Streptococcus species, unclassified coliforms, Escherichia coli, Klebsiella species, and Proteus species (Table 1). Of the 119 isolates obtained in the study, 38 of them were identified as Staphylococcus species (31.9%), 12 were Proteus species (10.1%), 11 were Streptococcus species (9.2%), and 13 were Escherichia coli isolates (10.9%). In addition, 20 unclassified coliform isolates (16.8%), and 25 Klebsiella species isolates, representing 21.0% of the total number of isolates, were also obtained from the 97 urine specimens sampled. The unclassified coliforms were probably Enterobacter species but confirmatory tests were unavailable at the laboratory where the bench work was carried out. These isolates were lactose fermenting on MacConkey agar, yielding pink-coloured colonies. However, these isolates were negative to the indole test (and were therefore not E. coli species). Their colonies were small and flat (not the large, rose-pink and dome-shaped colonies for Klebsiella species). The gram reaction for these isolates showed uniform gram-negative rods (not the polymorphic gram-negative rods of E. coli). Antimicrobial susceptibility of isolates Cotrimoxazole: All the six genera of isolates exhibited significant resistance to this drug (Table 2 & 7). Streptococcus species were moderately resistant to the drug (45.4% were susceptible). Staphylococcus, Proteus, and Klebsiella species exhibited high resistance to the drug (only ~21%, 16.7% and 24% were susceptible to the drug respectively). Resistance to cotrimoxazole was highest in E.coli (susceptibility 7.7%) and in the unclassified coliforms (susceptibility 5%). Ciprofloxacin: Streptococcus and E.coli species were all highly susceptible to this drug with percentage susceptibilities of 72.7% and 76.9% respectively. These percentages included isolates of Streptococcus and those of E.coli that showed intermediate susceptibility to the drug (Table 7). Staphylococcus, Proteus, and the unclassified coliforms (Enterobacter species) isolates were all moderately sensitive to ciprofloxacin with the susceptible organisms making up 63.2%, 58.3%, and 50% of the respective isolates. Two unclassified coliforms had intermediate susceptibility to the drug (Table 7). Klebsiella species were the only organisms that were highly resistant to ciprofloxacin; only 24% of the Klebsiella isolates were susceptible to the drug (Table 2 & 7). Amoxycillin: There was a moderately high degree of sensitivity (60.5%) to this drug in patients with UTIs associated with Staphylococcus infection (Table 7. Streptococcus was highly susceptible to amoxycillin (72.7%) (Table 7). There was, however, a very high resistance to the drug in the Escherichia coli and Klebsiella species (susceptibility 7.7% and 4% respectively).Resistance to amoxycillin was also high in Proteus, which had 33.3% of its isolates responding well to treatment. The unclassified coliforms were almost completely resistant to amoxycillin with 15% of these isolates showing only intermediate susceptibility to the drug (Table 7). The rest of the unclassified coliform isolates (Enterobacter) were resistant to amoxycillin (Table 3 & 7). Nalidixic acid: Of the six genera of isolates, only Proteus showed appreciable susceptibility to nalidixic acid (66.7%) (Table 7). Streptococcus (9.3%) and the unclassified coliforms (5%) were very resistant to the drug. Drug percentage susceptibility in Staphylococcus, Klebsiella and Escherichia species was 23.7%, 28%, and 30.8% respectively (Table 6 & 7), which also indicated a high resistance of these organisms to treatment using nalidixic acid. Nitrofurantoin: The susceptibility of Proteus, and that of the unclassified coliforms, to this drug was just average at 50% (Table 5 & 7). Nitrofurantoin was most effective against E.coli and Klebsiella species giving rise to percentage susceptibilities of 69.2% and 72% respectively. However, 33.3% of all the Proteus isolates revealed intermediate susceptibility to nitrofurantoin, and these were included when calculating the percentage susceptibility of these isolates to treatment with the drug, giving a value of 50 % susceptibility (Table 7). Furthermore, 12% of the Klebsiella species and 10% of the unclassified coliforms also showed intermediate susceptibility to nitrofurantoin, and were included when calculating the percentage susceptibilities of the organisms; giving susceptibility values of 72% and 50%, respectively (Table 7). Streptococcus species were moderately sensitive to the drug (54.6%). The susceptibility of Staphylococcus to nitrofurantoin treatment was 42.1%. Erythromycin: Streptococcus species responded well to erythromycin treatment (72.7%). 9% of these isolates (1/11) showed intermediate susceptibility to erythromycin (Table 7). Staphylococcus species showed modest sensitivity to erythromycin treatment with a percentage susceptibility of 57.9%, including 4 isolates that had intermediate zones of drug sensitivity (Table 7). Klebsiella species, together with the unclassified coliforms and Escherichia coli isolates, were all highly resistant to the drug. Their percentage susceptibilities were 8%, 15%, and 23.1%, respectively. Proteus was completely resistant to erythromycin treatment. In general, the most resistant organisms among all those isolated were the Klebsiella species that registered high resistance to all but one of the first line drugs used to treat urinary tract infections at Rubaga hospital (Table 7). Klebsiella only responded well to nitrofurantoin, although 3 (12%) of its isolates only showed intermediate susceptibility to the drug (Table 7). Klebsiella species were highly resistant to ciprofloxacin, cotrimoxazole, and to nalidixic acid; and nearly completely resistant to amoxycillin and erythromycin. The unidentified coliforms were the next resistant causal organisms of UTI, followed by Escherichia coli, Proteus and Staphylococcus species, in that order (Table 7). Streptococcus species were, generally, satisfactorily sensitive to most of the drugs; significant resistance of these isolates was mainly against nalidixic acid and cotrimoxazole only (Table 7). Discussion In this study Staphylococcus species were by far the most isolated infecting organisms. The frequency of infection caused by Proteus, Klebsiella, and Enterobacter species; and by enterococci and staphylococci is higher in recurrent UTIs, especially in the presence of structural abnormalities of the urinary tract10. 77.3 percent of the urinary tract infections (UTIs) were caused by a single bacteria species. With the exception of Proteus species, which were reasonably susceptible to nalidixic acid, Staphylococcus, Streptococcus, Enterobacter (the unclassified coliforms), Escherichia coli, and the Klebsiella species were all resistant to this drug. This result is not in agreement with those reported elsewhere9 where it was reported that the drug was useful for the treatment of UTIs caused by E.coli and all species of Enterobacter and Klebsiella, but agrees with the fact that Proteus responds well to nalidixic acid treatment. The above resistant organisms probably developed resistance due to the widespread use of this drug in hospitals when treating UTIs. It is known that the follow up cure rate of nalidixic acid is quite disappointing3. The results of this study at Rubaga hospital also show that there is continuing low frequency of nalidixic acid-susceptible gram-negative bacteria, as all the gram-negative bacteria in this study were significantly resistant to the drug. This development of resistance could be due to the indiscriminate use of the drug, since it is even available over the counter in many pharmacies. Nitrofurantoin was found to be suitable for the treatment of UTIs, particularly those caused by Klebsiella, Escherichia coli, Streptococcus, Proteus and the Enterobacter species (unclassified coliforms in this case). Due to its wide spectrum of activity against such important organisms that cause urinary infections, nitrofurantoin can be effectively used for long-term suppressive therapy. Staphylococci may have only recently developed significant resistance to nitrofurantoin. So it could still be used to treat UTIs where staphylococci have been identified as the causal organisms; although only 42.1 percent of the Staphylococcus isolates were susceptible to the drug. This drug, therefore, may be used as a last resort in the treatment of UTIs associated with Staphylococcus species. The results obtained in this study are probably due to the fact that there is no evidence that infectious transferable resistance (mediated by R-plasmids in bacteria) occurs with nitrofurantoin treatment 11. The gram-positive cocci were all still highly susceptible to amoxycillin. The enterobacter were, however, very highly resistant to the drug; and the same applies to the other Enterobacteriaceae (Klebsiella and E.coli). Proteus was also highly resistant to amoxycillin. Amoxycillin significantly alters the normal periurethral flora, most patients acquiring a flora of either resistant aerobic gram-negative rods (as seen in this study) or Candida albicans12. Such alteration of the periurethral flora may precede a recurrence of infection with resistant organisms. There is, therefore, a big possibility that many of the patients who were on amoxycillin treatment before may have had a recurrence of infection with resistant organisms, resulting in the high resistant pattern to this drug that was observed in this study. All the six genera of isolates were resistant to cotrimoxazole, a sulphonamide that belongs to the group sulfamethoxazole (a member of the major sub-group of short-acting sulphonamides). This is in line with the observation made3, that bacterial resistance to sulfonamides is now common; and that sulphonamide-resistant strains of E.coli and all other Enterobacteriaceae are now common, particularly in hospitals. However, the streptococci which were noted to have become susceptible to the drug appear to have mutated back to the resistant strains3. The results of this study seem to suggest that the streptococci have only recently become resistant to the drug since their susceptibility was 45.4 percent. This development of resistance is probably due to the fact that these drugs are extensively used to treat UTIs in domiciliary practice, because of their low cost13. Elsewhere, it has also been noted that sulphonamides are not usually effective against chronic and recurrent infections or in hospital-acquired infections3. Erythromycin was highly effective against streptococci (72.7%). This result is in line with the observation elsewhere3 that erythromycin, when used to treat UTIs, is largely highly effective against the enterococci; and that strains resistant to erythromycin are rare among the usually sensitive streptococci. 57.9 percent of the Staphylococcus isolates were erythromycin-sensitive. There is, therefore, a danger that in a relatively short time, more Staphylococcus strains could become resistant to the drug. However, it must also be noted that some authors 11 consider that there is only a slight risk that sensitive strains of Staphylococcus species will mutate to become resistant to erythromycin and, therefore, this drug can still be freely used in domiciliary patients without causing resistance. Based on this study, it is clear that the indiscriminate use of this drug in patients with UTIs could easily result in the susceptible microorganisms being selected against, leaving only the strains that are resistant to the drug. Erythromycin must, therefore, be selectively used when treating urinary infections to reduce the chances for the mutation of susceptible microorganisms to the resistant strains. Ciprofloxacin was the most active drug against the different causal organisms for UTI. Streptococcus, Escherichia coli, Staphylococcus, and the Proteus species were all encouragingly susceptible to the drug. The unclassified coliforms (Enterobacter) were just moderately susceptible to ciprofloxacin treatment. However, Klebsiella species were highly resistant to the drug. The cause for this is probably because this genus of organisms was often associated with hospital-acquired multiple infections that put a lot of selective pressure on the susceptible organisms, leading to their elimination from the population. This means that the Klebsiella isolates obtained in this study were largely those that had developed resistance against ciprofloxacin. Acknowledgements The guidance and assistance of Dr. Bukenya Joseph of Rubaga hospital is hereby acknowledged. The technical assistance of Mr. Musisi Lubowa is hereby appreciated. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07041t7.jpg] [hs07041t2.jpg] [hs07041t1.jpg] [hs07041t3.jpg] [hs07041t6.jpg] [hs07041t5.jpg] [hs07041t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}