 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 7, No. 4, December, 2007, pp. 232-238 Oral health status of school children in Mbarara, Uganda Batwala V1, Mulogo EM1, Arubaku W2 1 Department of Community Health, Code Number: hs07044 Abstract Background: Despite the need for oral health morbidity surveys to aid in reviewing of the oral health services, dental data of
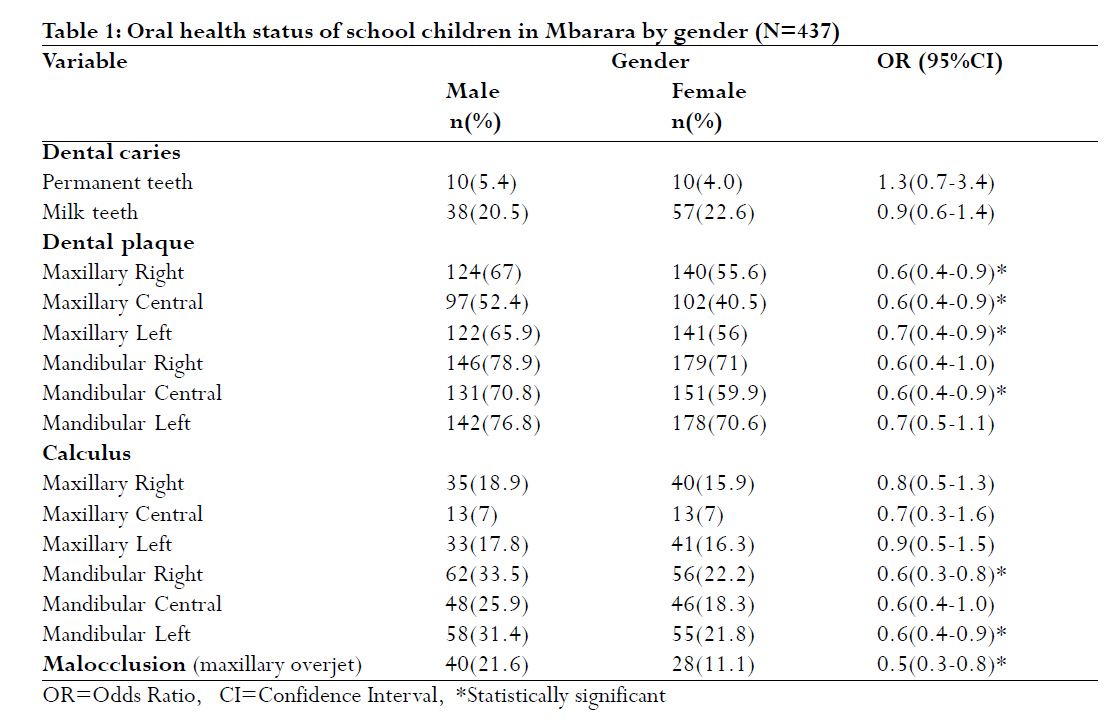
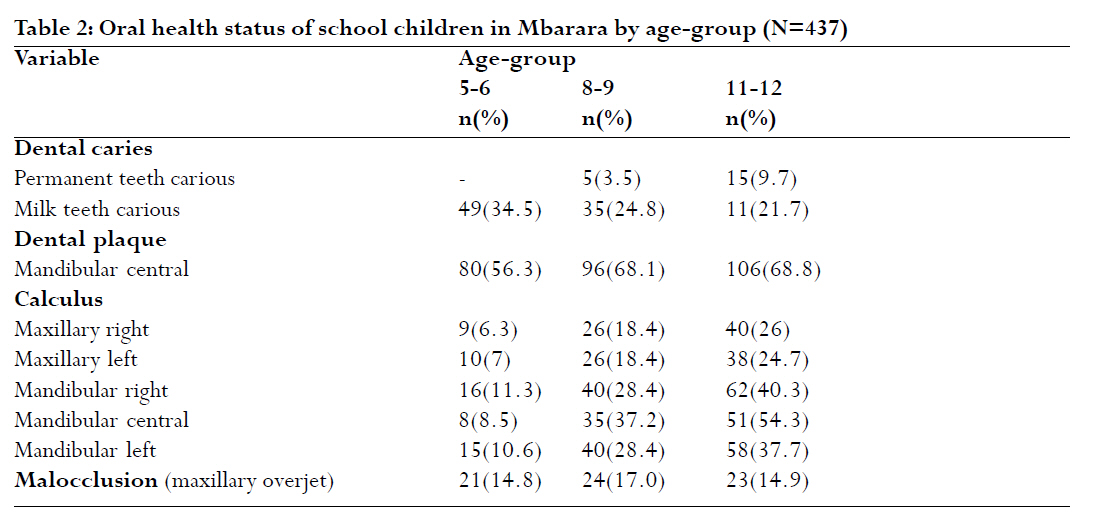
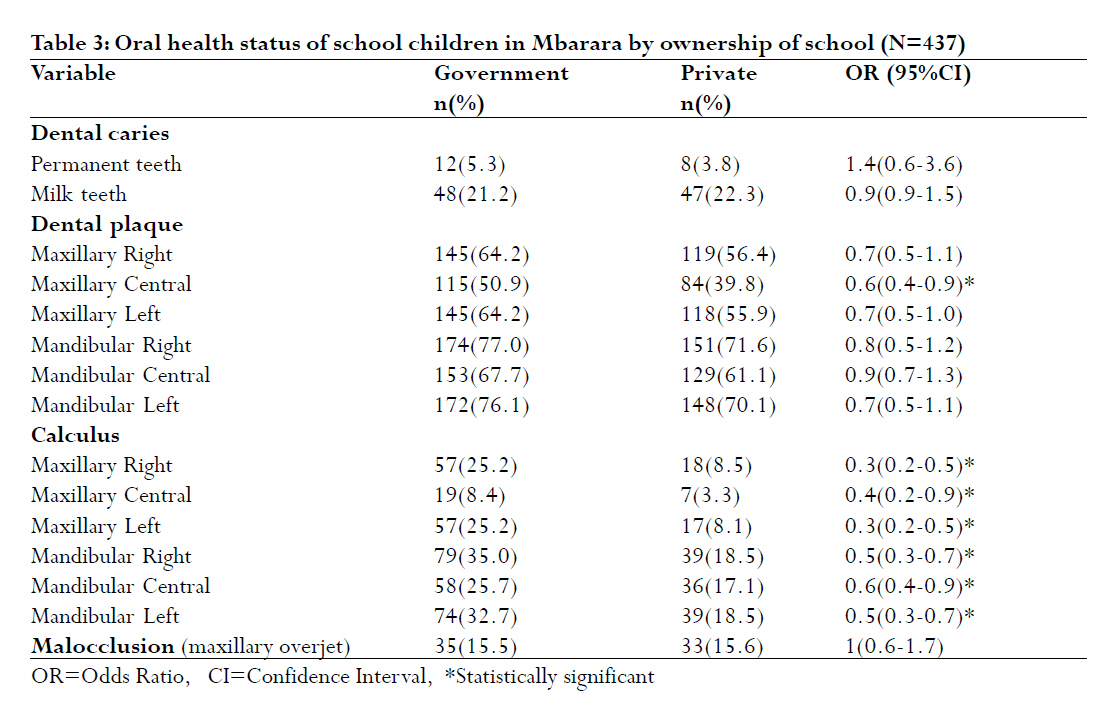
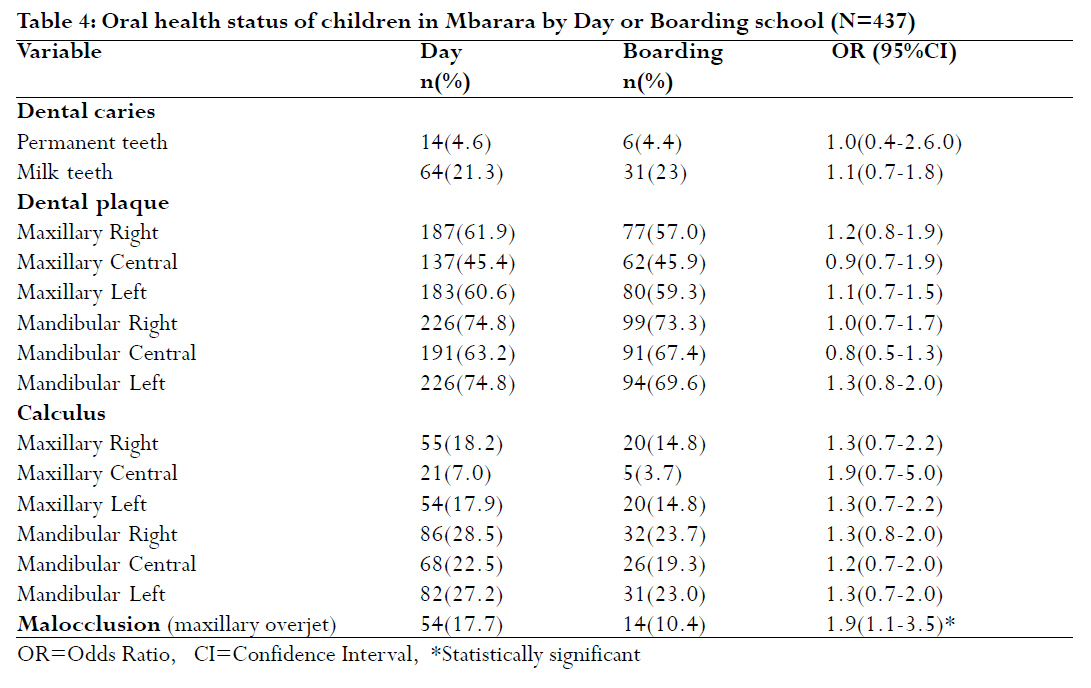
Ugandan children is scanty. Key words: Calculus, Caries, DMFT, dt, Fluorosis, Gingivitis, Malocclusion, Plaque, Uganda. Introduction Dental caries and gum diseases have been reported to be major oral health problems in Africa and elsewhere.1,2 It is estimated that as many as 19 percent of children aged 2 to 5 years and 52 percent of children aged 5 to 9 years have experienced dental caries.3,4 Dental caries varies from a Decayed, Missing and Filled Teeth (DMFT) 0.23 at age 5 years to 7 in 12-year-olds1,5-8 The prevalence and severity of gum diseases have been reported as high in the Africans (urban and rural combined). In some settings, 60-90% of children aged 12 years have poor oral hygiene allowing dental caries and other oral diseases to develop unchallenged.9,10 In Uganda, dental fluorosis has been estimated to vary from 3% to 23% among primary school children,7,8 and various forms of malocclusion to be 61%.7 A study in Kenya reported that maxillary over jet was 13% and spacing (60%) in the anterior teeth of 3-6 year-old children.11 Few studies7,8,12,13 have assessed the oral health status of the Ugandan population, yet out of pocket spending on dental treatment is substantial. In Mbarara, the cost of dental treatment in private clinics is estimated at US$ 3.9 for a tooth extraction, US$ 16.7 for scaling and polishing, US$5-13 for amalgam or composite filling and US$ 66.7 for correcting the dentition of a child with an orthodontic appliance. Absenteeism from work associated with dental problems and the undocumented effects on the level of performance of children in class are now recognized as problems of public health and socioeconomic concern. This article assessed the magnitude and distribution of selected oral health conditions affecting school children living and attending primary schools in Mbarara, Uganda. Materials and methods Study setting The study was implemented in Mbarara municipality located in Mbarara district in southwest Uganda with a total population of 69,218 people. The municipality has 39 primary schools (19 Government aided and 20 Private) with total enrolment of 19,699 (9,411 boys and 10,288 girls). There are four health units (including one of the government owned Mbarara Regional Referral Hospital-MRRH) providing oral health services. Four dentists and two dental assistants provide services in the municipality. MRRH dental clinic is manned by two dentists and the two dental assistants. MRRH provides free services; however, due to constant lack of restorative/conservative dental materials, these services are limited to tooth extractions. For restorative and periodontal treatment, patients are either referred or self-referred to the three private clinics located in town about 200 metres away from the hospital. Study design This was a clinical survey that employed quantitative techniques. A stratified two-stage cluster sample of 437 children was selected. Nine schools were randomly selected. Three classes with the largest numbers of children in the age-groups 5-6, 8-9, 11-12 years were selected per school. Age 6 was selected to reveal the history of milk dentition, age 9 to reflect the status of mixed dentition and the 12 to indicate the progressive status of permanent dentition. Two trained and calibrated dental assistants examined the children. Children were examined for dental caries, dental plaque, calculus, gingivitis, maxillary overjet and fluorosis under field conditions. Children were examined in the school compound in supine position with the head resting on a pillow placed on the laps of the examiner with adequate sunlight. Examination for dental caries was conducted with a plane mouth mirror and dental explorer. The examiners adopted a systematic approach-proceeding from one tooth space to the adjacent tooth or tooth space. A tooth was considered present in the mouth when any part of it was visible or touched with the tip of the explorer without unduly displacing soft tissue. If the permanent and primary tooth occupied the same tooth space, the status of the permanent tooth only was recorded. Dental caries was scored by surface according to WHO criteria. A numerical coding system was used for recording the status of permanent teeth and an alphabetical coding system for primary teeth. For plaque, gingivitis, calculus and fluorosis, the mouth was divided into six sextants (3 in each jaw -right, central and left). The mouth mirror and WHO 621 light weight probe with a 0.5mm ball tip were used. Plaque, gingivitis and calculus were scored as "present" or "absent." Fluorosis was graded as: normal, questionable, very mild, mild, moderate and severe on the basis of two most fluorosed incisors. Maxillary overjet was scored as: "no anomaly" or "serious anomaly (≥9mm)." Children who were in need of dental care were asked to be brought to hospital dental clinic for treatment. Mbarara University of Science and Technology Faculty Research and Ethics Committee approved the study. Permission was sought from Mbarara District Education Office and Mbarara Municipality and school authorities to conduct the study. Eligible children were given consent forms to be signed by their parents/legal guardians. Only children who returned signed forms were enrolled. Results: Background characteristics of study participants. Males were 185(42.3%) and females 252(57.7%). Those in government schools were 226(51.7%) and 211(48.3%) in private. One hundred thirty five (30.9%) were in boarding- while 302(69.1%) were in day- schools. Age-group 5-6 years constituted 142(32.5%), 8-9 years 141(32.3%) and 11-12 years 154(35.2%). Dental caries and fluorosis A total of 3633 permanent teeth had not erupted (1873 in maxilla and 1760 in mandible). Some 10277 teeth (7089 permanent and 3188 milk teeth) were visible in the mouth and were examined. Twenty (4.6%) children had dental caries in their permanent teeth and 95(27.1%) had dental caries in milk teeth. The Decayed Missing and Filled permanent teeth (DMFT) index was 1.5(±0.8SD) with a "D" component of 1.25. Only one child had a permanent tooth filled. Males had less caries in permanent teeth (DMFT: 1.3±0.7SD) compared to females (DMFT: 1.6±0.8SD), although the difference was not statistically significant. The decayed milk teeth (dt) index was 2.7(±1.8SD). Males had more caries in milk teeth (dt: 3.1±2.1SD) compared to females (dt: 2.4±1.6SD) (Table 1). Dental caries in permanent teeth increased with age (p<0.0001) while that in milk teeth decreased with increase in age (p<0.0001) (Table 2). Children in private had more caries compared to those in government schools in both milk teeth (dt: 2.9±1.9SD vs. 2.4±1.7SD) and permanent teeth (DMFT: 1.6±0.9SD vs. 1.3±0.7SD respectively) (Table 3). Day- scholars had more caries in permanent teeth, but less so in milk teeth although the difference was not statistically significant (Table 4). Eight (1.8%) had fluorosis ranging from "very mild" to "moderate." Missing teeth Four children lost six permanent incisors due to trauma. Nine (2%) had missing permanent teeth due to the cultural practice of "nylon teeth mutilation." Of the nine, seven were female. Six were attending government schools. Twenty four teeth were removed due to this practice. Six children had bilateral maxillary canines removed. One child had bilateral mandibular canines extracted. Two (females) had all four canines extracted. Soft deposits (dental plaque) Majority 325(75%) harboured dental plaque that increased with age (p<0.0001). Males significantly had plaque compared to females. Attending private schools was associated with less dental plaque (OR: 0.6, 95%CI: 0.4-0.9) (Table 3). Children in day- schools had more plaque, but there was no statistically significant difference from those in boarding- schools (Table 4). None of the children had severe gingivitis. Dental stones (dental calculus) One hundred thirteen (25.9%) had dental calculus. Being male was a significant predictor for calculus, especially in the lower jaw. Calculus increased with age (p<0.0001). Children in government schools significantly possessed calculus compared to those in private schools in all sextants (Table 3). Day-scholars were more likely to have calculus although there was no statistically significant difference from those in boarding. Malocclusion Female were associated with less maxillary overjet (OR: 0.5, 95% CI: 0.3-0.8). Day-scholars were about 2 times more likely to have maxillary overjet than those staying in boarding (OR: 1.9, 95%CI: 1.1-3.5). Children in government were equally likely to have maxillary overjet as in private schools. Two children had serious crowding while one had open bite. Discussion Despite the need to conduct yearly oral health morbidity surveys to aid in planning and reviewing of oral health services, dental data of Ugandan population is scanty due to limited research in the dental discipline. This study reports that the oral hygiene of primary school children was poor with a high prevalence of dental plaque reflecting a lack of established oral hygiene practices. Plaque prevalence among the 5-6 year olds reported here is about 2 times that reported among the 5-year olds in Kampala.12 This finding indicates a need for oral health education to be strengthened in the ongoing school health programme. Children in private schools and those in boarding schools were less likely to have plaque. This finding may not only be a reflection of socioeconomic background, where parents/guardians are able to buy toothbrushes, but also brushing of teeth in the morning is a collective practice in boarding schools. The proportion of children with calculus observed among those in government schools was higher than that in private schools. In addition, more children in day-schools had calculus as compared to those in boarding. The two findings suggest that the boarding and private school environments have a synergistic effect in improving the oral hygiene of primary school children. The increase in calculus with age is a reflection of the duration of soft deposits in the children's mouth that have eventually calcified. We have established that fluorosis is prevalent in Mbarara. The level of fluorosis reported here is however less than that reported in other studies.7 Further still, it is lower than that recommended for optimal fluoride ingestion for combating dental caries in Uganda.14 The current study has also established that children who exhibited more maxillary overjet were predominantly male. Further studies are needed to assess the causes of maxillary overjet especially among males. Dental caries experience in both milk and permanent teeth presented here is low compared to that reported in other parts of Uganda,7,12,13 and in other settings.2,10,15-18 The DMFT at age 11-12 years was lower than WHO goals for the year 2000.1 Although the caries rate was low, it is vital to direct efforts at preventing further deterioration in the dental status of these children. The decrease in milk caries with age is an indication of the normally increased exfoliation of milk teeth with age. The low caries level observed in permanent teeth among children in boarding may be attributed to policies (in some schools) that require children to undergo general medical and dental check-up before beginning of new term. The higher levels of milk caries among children in private and in boarding is an indicator of the difference in socioeconomic class. Children in private and those in boarding- schools where parents pay money for education are considered to be well-off economically compared to those attending free government schools. They are therefore likely to be exposed to risk factors such as sugary foodstuff sold at school. With change in dentition, females tended to develop more caries in permanent teeth. This may be due to females' preference of sugary foodstuff compared to males. The high caries to filled teeth ratios reveal that dental services are greatly needed. The fact that only one child in the study population had a permanent tooth filled while the rest did not, is an indicator that cost for dental services was prohibitive especially in private clinics that perform restorative procedures. We have reported that "nylon teeth mutilation" locally known as "Ebinyo" is still practiced in Mbarara. Missing teeth due to this cultural practice was bilateral in a jaw and the canines were mostly affected-in severe cases, all the four canines were missing. Primitive extraction of tooth buds (one or both canines) in a jaw leads to forward shift of posterior teeth. This movement disturbs the ideal teeth alignment as for example the maxillary premolars would be occluding with the mandibular canines. Conclusions and recommendations The oral hygiene of primary school children in Mbarara was poor with high prevalence of dental plaque, low levels of dental calculus, fluorosis and dental caries. A high prevalence of dental plaque shows a lack of established oral hygiene practices. With change in dentition, females tended to develop more caries in their permanent teeth. A comprehensive community-focused oral health care intervention that includes oral health education in homes and strengthening of school health programme is needed to improve the oral health status of children in Mbarara. Acknowledgement This study was funded by Faculty of Medicine, Mbarara University of Science and Technology. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07044t4.jpg] [hs07044t3.jpg] [hs07044t1.jpg] [hs07044t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}