 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 7, No. 4, December, 2007, pp. 239-243 Attitude of antenatal attendees to people living with HIV/AIDS in Uyo, south-south Nigeria Emem A. Bassey1, Festus Abasiubong2, Uwem Ekanem3, Aniekan M. Abasiatai1 1 Dept of Obstetrics and Gynaecology, Code Number: hs07045 Abstract Background: Stigmatization and discrimination of people living with HIV/AIDS has a negative impact on the global efforts to
control the HIV/AIDS pandemic. Due to fear of stigmatization and discrimination, many people are reluctant to undergo voluntary
counseling and testing, infected individuals are often unwilling to disclose their status and some of them still engage in high-risk behaviours
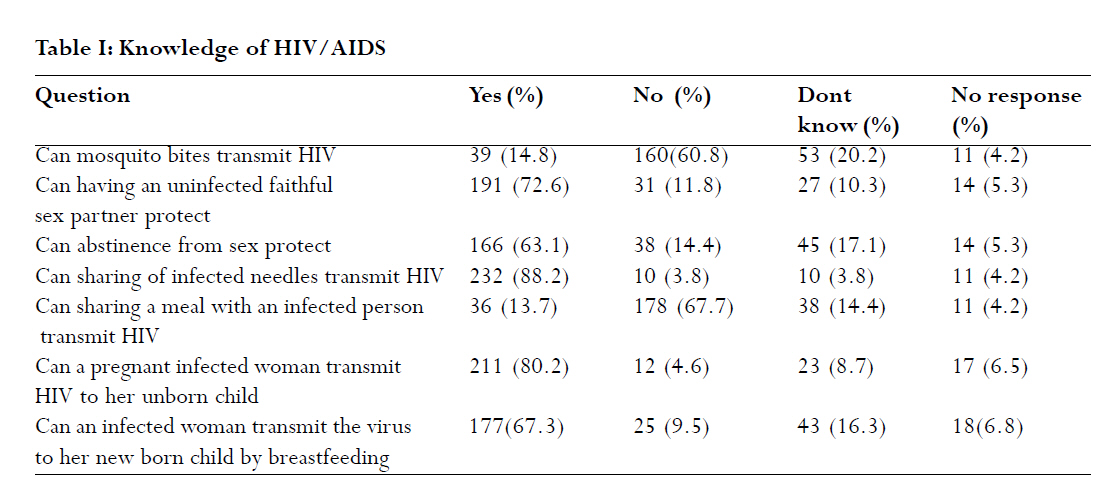
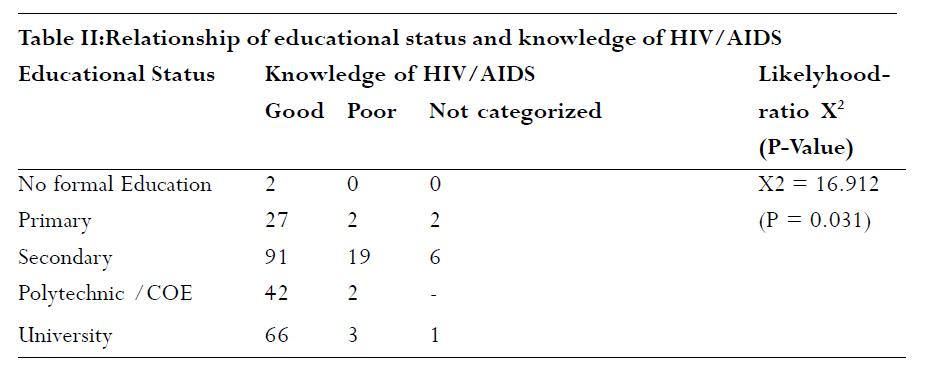
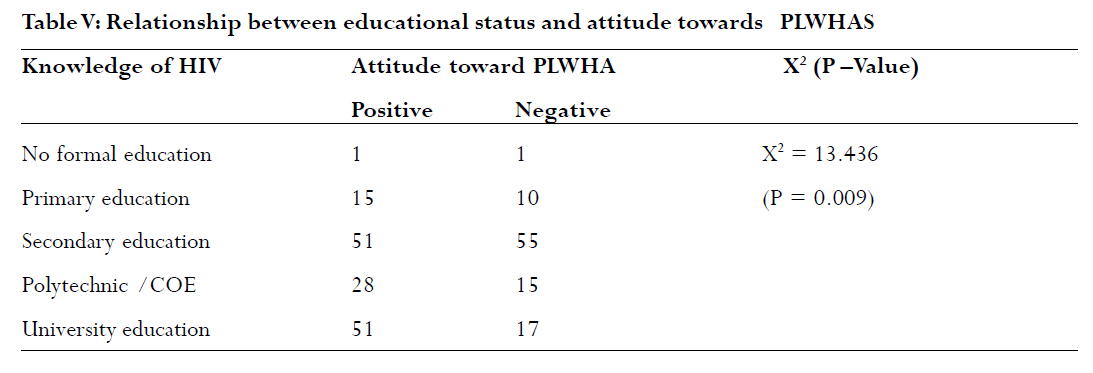
leading to increased transmission of the virus. Key Words: Attitude, Antenatal, Booking, HIV/AIDS, Uyo Introduction The global HIV/AIDS pandemic is a major public health problem. At present, there is no cure and most activities are aimed at reducing HIV transmission. Voluntary Counselling and Testing (VCT) is one of the strategies employed in the effort to control the global HIV/AIDS pandemic.1 Voluntary counselling and testing has been found to be effective in changing high risk behaviours and more than a 40% reduction in unprotected intercourse among individuals who received VCT, compared to those who received health information only has been reported.2 Unfortunately it is estimated that the majority of the more than 40million people living with HIV do not know their status and this proportion is highest in counties worst affected by the epidemic.3 The fear of stigma and discrimination is an important factor affecting the willingness of people to be tested for HIV.1, 4 Stigma and discrimination shown to people living with and affected by HIV/AIDS can worsen the spread and impact of the HIV/AIDS epidemic. In addition to affecting the willingness of people to be tested, people living with HIV/AIDS (PLWHA) are often reluctant to disclose their status 4, 5 and in extreme cases may knowingly spread the virus to others. Factors generally found to contribute to the HIV/AIDS related stigma include misconceptions about its mode of transmission and its association with behaviors such as homosexuality and intravenous drug addiction. Added to these are religious and moral beliefs that HIV/AIDS is the result of moral faults such as promiscuity or deviant sexual behaviour that deserve to be punished.6,7 HIV/AIDS prevention and control strategies in addition to the encouragement of behavioural modification and provision of antiretroviral drugs should also focus on the reduction of stigma and discrimination, protection of rights of PLWHA and their full integration into the society in ways that would allow them to live productive lives socially and economically.8 Prior to setting up Prevention of Mother-to-Child transmission Services (PMTCT) in a new site, it is recommended that a formative research be carried out to generate data on the knowledge, attitude, belief and practices of health care providers and community members as it relates to HIV/AIDS and PMTCT.9 The purpose of this study was to assess the attitude of women booking for antenatal care at the University of Uyo Teaching Hospital to PLWHA with the aim of developing a site-specific counselling intervention, which should specifically tackle misconceptions and negative attitudes to PLWHA. This could also be adapted for use in the surrounding host communities. It is also the intention of the authors to join the advocacy for protection of the rights and reduction in discrimination and stigmatization of PLWHA. Materials and methods This study was carried out at the antenatal clinic of the University of Uyo Teaching Hospital, a newly established tertiary health institution located in Uyo, the capital of Akwa Ibom State, Nigeria. It is at present the only such health facility in the state and is one of the antiretroviral therapy centers established by the federal government. The institution also offers prevention of mother to child transmission (PMTCT) interventions to all HIV positive women receiving antenatal care. Between September and December 2005, women who booked for antenatal care in the hospital were randomly selected (every even number) and recruited for the study. Participation was voluntary. Women who had received prior antenatal care at another facility or who admitted to being counseled for HIV/AIDS in the index pregnancy were excluded. An informed consent was obtained and pre-tested structured questionnaires based on sections 1 and 9 of a modified version of the instrument used for the National HIV/AIDS and Reproductive Health survey (NARHS) 2003, on knowledge, stigmatization and Discrimination of PLWHA were self administered to 265 subjects. This was usually done before the normal health talk, which includes general information on HIV/AIDS. This study was duly approved by the ethical review committee of the institution. The data was analyzed using the statistical package for social sciences (SPSS) version 11.0. Respondents' level of knowledge was computed by judging their answers to questions on mode of transmission of HIV/AIDS. A mark was awarded for every correct response and no mark awarded for incorrect responses. The total mark obtainable was 7. Respondents were graded as having poor knowledge if they scored below 4 and good knowledge if they scored 4 and above. The attitude of the respondents to PLWHA was also ranked on the basis of their opinions on stigmatization and discrimination of people living with the virus. Questions asked included whether they were willing to share a meal with an infected person or buy food from an infected seller, care for an infected male or female relation in the house, should an infected student be in school or teacher continue teaching and if they would keep the infection of a family member a secret. The maximum score was also 7 and respondents were graded as having a positive attitude if they scored 4 and above and a negative attitude if they scored below 4. Comparison of categorical data was done using the chi-square test (X2) and P value of < 0.05 was used as criterion for statistical significance. Where the cells had values of less than 5 the likelyhood-ratio chi-square was used.10 Results Two hundred and sixty-three questionnaires were well completed and only these were analyzed. This represented 41.2% of new antenatal clinic attendees during the study period. The ages of the respondents ranged from 12-44 years, mean 27 ± 5.1 years. Twenty-five (9.5%) respondents were 20 years of age and below, 2 were above 40 years, 54 (20.5%) were between 31- 40 years and 169 respondents (64.3%) were between 21- 30 years of age. Most of them 234 (89.0%) were married, 27 (10.2%) were single and 15 (5.7%) were in a polygamous relationship. Fifty-seven (21.7%) respondents were professionals, 38 (14.4%) were skilled workers, but majority 137 (52.1%) were either unemployed, unskilled or belonged to unclassified occupations. One hundred and thirteen respondents (42.9%) had tertiary education, 116 (44.1%) had secondary education, 31(11.8%) had primary education while 2 respondents had no formal education. Two hundred and forty-nine respondents (94.7%) were Christians, 7 (2.7%) were Muslims and the religion of 7 respondents (2.7%) was not stated. Most of them 199(75.7%) were Ibibio, 25(9.5%) were Ibos, 16(6.1%) were Efiks, 8(3.0%) were Yoruba, 1(0.4%) Hausa and 12 (4.6%) belonged to other tribes. Two hundred and Fifty two respondents (95.8%) were aware of HIV/AIDS. Two hundred and twenty eight (86.7%) were assessed as having a good knowledge of HIV/AIDS while 26 (9.9%) had poor knowledge of HIV/AIDS. Misconceptions about HIV/AIDS included answers by 39 (14.8%) and 36(13.7%) respondents that HIV could be transmitted by a mosquito bite and sharing a meal with an infected person respectively (Table I). There was a statistically significant association between knowledge of HIV/AIDS and the educational status of the respondents, 138 (95.6%) respondents with tertiary education had good knowledge of HIV/AIDS compared with 120 respondents (80%) with secondary education and less ( likelyhood- ratio X2 =16.912, P = 0.031). (Table II). Attitude to people living with HIV/AIDS Two hundred and forty-four respondents adequately filled the section of the questionnaire on stigmatization and discrimination of PLWHA and only these were analyzed. One hundred and forty-Six respondents (55.6%) were assessed as having a positive attitude to PLWHAS, while 98 (37.3%) were assessed as having a negative attitude. Positive attitudes to HIV/AIDS included answers by 101(38. 4%) and 125 (47.5%) that they were willing to care for infected male and female relations in their households respectively, 145 respondents (55.4%) who replied that an infected student should be allowed to continue attending school and 147 (55.9%) who replied that an infected teacher should be allowed to continue teaching. Negative attitudes including responses by 149(56.7%) that they would not share a meal with an infected person, 148 (56.3%) who would not buy food from an infected food seller and 141 (53.6%) respondents who would want the HIV positive status of a family member kept secret (TableIII). One hundred and forty-one respondents who were assessed as having a good knowledge of HIV/AIDS had a positive attitude to PLWHA compared with 80 respondents with good knowledge who had a negative attitude. (X2 = 14.735, DF=2, P=0.000) Table IV. There was also a statistically significant association between high educational status of the respondents and positive attitudes to PLWHA as 79 respondents with tertiary education had a positive attitude compared with only 32 of them who had a negative attitude. ( likelyhoodratio X2 = 13.436, P=0.009). Table V. Discussion This study revealed that awareness and knowledge of HIV/AIDS among antenatal clinic attendees in Uyo is high, though misconceptions on the mode of transmission of the virus were still present. This fact was corroborated by the National HIV/AIDS Reproductive Health survey 2005 and other Nigeria studies.11-13 These misconceptions have negative implications for interventions aimed at HIV/AIDS prevention, control and acceptance of PLWHA and should be specifically addressed.6,11 More than half of the respondents were assessed as having a positive attitude to PLWHAS and there were statistically significant associations between this, good knowledge of HIV/AIDS and high educational status of the respondents. This was a surprising observation, as earlier local studies reported predominantly negative attitudes among their respondents to PLWHAS even among well-educated people and health care providers who are supposed to have very good knowledge of HIV/AIDS.13,14 The finding in this study could partly be explained by the fact that being a more recent study, a lot of public education on HIV/AIDS had been carried out during the intervening period, creating more awareness on the mode of transmission of the disease. Furthermore, antiretroviral therapy has become more widely available and HIV/AIDS is now seen as a more manageable condition. Limitations of this study included the fact that it was hospital based and the sample size was small, thus the findings may not accurately reflect the general attitude of the local population to PLWHAS. Also the "don't know" and "no response" answers in the stigmatization and discrimination segment of the questionnaire used could have been indications of negative attitudes which could not be explicitly stated because of social desirability effect. If these were taken into account or if another survey questionnaire was used the findings could have been altered. Stigma and discrimination against PLWHAS is widespread in Nigeria and other African countries and involves all strata of the society including religious bodies that normally should provide succor.5,7,13-15 Some churches in Nigeria even require mandatory HIV testing for all couples wishing to get married and demand medical certificates of proof of negative status as a condition for marriage.14 The implications of the findings of this study is important since HIV positive pregnant women do not have a special antenatal clinic and maintaining strict confidentiality of a patients status is not always possible. If these women are discriminated against, they could default and resort to unorthodox birth attendants thus increasing the vertical transmission rates of the virus. As HIV/AIDS becomes the leading preventable cause of disease and death globally, the consequences of infection can no longer be ignored and comphrehensive strategies to cope with the ever increasing burden of suffering by people living with HIV/AIDS are urgently needed. Combating stigma and discrimination against people who are infected is as important as the provision of antiretroviral drugs in the process of preventing and controlling the global epidemic as this will encourage more voluntary testing, self-disclosure of positive status and more positive life styles among HIV positive individuals.1,2,5,16 Specific information, education and behavioural change interventions aimed at dispelling misconceptions against HIV/AIDS and reduction of stigmatization and discrimination should be implemented. This was shown to be effective among health care workers in Nigeria.17 Finally HIV positive individuals themselves should be better educated to enable them challenge the stigma and discrimination they encounter and should be involved in the design and implementation of projects to combat the virus. 11,18 References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07045t4.jpg] [hs07045t5.jpg] [hs07045t1.jpg] [hs07045t2.jpg] [hs07045t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}