 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 7, No. 4, December, 2007, pp. 246-252 Prevalence and determinants of ever smoked cigarettes among school-going adolescents in Lusaka, Zambia. aAdamson S. Muula, bSeter Siziya aDepartment of Community Health, University of Malawi College of Medicine, Blantyre, MALAWI, Code Number: hs07047 Abstract Background: Cigarette smoking is the single most important preventable cause of non-infectious diseases. There is limited data
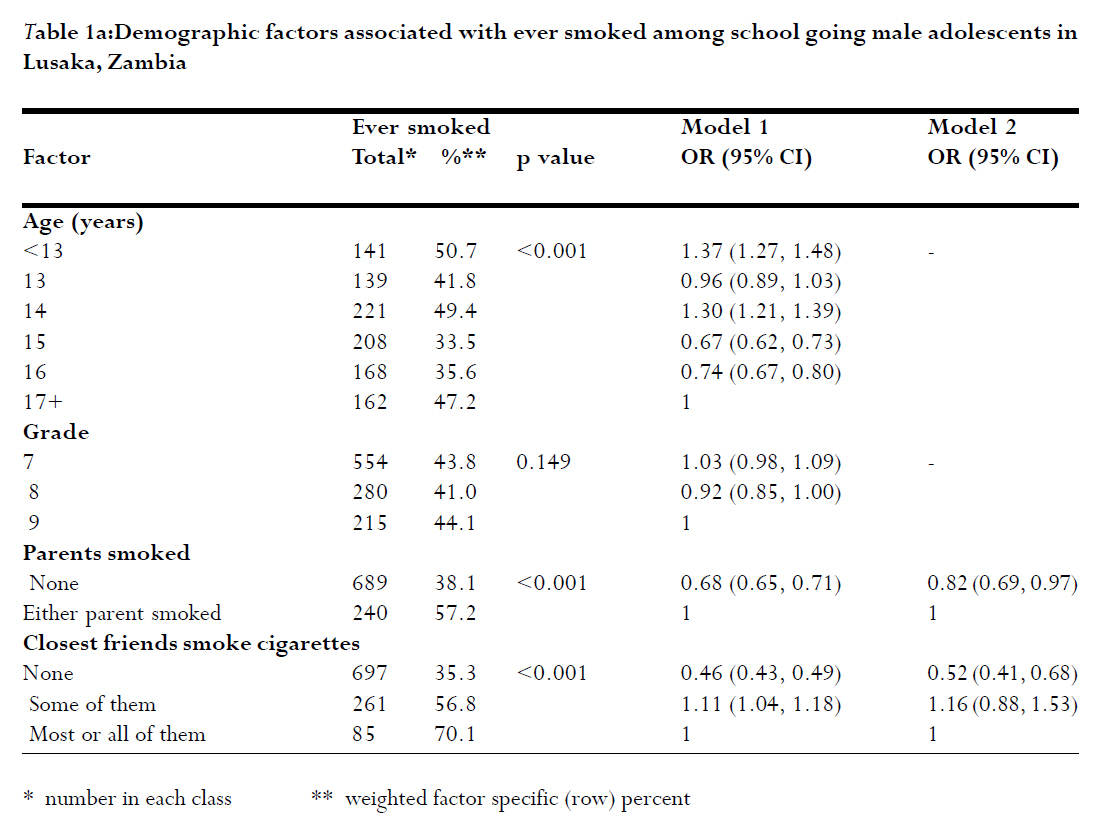
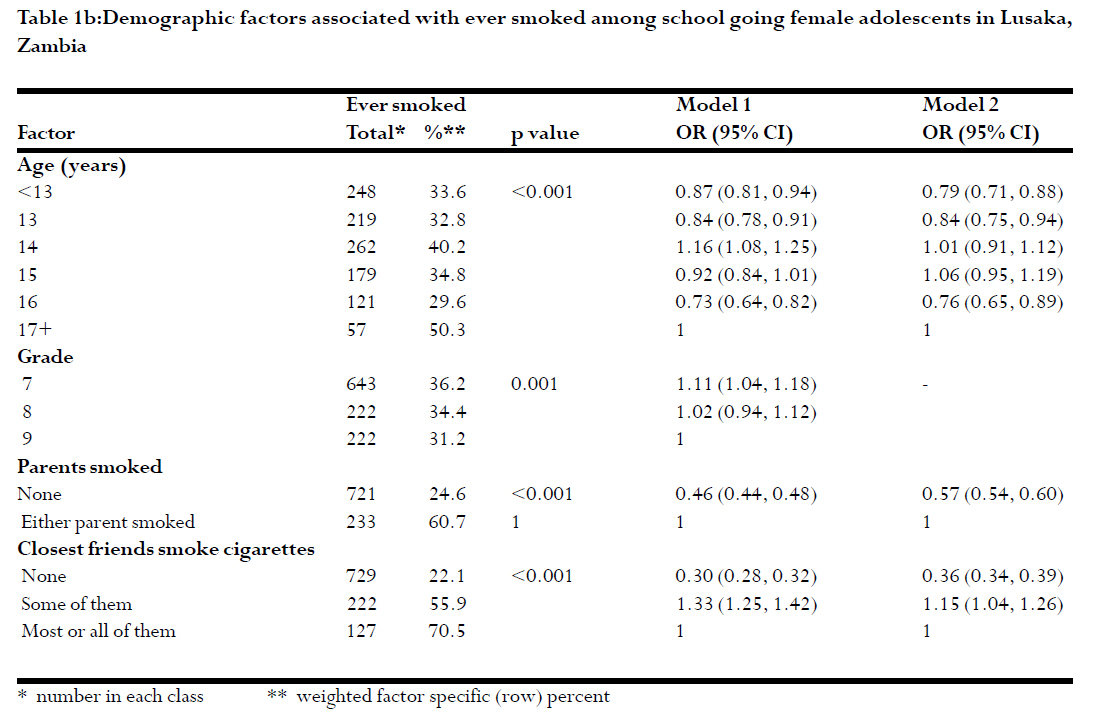
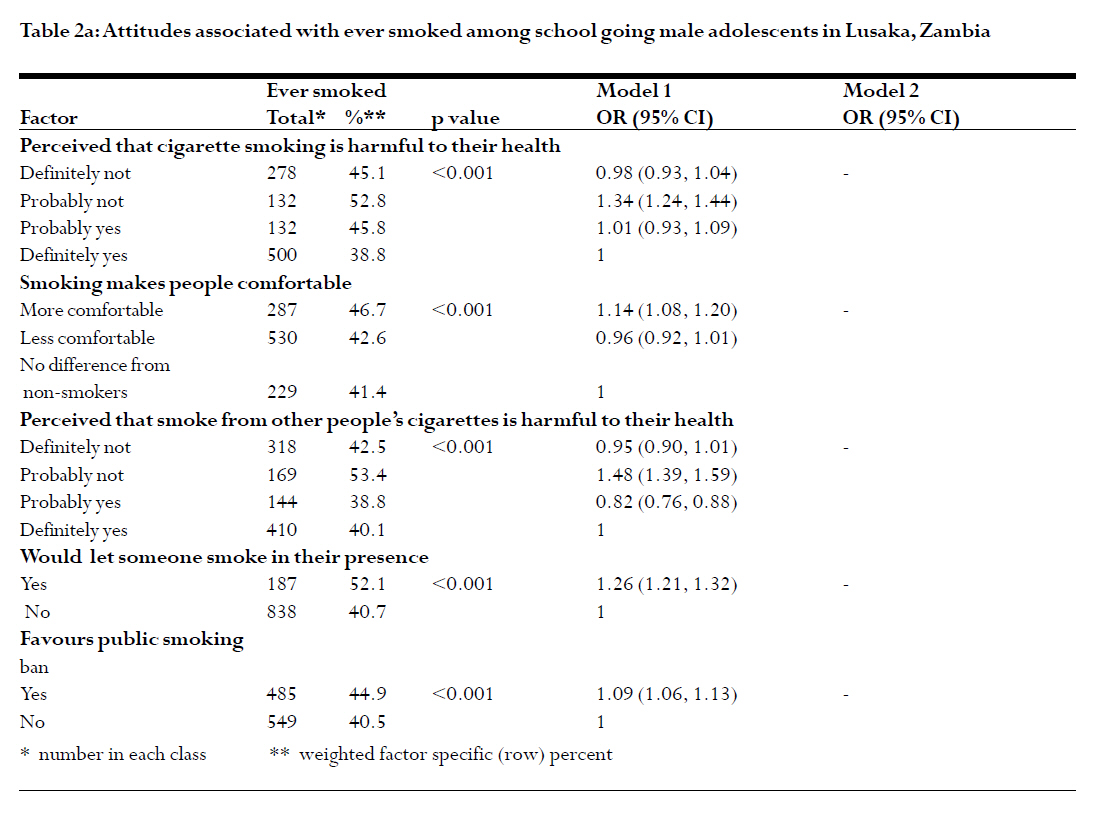
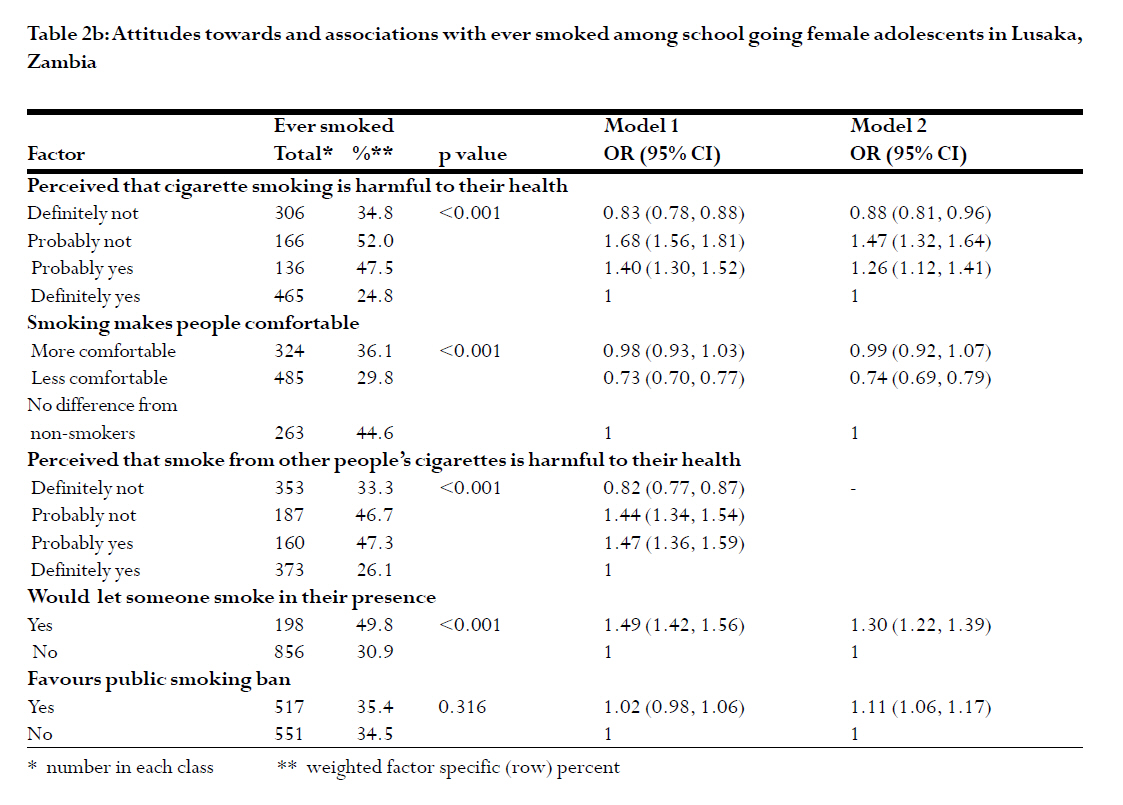
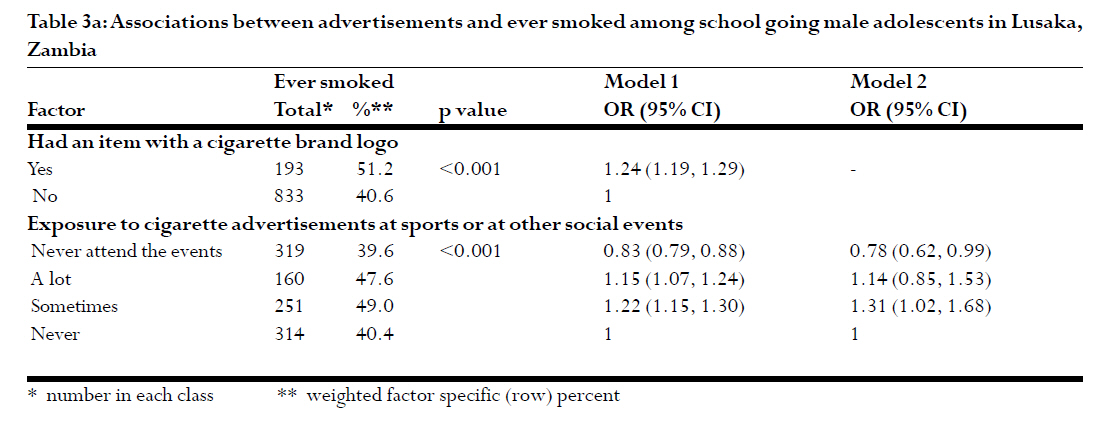
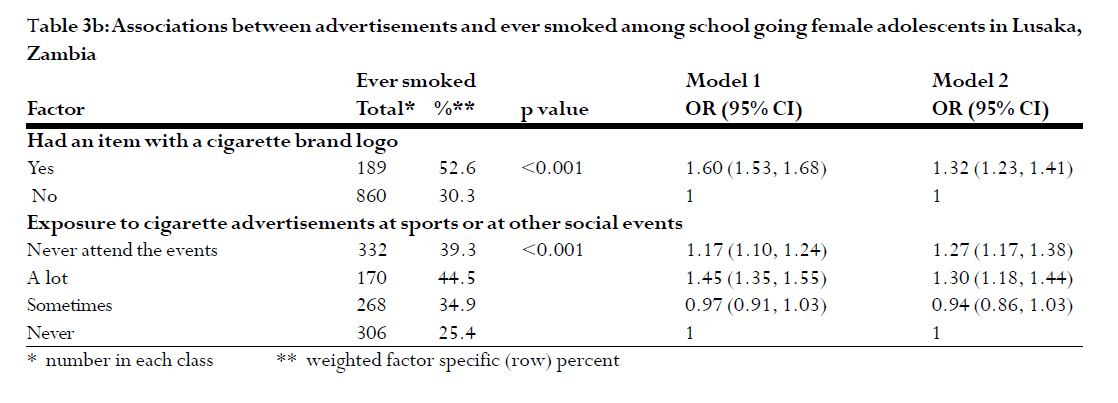
on adolescent smoking and its determinants in developing countries. Introduction Tobacco smoking is the single most important preventable cause of preventable morbidity and mortality from cancer and cardiovascular diseases. Although the greatest burden of disease in developing countries continues to be from infectious diseases, there is a growing recognition that non-communicable diseases are becoming significant public health concerns. 1Tobacco-attributable mortality is estimated to contribute about 10% of the total global mortality by 2020.2 In a systematic literature review on tobacco use among adults in sub-Saharan Africa, Townsend et al 3 reported that the prevalence of tobacco use was lower in this region compared to developed countries and was higher among males than females. The prevalence of cigarette smoking, again, among adults in Zambia has been studied by Pampel 4 using the Demographic and Health Survey data. The findings were that 10% of males were lighter-smokers, 6% were heavy-smokers, and 1% of females were light or heavy-smokers. In general, cigarette smokers were likely to be less educated, urban residents, non Christian and non Muslim and low waged employees. There is however paucity of data regarding adolescent tobacco use in the country. The `stage theory' has been suggested with regard to adolescent tobacco use in that initiation of tobacco smoking may later be associated with other unhealthy behaviours among young people.5 In New Zealand, Fergusson et al 6 have reported that use of cannabis by adolescents was associated with other illicit drug use. While current smokers are of public health interest, it is equally important that policy makers and public health program planners also consider the prevalence of having ever smoked, as individuals who have ever smoked are likely to continue or relapse.7 Tobacco firms may also target quitters in their marketing efforts.8 In order to design and implement anti-smoking programs targeting at adolescents in Zambia, there is need to assess the prevalence and determinants of history of smoking. The GYTS Collaborating Group 9 reported a prevalence of ever smoked cigarettes of 29.6% overall among 2277 respondents, and 36.0% among boys and 22.3% among girls. Determinants of ever smoked cigarettes were not analysed. We, therefore, carried out further analysis to document associations between selected demographic, attitudes and tobacco advertisements factors on one hand and history of ever smoked cigarettes on the other, among school-going adolescents in Lusaka, Zambia. We also aimed to document selected factor specific prevalence rates of ever smoked cigarettes. This information is useful as policy makers will have information as to who among adolescents is likely to smoke, and therefore target interventions to such groups of individuals. Methods Sample size and sampling The GYTS Collaborating Group conducted a cross-sectional study utilizing a multistage sample design in Lusaka, Zambia in 2002. Schools were selected proportional to their enrolment sizes, and classes within a selected school which had the majority of students within the 13 to 15 years age range were randomly chosen. The selected students were in Grades 7, 8 and 9. All the students within the selected classes were eligible for participation regardless of their actual ages. The school response rate was 100%, the student response rate was 78.3%, and the overall response rate was 78.3% 9. Data collection Students took between 30 to 45 minutes to complete the questionnaire. All questions were presented as multiple choice options and were completed at a single sitting. The GYTS core questionnaire aims to collect the following information: prevalence of cigarette smoking and other tobacco use; knowledge and attitudes towards cigarette smoking; role of the media and advertising on use of cigarettes; access to cigarettes; amount of pocket money received each day and amount of money spent on cigarettes, tobacco-related school curriculum; environmental tobacco smoke (ETS) and cessation of cigarette smoking 10. A comprehensive description of the GYTS methodology has been reported elsewhere. 11-13 For the purpose of this study however, only data related to factors associated with the history of ever smoked contained in the literature are reported. Having ever smoked was defined as having ever smoked even a single puff in one's life time. Ethical consideration: Permission to conduct the study was obtained from the Ministry of Education. All eligible students were also informed that participation was voluntary. Data collection was facilitated in schools by trained assistants without the presence of the teacher. The questionnaire was anonymously self-administered by the students. Data analysis: Data were analyzed using SPSS version 14.0 (2005 SPSS Inc). Factor specific prevalence rates of ever smoked cigarettes are reported. The Yates corrected Chi-square test in 2x2 tables, the Pearson's Chi-square test in higher tables, and odds ratios with their 95%CI were used to establish unadjusted associations between the explanatory factors and the outcome. Weighted logistic regression analyses were performed to determine associations between selected factors according to literature and ever smoked status. Backward logistic regression analyses were conducted to determine independent factors associated with ever smoked cigarettes. The results of bivariate analyses are reported in the tables as Model 1, while the results of the multivariate analyses are reported as Model 2. A weighting factor that was used in the analysis to reflect the likelihood of sampling each student and to reduce bias by compensating for differing patterns of non response was computed using the following equation: W = W1 * W2 * f1 * f2 *f3 *f4 where W1 is the inverse of the probability of selecting the school; Results Prevalence of history of ever smoked A total of 2175 students participated in the study out of which 40.1% (95%CI 39.5-40.7%) had ever smoked cigarettes (43.4% (95%CI 42.6-44.2%) of the boys, and 35.6% (95%CI 34.8-36.4%) of the girls ever smoked cigarettes (p<0.001). Because of the sex difference in the ever smoked status, the proceeding analyses are stratified by sex. Demographic characteristics and history of ever smoked Associations between history of ever smoked and age, school grade, parental smoking status and closest friend smoking status were determined and the results are presented in Table 1a and 1b, for boys and girls, respectively. Among both boys and girls, parental and closest friend smoking were independent predictors of ever smoked. Boys and girls with either parent who never smoked were 18% (OR=0.82, 95%CI 0.69-0.97) and 57% (OR=0.43, 95%CI 0.54-0.60) less likely to have ever smoked, respectively, than those students with either parent who smoked. Compared to boys and girls who had most or all of their closest friends who smoked, those with closest friends who did not smoke were 48% (OR=0.52; 95%CI 0.41, 0.68) and 64% (OR=0.36; 95%CI 0.34, 0.39), respectively, less likely to ever smoked. Perceptions towards smoking and history of smoking We also assessed associations between perception that cigarette smoking is harmful to their health, smoking makes people comfortable, perception that smoke from other peoples' cigarettes is harmful to their health, whether the study participants would let someone smoke in their presence or would favour public smoking ban on one hand and history of ever smoked on the other. The results are presented in Table 2a and 2b. None of these factors were independently associated with having ever smoked among boys. However, perception that cigarette smoking is harmful to their health, smoking makes people comfortable, letting someone smoke in their presence, and favours public smoking ban were independently associated with having ever smoked among girls. Girls who said that probably smoking is harmful to their health or not were more likely to have ever smoked (OR=1.26, 95%CI 1.12-1.41), OR=1.47, 95%CI 1.32-1.64, respectively) than those students who definitely said that smoking is harmful to their health. Furthermore, girls who reported that smoking makes people less comfortable were 26% (OR=0.74, 95%CI 0.69-0.79) less likely to have ever smoked compared to girls who said that there was no difference from non-smokers. Girls who would let someone smoke in their presence were 30% (OR=1.30, 95%CI 1.22-1.39) more likely to have ever smoked compared to their counterparts who would not let someone smoke in their presence. Finally, girls who were in favour of public smoking ban were 11% (OR=1.11; 95%CI 1.06, 1.17) more likely to have ever smoked compared to girls who were not in favour of public smoking ban. The role of tobacco advertisements and smoking We also assessed whether having an item with a cigarette brand logo and having been exposed to cigarette advertisements at sports or other social events were associated with having ever smoked cigarettes. The results are presented in Table 3a and 3b. Compared to girls who were never exposed to cigarette advertisements at sports or other social events, girls who were a lot more exposed to cigarette advertisements at these events were 30% (OR=1.30, 95%CI 1.18-1.44) more likely to have ever smoked. However, being exposed to a lot more to cigarette advertisements was not associated with ever smoked cigarettes among boys. Girls who had an item with a cigarette brand logo on it were 32% (OR=1.32, 95%CI 1.23, 1.41) more likely to have ever smoked compared with girls who had items with no cigarette brand logo on them. Discussion Our study reported a prevalence of history of having ever smoked cigarettes among school going adolescents in Lusaka, Zambia at 40.1%. Boys were more likely to have ever smoked cigarettes than girls (43.4% boys versus 34.9% girls). Although in this study, we found that males were more likely to have smoked cigarettes than females, globally the situation is diverse in that in some countries, there is male predominance while in others, no such male predominance exists.14 However, our finding is similar to the one reported in the sub-Saharan Africa by Townsend et al 3 that the prevalence of tobacco use was higher among males than among females across all countries in the region. We also found that adolescents who had closest friends who were smokers were more likely to have ever smoked cigarettes themselves.15-17 The reason for this observation could be due to peer selection in that smokers were more likely to befriend other smokers. The alternative explanation could be that there is peer influence in that non-smokers are likely to be influenced to initiate smoking if they have a friend who smokes. Urberg et al 18 have reported that smokers were likely to overestimate smoking status among their friends i.e. smokers were likely to report their friends as smokers when they were not. We do not have evidence from our data to confirm or dispute any of these possibilities. We however believe that all these explanations are plausible and could be operating at the same times. Adolescents whose parents were smokers were also more likely to have ever smoked themselves. Several studies have reported the association between parental smoking and adolescent smoking. 19-23 Interventions to prevent smoking among adolescent should incorporate the fact that parental influence may be a factor. Parental smoking may affect adolescent smoking by parents being role models, failure by smoking parents to discourage the practice and the ready availability of cigarettes at home. This study also explored the role of advertisements and their associations with adolescent smoking. There is evidence that tobacco firms continue to target adolescents and young adults. 24 Sargent et al and 25 Dalton et al 26 have reported on the association between adolescent smoking and watching movies depicting some character who was smoking. These findings however are in contrast to the situation reported in 1974 that the Zambian government had banned tobacco advertisements on radio. 27 Our study conducted about three decades later shows that many adolescents continue to be exposed to pro-tobacco advertisements. Our study has several limitations. First data collection was limited to school-going adolescents and so may not be representative of all adolescents in Lusaka, Zambia. Also the data were self-reported and so mis-reporting is possible whether deliberate or inadvertent. We cannot ascribe causation to our observed associations from the nature of our study design. Conclusions The proportion of adolescents who had ever smoked cigarettes in Lusaka, Zambia was 43.4% for boys and 35.6% for girls. Parental smoking and closest friend smoking were associated with history of ever smoked among both sexes of this group. Exposure to pro-tobacco advertisements was also associated with history of ever smoked among girls. Public health intervention aimed to prevent initiation of smoking and encourage cessation of smoking should be guided by a comprehensive understanding of the determinants of smoking. We can have more confidence on the nature of the associations if cohort studies could be conducted. Acknowledgements We are grateful to Richard Zulu who coordinated the collection of data. The GYTS is a collaborative project of WHO/CDC/participating countries. Analyses of GYTS data are not necessarily endorsed by the WHO/CDC/participating countries. We are thankful to the study participants and research assistants References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07047t3b.jpg] [hs07047t2b.jpg] [hs07047t2a.jpg] [hs07047t1b.jpg] [hs07047t3a.jpg] [hs07047t1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}