 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
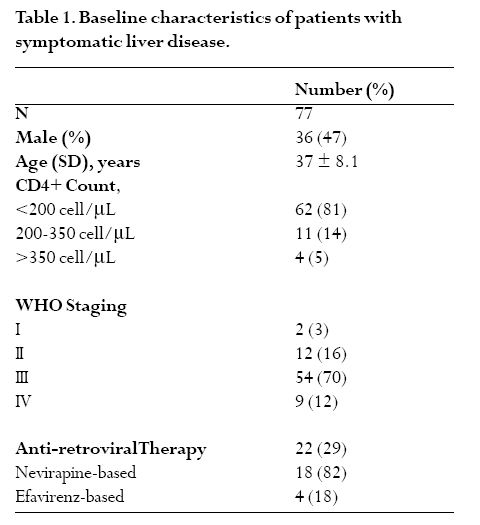
African Health Sciences, Vol. 8, No. 1, March, 2008, pp. 8-12 The spectrum of liver diseases in HIV infected individuals at an HIV treatment clinic in Kampala, Uganda Ponsiano Ocama1, Michael Katwere, 1 Theresa Piloya, 1 Jordan Feld2, Kenneth C Opio3, Andrew Kambugu, 1 Elly Katabira1, David Thomas4 , Robert Colebunders, 5 Allan Ronald1 1Infectious Diseases Institute, 2National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), 3Departement of Medicine, Makerere University, 4Johns Hopkins University, 5 Institute of Tropical Medicine and University of Antwerp Code Number: hs08004 Abstract Background: Liver diseases are common in patients with HIV due to viral hepatitis B and C co-infections, opportunistic infections
or malignancies, antiretroviral drugs and drugs for opportunistic infections. Introduction Hepatobiliary diseases occur commonly in patients with human immunodeficiency virus (HIV) infection and are now the commonest causes of death in HIV positive patients on antiretroviral therapy (ART) in western countries.1,2 Liver enzyme abnormalities have been reported in 20 - 93% of HIV-infected populations. 3, 4 The common causes include opportunistic infections, malignancies and drug toxicities. Due to both common modes of transmission and geographic patterns of disease, hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV frequently occur as concomitant infections. 5,6 All classes of antiretroviral therapies (ART) can induce liver toxicity but the probability and extent of injury varies substantially with the individual agents.7,8,9 In addition to the antiretroviral drugs, other frequently prescribed medications for the management of opportunistic infections including anti-tuberculous drugs may cause hepatic injury.10 Liver disease etiology in HIV-1-infected persons in sub-Saharan Africa may differ from what has been described in the West and may change with the recent expansion of access to ART. We designed a study to characterize the causes of liver disease among HIV- infected individuals attending the Infectious Diseases Clinic (IDC) in Kampala, Uganda. Patients and Methods The study was carried out over 11 months from May 2004 to March 2005 at the Infectious Diseases Clinic, a specialized unit for HIV care within Makerere University Medical School. During this interval, ART use expanded markedly coincident with the widespread availability of free ART. ART consisted of either the generic fixed drug combination: stavudine, lamivudine, and nevirapine (Triomune) or zidovudine, lamivudine, and efavirenz. Consecutive patients were referred by the medical staff to one of two study physicians if they had newly recognized signs or symptoms possibly indicative of liver disease including any or a combination of the following: a) jaundice, Those providing informed consent were enrolled in the study and a questionnaire focused on liver disease was administered. Liver enzymes (alanine aminotransferase (ALT), aspartate aminotransferase (AST) alkaline phosphatase (ALP) and gamma glutamyl transpeptidase (GGT), hepatitis B surface antigen (HBsAg) and anti-hepatitis C antibody were obtained, and all patients underwent abdominal ultrasound. Based on liver enzyme results and considering upper limits of normal (ULN), patients were classified into established patterns of liver injury: cholestatic (ALP/ULN:ALT/ULN>2), hepatocellular (ALT/ULN:ALP/ULN>2) mixed pattern (ALP/ALT ratio of 0-2) or normal pattern (ALP and ALT <1.3xULN). Stool analysis was performed in patients with cholestatic liver enyme pattern while ultrasound guided liver biopsies were performed in those patients with liver masses (nodules). No significant complications of liver biopsy were noted. On the basis of these tests and information from the questionnaire, diagnosis was classified as definite, probable or possible. Diagnoses of hepatocellular carcinoma and hepatic adenoma were made on histology. The study was approved by the Scientific Review Committee of the Infectious Disease Institute and Makerere University Faculty of Medicine Research and Ethics Committee. Results By end of the study 8,715 patients were registered at the IDC 5,585 (64%) being females; 1,560 (18%) were on ART. Out of all these patients 1,485 (95%) were on first line regimen with nucleoside reverse transcriptase inhibitor (NRTI) based regimen, 846 (57%) on nevirapine and 692 (43%) on efavirenz. One hundred eighty seven patients were on isoniazid (INH) either as prophylaxis (5 patients) or for treatment of tuberculosis (182 patients). A total of 77 (0.8%) of 8,715 patients presented with apparent symptomatic liver disease during the study period and all agreed to study participation. The baseline characteristics of the patients enrolled are shown in Table 1. Twenty-two (29%) of these patients were on ART; 18 (82%) of whom were on a nevirapine-containing regimen while 4 (18%) were on an efavirenz-based regimen. Thirty six patients were male (47%, p=0.049, 95% confidence interval= 0.97- 2.51), and the majority (81%) had severe immunosuppression with CD4+ counts below 200 cells/µl. Symptoms at presentation Thirty nine (51%) patients presented with jaundice either alone in 19 (25%) patients or in combination with other features. Right upper quadrant pain was the most common presenting complaint occurring in 48 (63%) patients. Ascites was documented in 16 (21%) individuals (Table 2). Liver enzyme patterns Investigations revealed that the majority 48 (63%) of patients had a cholestatic pattern of liver enzyme elevation with a mean 7 fold increase in ALP (range 1.3-38) (Table 2). Six (8%) patients had a hepatocellular liver enzyme pattern with a 2-36-fold increase in ALT levels. Another 15 (19%) patients had a mixed picture while 8 (10%) patients had normal liver enzymes and abdominal ultrasound scans. Hepatitis B and C serologies were negative in all 8 patients. None of them was investigated further and during the follow up none of these subjects developed further evidence of a specific liver disease. Spectrum of liver disease The presenting symptoms, liver enzymes and baseline clinical data for the most common diagnoses are compared in Table 2. Twenty-three of the patients (30%) who met the inclusion criteria had a diagnosis of either nevirapine or INH toxicity as the cause of their liver disease including 4 patients on both drugs where the specific culprit could not be determined. Although 14 (61%) patients presented with jaundice, all recovered on discontinuation of the presumed offending drug(s). Nevirapine alone led to greater elevations of ALT (443 vs 92 IU/l, p=0.007) and ALP (733 vs 380 IU/l, p=0.14) compared to INH but the latter was more likely to cause jaundice (3/8 vs 8/11, p=0.13) (Table 2). Co-infection with HBV was common with 11 (15%) patients testing positive for HBsAg. However, hepatitis B was considered to be the sole cause of admission into the study in 8 (11%) of these patients. One of these co-infected patients was on both INH and nevirapine and improved on stopping the drugs while 2 others presented with histologically proven HCC. Three other patients presented with HCC in the absence of positive HBV serology. Co-infection with HCV occurred in only 2 enrollees and was not implicated in any adverse outcome. Probable granulomatous hepatitis was diagnosed in 7 (9%) patients. The diagnosis was made on the basis of marked elevation of ALP (mean 2147 IU/l), an enlarged liver on ultrasound scan, and clinical features of tuberculosis (TB) including recurrent fever, loss of appetite and weight loss but without biopsy or culture. All 7 patients were treated for tuberculosis and all resolved with no evidence of any other hepatic disease. Presumably all seven patients had hepatic tuberculosis. Additional hepatic diagnoses included alcoholic liver disease in 4 (5%), AIDS cholangiopathy in 1 (1%), schistosomiasis in 1 (1%), haemangioma in 1(1%), hepatic adenoma in 1(1%) and liver disease of unknown origin in 13 (17%). All but one of these latter patients had a CD4+ count less than 200 cells/μl and had either cholestatic (8) or a mixed liver enzyme picture (5). All patients with HCC presented with a cholestatic/mixed pattern and an abdominal (liver) mass and 2 presented with associated right upper quadrant pain. Twelve patients died during the course of the study. Seven of the patients died of liver disease (4 due to HCC and 3 with end-stage liver disease). The remaining patients died of various other causes including renal failure (1), disseminated Kaposi’s sarcoma (1) and lymphoma (1) while 2 died of unknown cause. Discussion Investigating liver disease in resource-constrained settings is complicated due to limited access to laboratory testing, ultrasound examination and liver biopsy for histological examination. Therefore to date very few studies have addressed the causes of liver disease among persons with HIV infection in tropical countries.11 At the clinic of the Infectious Diseases Institute in Kampala we were fortunate to be able to perform certain tests but complete investigation of our patients with HIV infection presenting with liver disease was still not possible. This study differs from most evaluations of liver disease in HIV-infected populations because only symptomatic patients were included. Most studies have described patients with asymptomatic liver test abnormalities found as incidental findings during screening or investigations for other conditions.1,2 Therefore, although our reported incidence of <1% may appear low this represents only patients with liver injury significant enough to cause symptomatic disease and may still lead to a large burden of disease given the high prevalence of HIV infection. Hepatotoxicity due to nevirapine and/or INH was the most frequent diagnosis. All these 22 individuals made a complete recovery with no clinical evidence of ongoing hepatic illness at six months after the drug was discontinued. Immediate discontinuation and replacement with alternative medication is probably the preferred option when patients present with clinical illness possibly due to drug induced liver injury. Second, granulomatous hepatitis presumably due to tuberculosis was common. Although liver biopsies were not performed, patients improved on anti-tuberculosis treatment. Infection with Mycobacterium tuberculosis has been demonstrated to be the commonest cause of granulomatous hepatitis in HIV infected patients.1 In resource poor settings clinicians often hesitate to initiate anti-tuberculosis treatment in patients presenting with jaundice. In this study 3 of the 7 patients had jaundice at presentation, all 7 had a marked elevation of ALP and all improved with anti-tuberculosis treatment. Hepatitis B surface antigen was positive in 11 (15%) of the patients. Unfortunately, in most resource limited settings patients are not routinely investigated for HBV infection prior to initiating HAART. Most first line ART regimens include lamivudine and if HBV is present, acquisition of HBV resistance to lamivudine is high.12 Other drugs including tenofovir are effective against the wild type and lamivudine resistant strains of HBV13 but studies to select optimal treatment for co-infected individuals in Africa are required. All patients who present with right upper quadrant pain and/or jaundice require investigation for HBV, particularly to rule out the presence of HCC. Ideally HBV serology should be evaluated prior to starting ART to help guide therapeutic decision-making. HCV was uncommon, occurring in only 2 of the patients. Other studies have shown a similarly low HCV prevalence in many resource limited settings.14,15 Testing for HCV among patients with HIV infection in Uganda may not be cost-effective. Hepatocellular carcinoma is a common malignancy in Uganda and other parts of the world presumably due to HBV and perhaps other carcinogenic agents including alcohol and aflatoxin. 16,17 Further studies are needed to determine if HCC occurs more commonly in HIV-infected individuals both with and without HBV co-infection. This is particularly important given the high prevalence of resolved HBV infection (anti-HBc positivity). Gall bladder disease, parasitic liver infections particularly schistosomiasis, cholangiopathies, and liver abscess all need to be considered in the differential diagnosis of hepatic `clinical presentations' and each occurred in our series but they were infrequent. In conclusion among an HIV-infected population, drug history, liver enzyme studies, abdominal ultrasound, and HBV and HCV investigations identified the probable etiology in 60 (78%) of 77 patients presenting with symptoms and/or signs of liver disease, with good outcomes and return to normal hepatic function in the majority of patients. Acknowledgments: We acknowledge The Bill and Melinda Gates Foundation for funding this study, Dr Barabara Catelnuovo for her input in the manuscript, the Director of the Infectious Diseases Institute Prof Keith McAdam for supporting this work, the staff and the study patients Potential conflict of interest: None directly relating to this study for all the authors References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08004t2.jpg] [hs08004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}