 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 1, March, 2008, pp. 20-24 Lymphoreticular diseases in Nigerians Adelusola Kayode A, *Sabageh Donatus O, **Ukah Cornelius O. Department of Morbid Anatomy and Forensic Medicine, Obafemi Awolowo University, Ile-Ife, Nigeria. Code Number: hs08006 Abstract Background: The lymphoreticular system plays a major role in both the innate and adaptive immune responses. This study
reviews retrospectively cases of lymphoreticular diseases seen at a tertiary institution in Nigeria. Key Words: Non Hodgkin's lymphoma, Splenectomy, Bone marrow. Introduction The lymphoreticular system consists of the primary lymphoid organs (bone marrow and thymus), the secondary or peripheral lymphoid organs (lymph node, spleen and peyer's patches) and the tertiary lymphoid organs, which include acquired lymphoid organs in the skin, respiratory and reproductive tracts in response to local antigenic stimuli1. Infectious agents, immunologic reactions and various other stimuli may cause reactive changes in lymphoreticular organs, notably the lymph node, many of which are non specific. Some of these reflect the underlying abnormalities of the immune system and cell control processes, while others are related to viral infections of unknown cause 2. Benign non specific reactive changes may also involve the bone marrow and the spleen. Sometimes a cellular component of the organ is predominantly involved, as in follicular hyperplasia in lymph node and the spleen, and reactive erythroid hyperplasia in bone marrow. Some reactive changes can mimic malignancy or progress to malignancy 3. Malignant diseases can also secondarily involve any of the lymphoreticular organs. Literature on lymphoreticular diseases among Nigerians and Africans in general is very scarce and addresses mainly lymph node diseases4,5 This paper attempts to analyse all categories of lymphoreticular diseases (benign and malignant) seen in a university teaching hospital in Nigeria within a period of 16 years and to highlight the variation in disease pattern with age and sex. Materials and methods Obafemi Awolowo University, Ile-Ife in Nigeria is a tertiary health institution with 576 beds. It serves a population 1,333,603 with a slight female predominance (1991 census) of the Ife-Ijesa area of Osun state, Nigeria. Surgical biopsy specimens of patients with lymphoreticular diseases sent to the histopathology department of the university within the 16-year period from January 1988 to December 2004 formed the basis of this report. These were segregated into three categories:
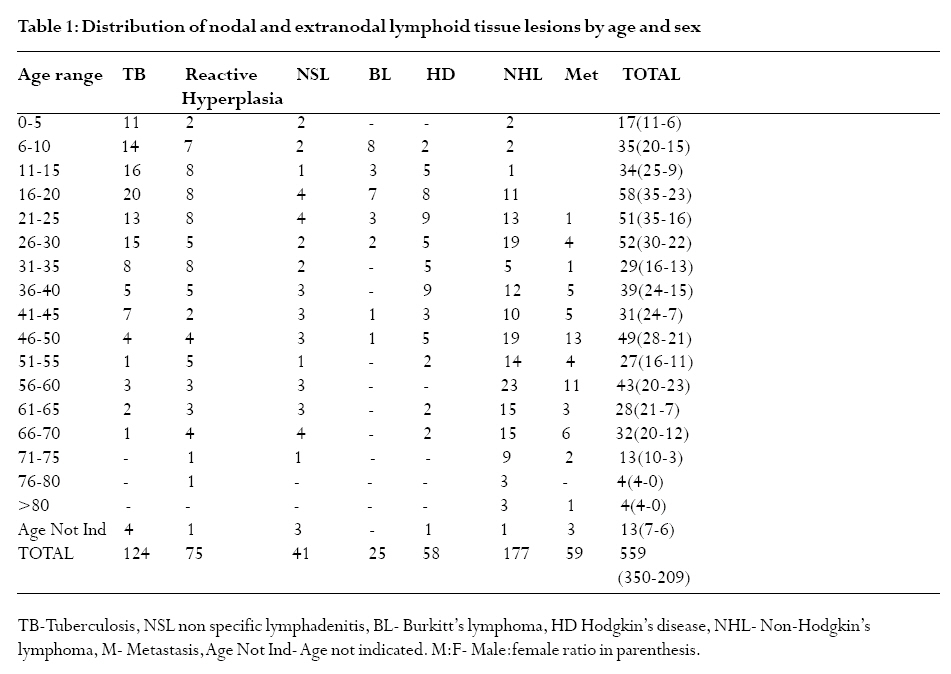
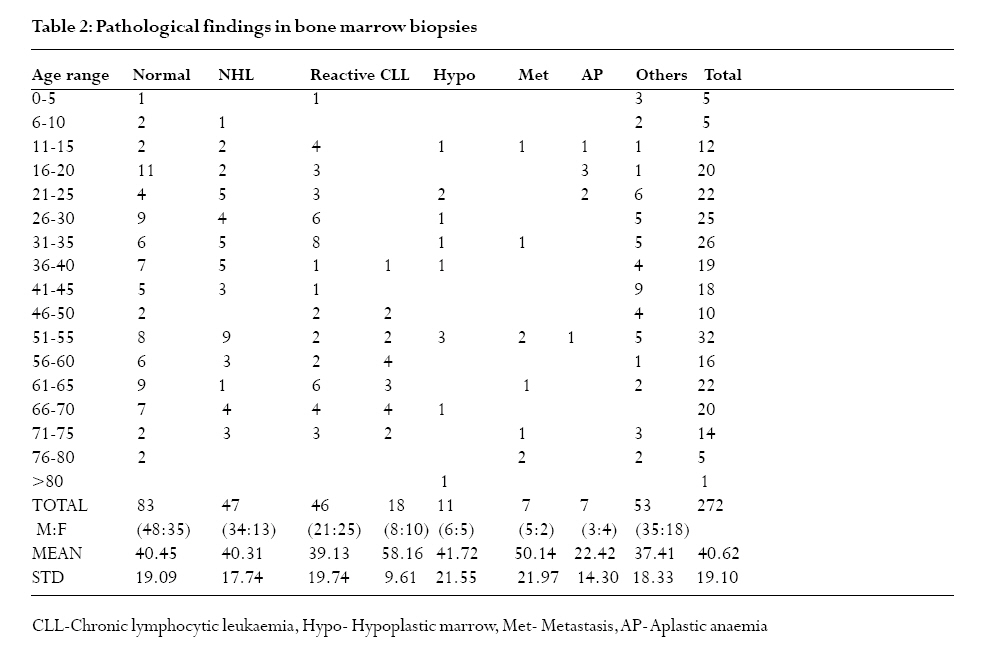
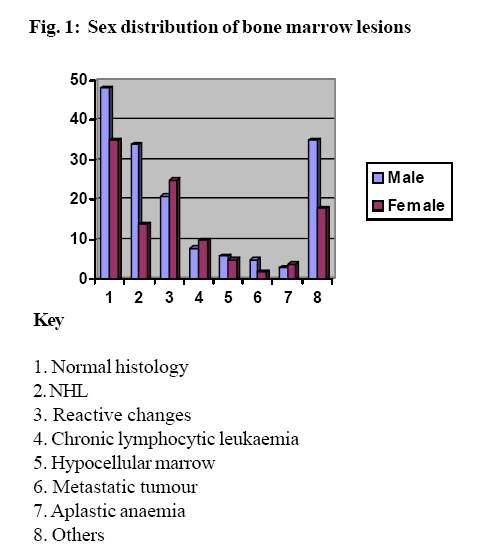
The lymph node biopsies were mainly excisional. All biopsies were routinely fixed in 10% formal saline, embedded in paraffin wax, and stained routinely with haematoxylin and eosin. Bone marrow trephine biopsies were taken from the posterior iliac crest and decalcified with formic acid before routine processing. The surgical biopsy reports and the request cards of the patients were scrutinized and the demographic data as well as the histological diagnosis were extracted. The slides were retrieved, reviewed and new sections were cut in some cases. Special stains such as Ziehl-Neelsen stain, Giemsa, Periodic acid Schiff and Perls' reaction for iron were used to reach a conclusive diagnosis in some cases. Cases lacking adequate data or with no clear-cut diagnosis whose slides cannot be retrieved for reassessment were excluded from the study. Statistical analysis was performed for differences in proportion using Chi square (p is significant at <0.05) by SPSS version 12. The mean and standard deviation were also calculated where relevant. Results There were 944 cases consisting of lymph node and extranodal lymphoid tissue (n=559), bone marrow (n=272), spleen (n=113) and lymph node metastases (n=59). Overall, male predominated over female. Lymph node and extranodal lymphoid tissue Overall there were 559 cases (348 males and 211 females). The age range was 1.5 years to 87 years, (mean 35.73 and STD 20.19). Table 1 shows the distribution of the lesions by age and sex. Non-Hodgkin's lymphoma (NHL) was the predominant lesion, followed by tuberculosis, non-specific lymphadenitis and others. Twenty four cases of NHL occurred at extranodal sites (10 in the GIT, 5 in the skin, 3 in the testis, 2 each in the salivary glands and the nasopharynx and 1 each in the maxillary antrum and the nose). Twenty five cases of Burkitt's lymphoma (BL) were extranodal (17 in the jaw, 4 in the breast, 3 in the ovary and one in the testis). The breast cases were aged 20, 22, 24 and 40 years. Three of these were bilateral, one of them occurred in a pregnant woman (age 20). There was a male predominance for all disease categories. Immunophenotyping of 46 of the NHL cases showed 35 were diffuse large B-cell lymphoma. The rest were: T- cell lymphoma-5, follicular lymphoma-4, nasal T/NK cell lymphoma-1 and 1 null cell ALCL. Two of the patients with NHL, both male and aged 27 and 40 years were documented to have AIDS. Most of the other cases not immunophenotyped are of the centrocytic/centroblastic variants. There were 59 cases (30 males and 29 females) of metastasis to lymph nodes (Table 1). Axillary nodes accounted for 19 cases (17 from breast cancer and 2 of unknown origin). The cervical lymph nodes accounted for 18 (from nasopharyngeal carcinoma and salivary gland-3 each, from the thyroid 2 and one of gastric origin and 9 from unknown primary origin). Ten cases were seen in the inguinal nodes, mainly from melanoma on the foot. There were also metastasis to the mesenteric lymph nodes (5), omentum (3) and others (4). The category of reactive hyperplasia (Table 1) are cases showing the basic reactive patterns in a lymph node (follicular hyperplasia, paracortical expansion, sinus histiocytosis). Bone marrow There were 272 cases with 160 males and 112 females (Table 2). 30.5% of the bone marrow biopsies were essentially normal on histology. Non-Hodgkin's lymphoma and reactive changes were the most common pathologic findings. Patients with chronic lymphocytic leukaemia had the highest mean age and there was a significant difference in age between those with CLL and those with NHL (p = .001; 95% confidence interval -27.91 to -7.76). Findings listed as others included: chronic myelocytic leukaemia, myelofibrosis, multiple myeloma, plasmacytoma, polycythaemia vera and Hodgkin's disease. Fig 1 shows the sex distribution of bone marrow diseases. With the exception of reactive changes and aplastic anaemia, males predominated in all disease categories. The spleen This consisted of 113 cases (74 males and 39 females). All were splenectomy specimens. The age range was 1 to 86 years (mean 34.8 STD 19.6). There were 71 cases of splenic rupture. Road traffic accident accounted for 59 of these, gunshot wound (5) and 7 other cases which are: falls from height (3), acute abdomen (2) and blunt abdominal injury due to affray (2). There were 42 other pathological findings not associated with splenic rupture. These were: chronic lymphocytic leukaemia (13 cases), hypersplenism of unknown cause (7), lymphoma (5), sickle cell disease (4), metastatic carcinoma (2), splenic infarct (2), a case each of essential thrombocytopaenia, hereditary spherocytosis, splenic abscess, splenic congestion of unknown cause, histoplasmosis, lipidosis and essentially normal spleen (3). The peak age incidence for splenectomy was 21-25 years, although the rate was also high in other age groups (6-10, 31-35 and 56-60). The highest mean weight (2289gm) was for spleen involved with chronic lymphocytic leukaemia. The mean weight for spleen involved with traumatic rupture was 298.3gm. Cut surfaces of these spleens showed haemorrhage and necrosis. Histology in addition to haemorrhagic necrosis showed trabecular fibrosis and haemozoin pigment in many cases. Discussion The diversity of the lesions seen in this report reflects the ability of the lymphoreticular system to undergo various pathological changes depending on the nature of the stimulus and the body's reaction to it. This is probably the first report on this subject in Nigerians. The Obafemi Awolowo University Teaching Hospital, Ile-Ife, where this study was carried out is a referral centre and the only hospital with histopathology services in Ife-Ijesa area. Its histopathology department receives and processes between 1600 and 1800 biopsies per year, mainly from the Ife-Ijesa area of Osun state but also from neighbouring states with no well established histopathological services. In this report 944 cases of lymphoreticular diseases were studied. Patients with lymph node and bone marrow biopsies accounted for the majority of cases. This may in part be due to the superficial location of most of the lymph nodes in this report and the relatively simple and inexpensive technique of excisional lymph node biopsy. There is a high male:female ratio for all disease categories except for metastases to lymph nodes; due to the number of cases of breast cancer metastasis to the axillary nodes. The predominant lesion in lymph node and extranodal lymphoid tissue is NHL, followed by tuberculosis, the former showing a high male:female ratio. This is in sharp contrast to the study of Sibanda et al5 in Zimbabwe where NHL constituted just 7% of the nodal lesions studied. This is probably because their study did not include extranodal lymphoid tissue. HIV/AIDS because of severe immuno-suppression is known to be associated with lymphoma.6. Only two of the patients in this study were known to have AIDS. Since HIV test is not routinely done on all patients in our hospital, it can be assumed that some more cases would have been HIV-positive, if tested. Lymphoma is not the only nodal lesion associated with HIV/AIDS. Reactive changes such as follicular hyperplasia, follicular lysis and involution are all benign lymph node lesions associated with various stages of HIV/AIDS. None of the patients with reactive changes in this study was documented to have HIV or AIDS. Again this may be due to the fact that they were not routinely screened for HIV. Prominent among other factors that could predispose to lymphoma in Nigeria is exposure to petrochemicals.7 The habit of siphoning fuel from plastic cans into vehicle tanks by siphoning is common at periods of fuel scarcity and is habitually practised by motor mechanics. Other important factors that could predispose to lymphoma include the hepatitis C virus8 and the Epstein-Barr virus9. Some studies, however, have found no association between hepatitis C virus and NHL10. The contribution of these factors to the burden of lymphoma in Nigerians at present is not known. The high incidence of Burkitt's lymphoma in tropical Africa and its occurrence at extranodal sites are well known. However, most of the cases in our hospital are diagnosed by haematologists and do not get to the histopathology department. Moreover, Burkitt's lymphoma rarely affects the lymph node in endemic areas. Four of the cases in this report were seen in the adult female breasts. Lymphoma of the breast is known to have a poor prognosis, regardless of the treatment modalities 11. The incidence of tuberculosis in lymph node was high up to the age of 30 years, and thereafter decreases. As from the age of 25 years the incidence of NHL starts to rise. The rare coexistence of TB and Hodgkin's lymphoma has been reported in the cervical lymph nodes.12 The basis for this is probably immuno-suppression associated with both entities. The prevalence of tuberculous lymphadenitis among Nigerians had been reported by Oluwole et al 13, who also noted a high incidence in the cervical lymph nodes. Poverty and worsening socio-economic condition coupled with lack of quality health care and HIV/AIDS are some of the factors that could explain the high incidence of tuberculosis in this report. HIV infection, which is common in Nigeria is the most powerful risk factor for progression from latent infection with mycobacterium tuberculosis to active tuberculosis14. Bone marrow biopsies accounted for a large number of cases in this report. The biopsies were most often done for the evaluation of lymphoma and various forms of anaemia. The diagnosis of lymphoma in bone marrow could be challenging as benign lymphoid aggregates seen in the elderly also has to be considered. Absence of germinal centres, B- or T-cell gene rearrangement by molecular analysis all favour a diagnosis of lymphoma. A number of cases are hypocellular. Bone marrow cellularity depends on age and is 100% at birth. Thereafter it decreases by 10% per decade. The causes of marrow hypoplasia are many and they include sampling errors, artefacts, viral infections including EBV and HIV, drug toxicity etc. Bone marrow hypoplasia is one of the features of chronic exposure to benzene15. All biopsies of the spleen in this report were from splenectomy specimens and the most common reason for splenectomy was splenic rupture in road traffic accident (RTA). Splenic rupture with haemoperitoneum from RTA is an important reason for splenectomy in Nigeria16-17. The studies of Adejuyigbe et al.18 and Ameh et al.19 showed that most abdominal injuries in Nigerian children were due to blunt trauma, mainly from RTA, most of which result in splenic injury. Males are more aggressive than females in economic activities and other activities involving frequent travelling. Women are expected to look after the home while men are busy trying to provide the needs of the family. This may be one of the reasons why men are more involved in RTA and consequently splenic laceration than females. Secondary lesions in lymph nodes are in the form of metastases. In this report, there is a female preponderance due to the frequent involvement of the axillary lymph node by carcinoma of the breast. Because most cases of melanoma in Africans occur on the foot, the inguinal lymph node is commonly involved, as in this report. This report highlights the high rate of occurrence of NHL as the most common lymphoreticular disease among Nigerians. The incidence increases with age and males are more vulnerable. The fact that 30.5% of bone marrow biopsies in this report were normal on histology calls for some caution in the selection of case for bone marrow biopsies. It is also possible that techniques such as flow cytometry and immunohistochemistry may detect lesions in a few cases reported as normal. Provision of such facilities at least in a few referral centres should be one of the priorities of the government. Unnecessary splenectomies in the absence of pathological lesions in the spleen must also to be avoided. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08006f1.jpg] [hs08006t2.jpg] [hs08006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}