 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
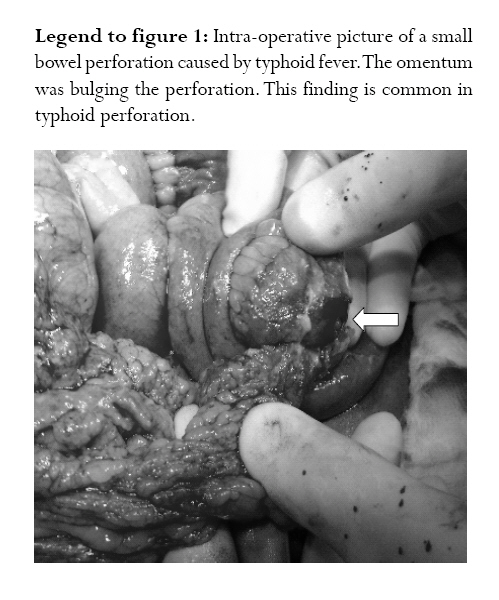
African Health Sciences, Vol. 8, No. 1, March, 2008, pp. 36-39 Non-traumatic perforation of the small bowel Hani O. Eid1, Ashraf F. Hefny2, Sandhya Joshi3, Fikri M. Abu-Zidan1 Department of
Surgery1, Faculty of Medicine and Health Sciences, United Arab Emirates University, Al-Ain, United Arab
Emirates, PO Box 17666, Departments of
Surgery2 and Pathology3, Al-Ain Hospital, Al-Ain, United Arab Emirates, PO Box 1006 Code Number: hs08008 Abstract Background: Non-traumatic perforation of the small bowel is an uncommon serious complication associated with high morbidity
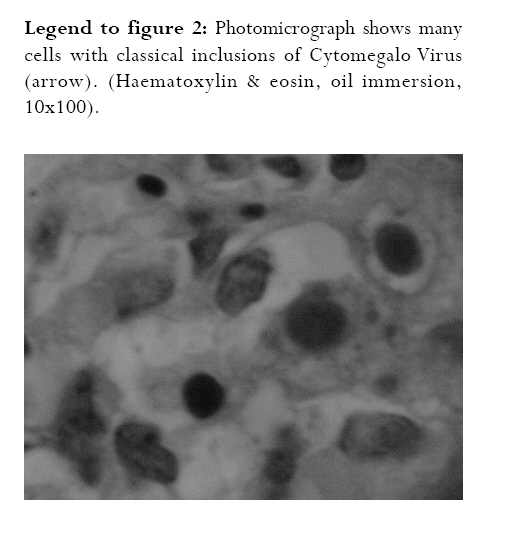
and mortality. Diseases that cause small bowel perforation vary in different areas of the world. Key words: HIV, hook worms, small bowel perforation, tuberculosis, typhoid. Introduction Non-traumatic small bowel perforation is uncommon but can be fatal. Typhoid fever and tuberculosis are the common causes of such perforation in the developing countries, while in western countries non-infectious pathology is more common1, 2, 3. Peritonitis following perforation may lead to multi-organ failure and death unless it is treated promptly and vigorously. United Arab Emirates is a developed country. Al-Ain City has a population of about 472,000.4 A well developed water supply and safe disposal of waste in the city has almost eliminated typhoid fever. HIV screening is mandatory for all residents in the country by law. Al-Ain Hospital is one of the two main hospitals serving the city. Herein, we have retrospectively studied four cases of non-traumatic small bowel perforation that were managed in our hospital. We aimed to highlight difficulties in diagnosis and management of non-traumatic perforation of the small bowel in our setting. Case One A forty-seven year old man presented with abdominal pain and intermittent fever of one month duration. The pain became more severe in the last 2 days and was associated with nausea and vomiting. The temperature of the patient was 37 ºC, pulse 113 per minute and blood pressure 105/70 mmHg. The abdomen was slightly distended, soft with generalized tenderness. Bowel sounds were audible. White blood cell count was 8x109/L. Lymphocytes were increased (40%). Serum electrolytes, blood sugar, and serum bilirubin were all normal. Serum amylase was mildly raised (231 U/L). Chest X-ray has shown air under diaphragm. A laparotomy has shown a punched-out perforation of the ileum at midpoint (Fig 1) with free fluid in the peritoneal cavity. The ulcer was excised; the defect was closed in two layers. Histopathological examination has shown few scattered aggregated epithelioid cells poorly forming granulomas, without obvious caseation. Special stains have failed to reveal any organism. Blood cultures were negative. Clinically, the patient was diagnosed as typhoid fever and was treated with intravenous broad spectrum antibiotic (Meronem 1 gm 8 hourly for one week followed by Ciprobay 400 mg 12 hourly for four weeks). The patient was discharged home in the 8th postoperative day in a good condition. Case Two A thirty-year old man presented with colicky abdominal pain of two days duration. On examination, the patient had a temperature of 37.6 ºC, pulse 88 per minute and blood pressure of 110/70 mmHg. Abdominal examination revealed generalized guarding and tenderness. His white blood cells count was 9.8 x109/L. Serum electrolytes, blood sugar and serum amylase were all normal. Erect chest X-ray was normal. Urgent abdominal ultrasound and CT scan were also normal. Laparotomy was decided after 6 hours of observation. Midline laparotomy has shown a pin-hole perforation at the mesenteric border of the ileum 10-15 cm from the ileocaecal junction. Another two non-perforated erosions with elevated borders, were felt manually during surgery. The tissue around the perforation was excised and the defect was closed in two layers. The other 2 ulcers were buried using seromuscular stitches. The patient was discharged home on the 6th postoperative day in a good condition. The histopathological examination has shown a non-specific ulcer of the small intestine with many eosinophils. Stool examination has shown ova of hook worms. The patient was treated with a single dose of Mebendazole. Case Three A 75-year old man has presented with lower abdominal pain of two days duration. The patient was dehydrated; his temperature was 37 ºC, pulse 100 per minute, and blood pressure 117/66 mmHg. The abdomen was soft with supra-pubic tenderness. His white blood cell count was 4.7 x109/L. Serum electrolytes and blood sugar was normal. Chest X-ray has shown air under diaphragm. Laparotomy has revealed a 1cm perforation of the terminal ileum 60 cm from ileocaecal junction with pyogenic membrane covering the small intestine. Resection of a 15 cm segment of the small bowel was done with end to end anastomosis. Post operatively the patient was intubated and ventilated in the ICU and covered with broad spectrum antibiotics. He developed multiple organ failure and died on the 9th postoperative day. Histopathological examination showed ulceration and perforation of the small intestine due to Cytomegalo Virus infection (Fig 2). Serological test confirmed HIV infection. Case Four A 22-year old man presented with a one-day history of colicky lower abdominal pain associated with nausea. On examination, the patient was dehydrated. His temperature was 37.3 ºC, pulse 104 per minute and blood pressure 105/85 mmHg. Abdominal examination revealed severe lower abdominal tenderness and guarding. His white blood cell count was 16.4 ´109/L. Serum electrolytes and blood sugar was normal. Chest X-ray has shown air under diaphragm. Laparotomy has shown a small perforation of 2 mm diameter in the ileum, 40 cm proximal to iliocecal junction. The ulcer edges were excised and the defect closed in two layers. The patient was discharged home on the 9th postoperative day in a good condition. The histopathological examination has shown sheets of chronic inflammatory cells with many scattered poorly formed granulomas. However, no caseous necrosis could be seen and special stains failed to reveal any organisms. The lymph node sections showed few granulomas. The differential diagnosis included tuberculosis and Crohn's disease. A detailed small bowel diagnostic workup, small bowel enema and colonoscopy with terminal ileum biopsy, to reach a definite diagnosis was planned but the patient was lost to follow up. Discussion Different pathologies may lead to perforation of the small intestine. Infection is the commonest cause of such perforations in developing countries. This includes typhoid fever and tuberculosis 1, 3, 5, 6, 7. Nevertheless, in industrial countries, non-infectious etiology such as Crohn's disease and malignancy is predominant. Rare cases of non-traumatic perforation of small intestine due to opportunistic infections were also reported 1, 5. The clinical presentation in non-traumatic perforation of small intestine is non specific 1, 5. The abdominal examination of three of our patients has revealed moderate localized or generalized tenderness but relatively soft abdomen. The diagnosis is mainly clinical, supported by radiological finding of free gas under diaphragm 2, 5, 8. In one of our patients, chest X-ray, ultrasound and CT scan were all normal. Laboratory investigations were not helpful in all cases (2, 8, 9). Leukocytosis was present only in one patient. In a series of 79 patients, Wani et al have found that only 29% of patients with non traumatic perforation of terminal ileum have leucocytosis. Furthermore, no single investigation had a high diagnostic accuracy5. Intestinal perforation is associated with high mortality if early and proper management is not initiated 5, 8, 10. Preoperative resuscitation and intravenous antibiotic are important (8, 11). Furthermore, the general condition of the patient, the number of perforations, the condition of the intestine, and surgeon's experience define the operative procedure, prognosis and outcome 6, 11, 12. Single ileal perforation was seen in all cases and non-perforated ulcers were found in two patients. Single perforation can be treated by excision and simple closure 5, 11, 13. Resection anastomosis was the choice in the HIV patient due to the multiplicity of ulcers 9. The Histopathological examination of the small bowel ulcer were non conclusive in three patients. We have made our management plan according to the clinical findings. Histopathological examination of the first patient was non specific. The travel history to an endemic area with typhoid, the history of intermittent fever for one month, and the age of the patient made the clinical diagnosis of typhoid fever more probable 5, 8. We have stopped performing Widal test because of its limited value 2. In a series of 82 cases of proven typhoid ileal perforation, Atamanalp et al have found that histopathological findings were non specific in mild cases6. This is similar to case one in our study. In another study of terminal ileal non traumatic perforations, Wani et al have found that in almost one quarter of the patients the cause of perforation could not be known and typhoid was diagnosed clinically similar to case one in our study 5. The intraoperative findings have mimicked typhoid without laboratory confirmation of the disease 5. The histopathological picture in the second patient was a tiny pinhole non-specific inflammation possibly caused by the hook worms. We have found only one reported case of perforated jejunum by hookworms 14 It is difficult to know whether this is a coincidence or a cause. Wani et al have found ascariasis in the peritoneal cavity of 14 out of 79 patients of non traumatic bowel perforation and they thought that this was a sequence and not the cause 5. CMV infection was the cause of ulceration and perforation of the third patient. Although, HIV infection is uncommon in our community because all residents are screened for HIV, CMV infection is known to be the most common cause of intestinal perforation in AIDS patients 15. Although abdominal pain is a common symptom in AIDS patients, they rarely develop intestinal perforation. Only 5% of HIV patients present with abdominal pain that requires laparotomy 15. The morbidity after laparotomy in those patients reaches up to 50 % 15, 16. Presence of granulomas in the histopathological examination in the fourth patient was suggestive of a granulomatous inflammation with a differential diagnosis of tuberculosis or Crohn's disease 17. Tuberculosis is more common in our area. Furthermore, it is the second commonest cause of small bowel perforation after typhoid which is usually has a single perforation 3. If the diagnosis is not definite, we assume that it is tuberculosis and treat it accordingly. Otherwise, if prednisolone is started the result can be catastrophic leading to disseminated tuberculosis. The patient was planned for workup, small bowel enema and colonoscopy with terminal ileum biopsy, but he was lost to follow up. Low income and fear of the cost of medical treatment is a common cause of lost follow up of low socioeconomic patients in our community. In summary our study has shown that the diagnosis of non traumatic perforation is a challenge. Clinical findings are usually non specific and definite diagnosis is usually reached after surgery. Although intraoperative biopsy around the perforation is an important factor for proper management, histopathological examinations are not always informative. Non traumatic perforation in developing countries can be due to typhoid, HIV, tuberculosis and possibly hook worms. References:
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08008f1.jpg] [hs08008f2.jpg] |
| |||||||||

{kind=link}
{kind=link}