 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 1, March, 2008, pp. 44-49 Risk factors for placenta praevia presenting with severe vaginal bleeding in Mulago hospital, Kampala, Uganda Paul Kiondo1, Julius Wandabwa2, Pat Doyle3 1) Makerere medical school, P.O. Box 7072, Kampala, 2) Walter Sisulu University, Private Bag XI Unitra, Mthatha 5117,
South African 3) London School of Hygiene and Tropical medicine, London Keppel Street WC1E 7HT Code Number: hs08010 Abstract Objective: To determine the risk factors for placenta praevia presenting with severe vaginal bleeding in Mulago hospital,
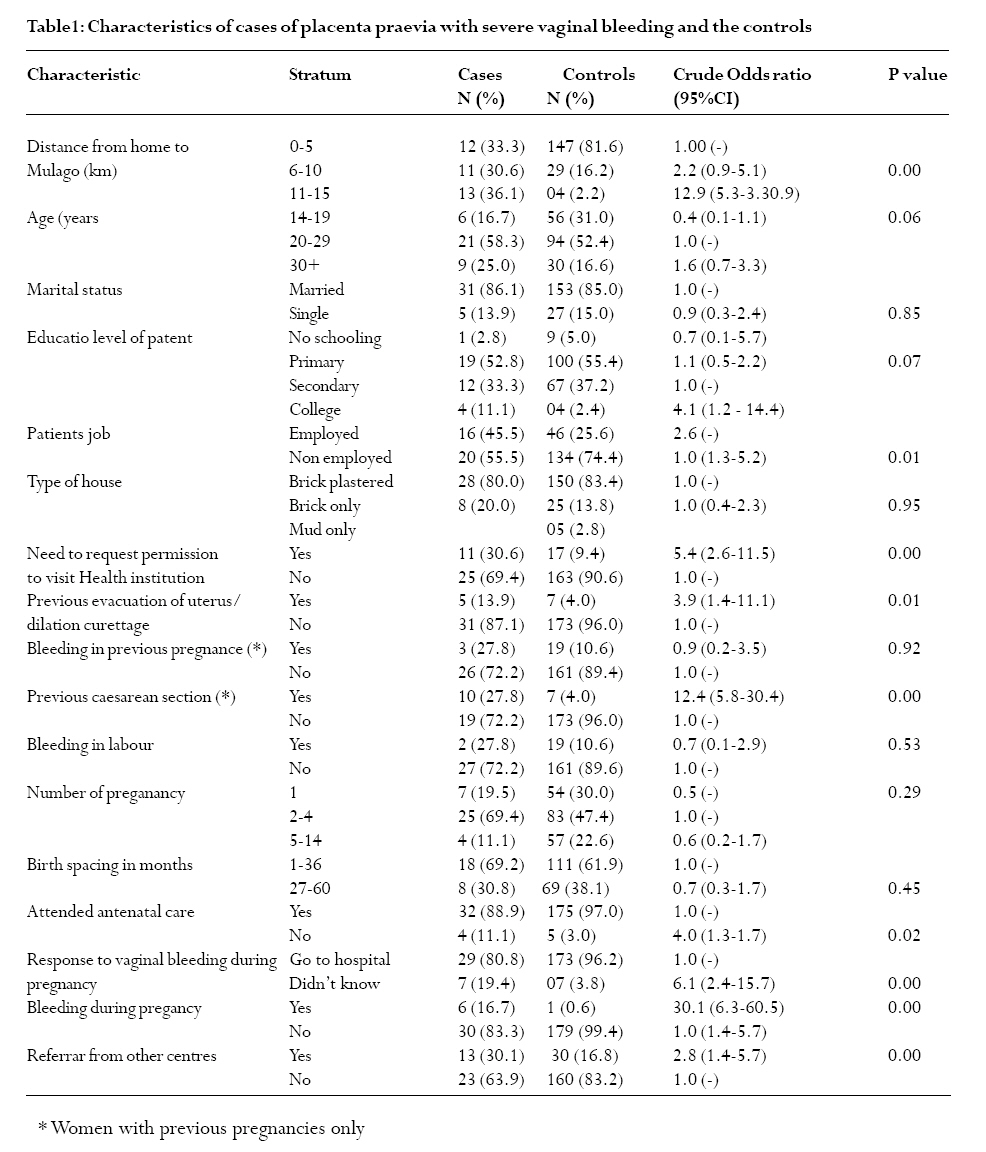
Kampala, Uganda. Introduction Placenta praevia is the implantation of the placenta partly or entirely in the lower segment of the uterus. It is classified as minor or major placenta praevia1. Major placenta praevia is when placental edge touches or covers internal cervical os. Mothers with placenta praevia present with painless vaginal bleeding after twenty four weeks but before delivery of baby2. The bleeding is usually mild and recurrent but sometimes can be massive and life threatening. The incidence of placenta praevia is 3-5 per 1000 pregnancies world wide and is still rising because of increasing caesarean section rates. The incidence is much higher at twenty weeks than at 36 weeks and above. This is because as pregnancy advances the lower uterine segment is formed, the upper segment enlarges and moves with the placenta.1-5. The independent risk factor for placenta praevia is a previous delivery by caesarean section. The risk increases with the number of caesarean sections performed. The incidence is 2% after one previous caesarean section, 4.1% after two and 22% after three.1. Similarly dilation and curettage, evacuation of uterus and myomectomy are associated with placenta praevia. Placenta praevia is more common in older and multiparous women.5,6,7. The reason is not clear but it may be associated with the ageing of vasculature of the uterus. This causes placental hypertrophy and enlargement which increases the likelihood of the placenta encroaching on lower segment.6 Birth spacing is associated with a risk of placenta praevia. In a study carried out among Norwegian women, it was found that birth spacing of more than four years was associated with placenta praevia. This could be due to scarring or poor vasculature of the uterus which is associated with increasing age.6 Placenta previa is associated with male births6,8,9. The reason for this is not known but it could be linked to maternal hormones or prematurity. Premature rupture of membranes occurs more commonly in pregnant women with male babies and placenta praevia is also more common in premature pregnancies2. Mothers with placenta praevia have a ten fold risk of reoccurrence in a subsequent pregnancy. This is thought to be linked to defective decidual vascularisation.6,8 . Placenta abruptio is associated with placenta praevia. In Norway women who had abruptio placenta had two fold risk of having placenta praevia as well. Abnormal placentation and smoking have been attributed to abruptio placenta and placenta praevia6. Multiple pregnancies are associated with placenta praevia. This is because the large placenta usually encroaches on lower segment of the uterus. But one study did not find this association4. Severe bleeding in placenta praevia is associated with severe maternal morbidity and sometimes mortality. This is especially so in developing countries where few women attend antenatal care, there is shortage of blood for transfusion and delays of operative delivery due to logistical problems. The risk factors for severe bleeding in parturients with placenta previa are not well documented. The major objective of this study therefore was to determine the risk factors for parturients with placenta praevia who presented with severe vaginal bleeding so as to reduce the maternal morbidity and mortality associated with this condition. Methods Study design: This was part of a case-control study for risk factors for severe maternal morbidity conducted in Mulago hospital, Uganda between 15th November 2001 and 30 th November 2002. The main results of the case control study will reported elsewhere. The risk factors of severe bleeding in parturients with placenta previa were studied. Setting: Mulago hospital labour suite where mothers with complications in pregnancy are referred for delivery. Mulago Hospital is a National Referral Hospital for Uganda and a Teaching Hospital for Makerere University, Faculty of Medicine. It also serves as a District Hospital for Kampala district. Mothers with complications in Kampala are referred here. Study population: Women who were admitted in Mulago hospital labour suite. Selection of cases and controls Both cases and controls lived 15 kilometres or less from Mulago Hospital and consented to the study. In this study severe bleeding in placenta praevia was defined as painless vaginal bleeding in pregnancy after 24 weeks gestation in which the mother developed an episode of shock with a systolic blood pressure of 90mmHg or less, a pulse rate of 100 beats/minute or more with a small volume, a need for an intravenous therapy of two or more units of blood, and an intravenous therapy of fluids of two or more litres. The cases were selected consecutively until the sample size was attained. Controls were selected from women who had a normal delivery at Mulago Hospital during the study period. They must have not had an episiotomy or tear of more than first degree and had normal blood loss .They were recruited using computer generated numbers, where five women were selected for every case. The cases and controls were followed up till discharge or death. The mothers were interviewed about their (exposure variables) socio demographic characteristics, social and family history, gynaecological operations, blood transfusion, medical conditions, past and present obstetric performance. Those who were too sick their spouses or first relatives were interviewed and later when the patients improved were interviewed at discharge. At discharge or death the clinical record files were reviewed and information on management was extracted. All the mothers were counselled before their blood was withdrawn for HIV screening. The screening was done using Determine test (Abbott Laboratories, Abbott Park, IL). This was an immunochromatographic test for qualitative detection of HIV-1/2. The test was performed by applying 50ul of serum to the test pad at the bottom of the strip. Analysis The data collected were checked, coded and double entered using Epi-Info 6.04 software package. The data were cleaned and transferred to stata 8. Univariate analysis The numbers and percentages of cases and controls at each level of exposure are presented. Chi square test was used to compare the proportions. Logistic regression Logistic regression was used to establish the strength of association between exposure variables and severe bleeding in placentae previa. Logistic regression uses the log odds ratio and all associations are presented as odds ratios with corresponding 95% confidence intervals. Odds ratio greater than one represents an increased risk of severe bleeding in placentae previa in that exposure category compared to the baseline category. Several factors that were influential in the study were put in a model. The logistic regression model first included exposure variables from socio demographic, family and social characteristics. Those that were statistically significant were included in the next model which included gynaecological and past obstetric performance and those significant were included in final model with present obstetric performance and HIV status. Age was included in the model because it is a known risk factor. All factors that had a p value of less than 0.1 in the socio demographics, social, family, and medical history were selected together with age and put in one logistic regression model and adjusted. Then significant factors with p value of 0.05 or less from this model were adjusted against past obstetric outcome, and then adjusted against current obstetric outcome and the laboratory results. Results There were 22456 deliveries during the study period and 36 patients presented with placenta praevia with severe vaginal bleeding contributing 0.16% of total deliveries. The thirty six cases were compared to one hundred and eighty normal deliveries. Eighty percent of the cases were major placenta praevia. All the minor placenta praevia were of type two. The cases and controls were similar in their socio demographic characteristics as shown in Table 1. The majority of mothers were below the age of thirty years and the rate of HIV infection was similar in both groups. It was s 8% in the cases and 9% in the controls. However most cases lived more than five kilometres from the hospital when compared to controls (P< 0.001). The cases were more likely were more likely to ask for permission to visit a health institution (p=0.001), were more likely to have had an evacuation in a previous pregnancy (p=0.01) and more likely to have delivered by caesarean section in the previous pregnancy (p=0.001) compared to controls. The cases were less likely to attend antenatal care (p=0.02) and were more likely to have been referred to hospital (p=0.001) when compared to controls. The cases were less likely to know what to do after an episode of vaginal bleeding (p=0.001), and they were more likely to bleed during the current pregnancy (p=0.001) compared to controls. These were distance from Mulago hospital ( OR 21.4, CI 7.4-63.4), request for permission to seek health care (OR 3.2, CI: 1.3-5.2), previous history of an evacuation of the uterus (OR3.6, 95% CI 1.1 to 12.5), delivery by caesarean section in their previous pregnancy (OR 19.9, CI 6.4 to 61.7) , poor response to vaginal bleeding(OR 7.3, CI 2.4-22.0) and bleeding in the present pregnancy before labour(OR 9.9, CI 1.3- 77.8) were associated with an increased risk of having placenta praevia. Discussion Placenta praevia is a major cause of obstetric haemorrhage in the third trimester. It is associated with severe maternal complications and adverse perinatal outcomes. The majority (75%) of patients had major placenta praevia. Five of the cases of placenta praevia type two were also placenta accreta. The further the patients lived away from Mulago hospital and asking for permission before attending a health unit or a hospital were associated with increased risk of developing severe ante partum haemorrhage due to placenta praevia. This condition is life threatening and occurs within a short time and if patients have to ask for permission to attend a health unit, then it increases the risk of the risk of severe vaginal bleeding and hence maternal morbidity and mortality. The patients who were referred were associated with thrice the risk for developing severe haemorrhage due to placenta praevia. Referral may have been associated with delay for patients to arrive in Mulago hospital because of lack of ambulance services in most health units. The majority (75%) of both cases and controls in the study were below the age of 30 years. Age and parity were not found to be risk factors in this study, although many studies have reported an association of placenta praevia with increasing age and high parity5,10,11. The patho-physiology of placenta praevia in multiparity is similar to that of age which is thought to be due to atherosclerotic changes in the uterus and infarction which cause under perfusion of the placenta. This leads to an increase in the size of the placenta. It causes mainly minor placenta praevia and most of these cases were not included in the study unless they presented with severe haemorrhage. The patients who were employed were associated with twice the risk of placenta praevia with severe vaginal bleeding. Women who are employed spend less time resting. This may predispose them to haemorrhage since bed rest is one way of managing placenta praevia. However no study has ever reported an association of socio economic factors as a risk factor for placenta praevia. It is possible that the working women could have had an evacuation or dilation and curettage resulting into placenta praevia. A history of evacuation and or dilation and curettage of the uterus were associated four times with the risk of placenta praevia. This was similar to other studies5,10,12. Evacuation was related with a history of abortion but abortion was a not a risk factor in this study. Evacuation is associated with scarring of the uterus. This leads to under perfusion of the uterus and predisposes women to placenta praevia. Scarring of the uterus is also associated with placenta accreta5,11,13,14. Patients who had previous delivery by caesarean section were associated with an increased risk of placenta praevia. Most studies have reported an association between previous caesarean section and placenta praevia.5,10,12,15. In a Meta analysis of 170,640 pregnant women, a dose related response pattern of risk factors for placenta praevia was found with increasing number of caesarean section deliveries. The odds ratios ranged from (4.5, 95%CI 3.6 to 5.5) for one caesarean section delivery to (44.9, 95%CI 13.5 to 149.5) for four or more caesarean section deliveries.14. The reason is the damage and scarring of the uterus during caesarean section. This predisposes to low implantation of the placenta. However the damage during lower segment caesarean section is not much and may not be the only explanation. The other explanation is the attraction and adherence of the placenta to the caesarean section scar 14,15,16,17,18. The scarring of the uterus may also retard the physiological development of the lower uterine segment. These interfere with the placental migration with the upper segment as the pregnancies grow. The history of evacuation of the uterus may act in the same way as previous scar on the uterus.10,14. Recently manual removal of placenta has been reported to be a risk factor for placenta praevia. This also acts through scarring of uterus5. When women were asked what they would do when bleeding starts during pregnancy, those who didn't know were at an increased risk of seven times of developing placenta praevia with severe vaginal bleeding after adjusting for confounders. Bleeding in the present pregnancy was associated with an increased risk of severe vaginal bleeding due to placenta praevia. This was likely to be due threatened abortion or early presentation of placenta praevia. Vaginal bleeding due to placenta praevia is likely to occur when the lower segment of the uterus begins to form from thirty two weeks of pregnancy. Eleven percent of cases compared to 3% of controls didn't attend antenatal care. After adjusting for confounders the effect of lack of antenatal care on the risk of getting severe placenta praevia disappeared. Antenatal care would be effective if there was a routine ultrasound examination on all women who attended or have had vaginal bleeding. This will identify cases with placenta praevia and their management planned. The cost and maintenance of ultra sound machines may be enormous for developing countries for it to be routine. Women with placenta praevia were nineteen times more likely to deliver low birth weight babies. This is because of severity of bleeding leads to premature delivery. Chronic hypoxia due to placenta praevia also causes intra uterine growth retardation. This leads to delivery of low birth weight babies. Similar findings have been reported by Svien.11. HIV infection was not a risk factor for placenta praevia. The limitations of this study were small numbers which can be explained by the low prevalence of placenta praevia. There was also a selection bias as Mulago Hospital is a National Referral Hospital and many women with previous and/or current pregnancy complications are referred here. However the results have similar trends to already published results. Conclusion Severe bleeding in placenta praevia is associated with high maternal morbidity. The determinants of severe bleeding in placenta praevia can be used in the antenatal period to identify mothers at risk. These with prompt intervention to deliver the women can reduce the maternal morbidity associated with this condition. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08010t2.jpg] [hs08010t1.jpg] |
| |||||||||

{kind=link}