 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
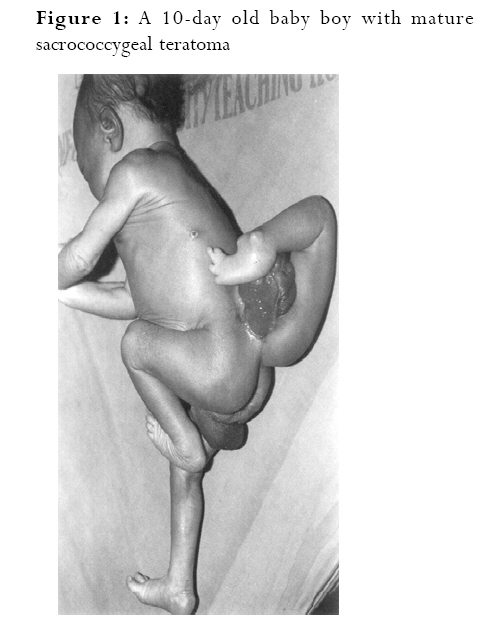
African Health Sciences, Vol. 8, No. 1, March, 2008, pp. 54-57 Case Report Mature sacrococcygeal teratoma: case report J.N. Legbo, W. Ek. Opara, J.F. Legbo Department of Surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria. Telephone: +234 (0) 8035868790, E-Mail: legboj@yahoo.co.uk Code Number: hs08012 Abstract Background: Mature sacrococcygeal teratomas (SCT) are uncommon neoplasms comprised of mixed elements derived from the
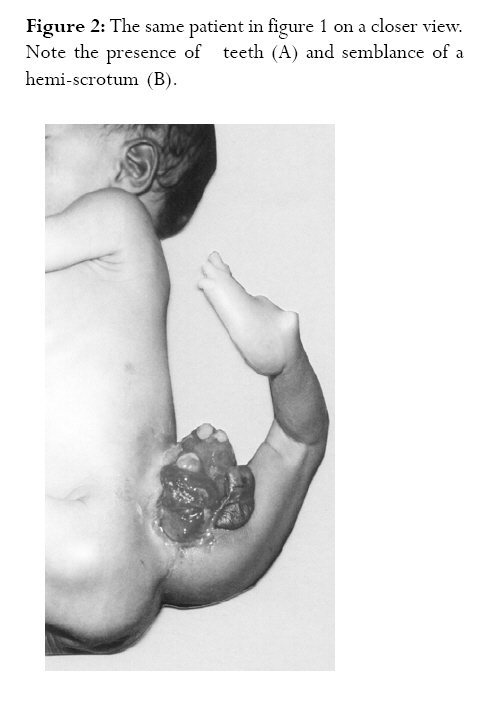
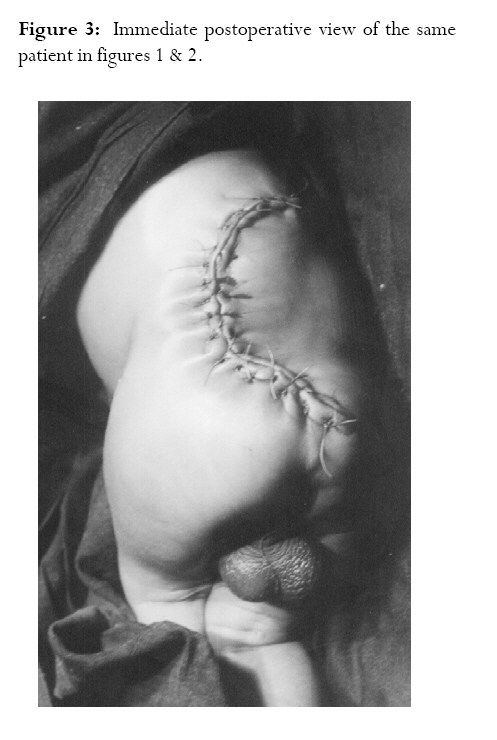
three germ cell layers. They attract attention because of their gross appearance and bizarre histology. Keywords: Sacrococcygeal teratoma, excision. Introduction Sacrococcygeal teratoma (SCT) is a well-known tumour of the newborn which carries an excellent prognosis provided adequate surgical treatment is prompt and excision complete 1. Although generally a rare condition, it is said to be the most common tumour in the newborn period, with a reported incidence of approximately one in 35,000 -40,000 live births 1-3. It is a more common tumour in females 4, with a male: female ratio of about 1: 3-4 4,5. There are many conflicting theories as to the origin of SCT 3. Historically, teratomas were attributed to demons, sexual misconduct and abnormal fertilization 6. They are composed of two or three germ cell layers; have multiple tissue types, and can present in various sizes and shapes 6,7. Believed to have arisen from the totipotent somatic cells that originate from the primitive knot (Hensen's node), they are usually attached to the coccyx 7,8. In contrast to the newborn with SCT, the fetus with SCT remains at high risk of perinatal complications and death 9. Fetuses with SCT detected antenatally have three times mortality rate compared with postnatally diagnosed neonates 10. Neonatal death may result from maternal obstetric complications of tumour rupture, preterm labour, or dystocia 9,11 . The fetus is also at risk of high output cardiac failure, placentomegally and hydrops with subsequent fetal demise secondary to the metabolic demands and vascular steal of a rapidly growing solid tumour 7,9. Modern technology using the three-dimensional (3D) sonography now allows prenatal diagnosis of SCT even in the first trimester 12. Surgical resection remains the mainstay of therapy, and recurrence is rare following complete excision. Only a few cases of SCT with a complete limb have been reported worldwide 7,13. This case is reported to highlight the clinical presentation and management of SCT in a neonate. Case report A 10-day old baby boy was presented to us by his parents with a third leg at the lower back since birth. He had otherwise been apparently well since birth. He was delivered at home by traditional birth attendants (TBA) after a term, unsupervised pregnancy to a 32-year old para 7 woman. Both pregnancy and delivery were uneventful. Both parents looked anxious and quite worried. On clinical examination, the baby was an active, healthy-looking neonate with a mass attached to the sacrococcygeal region. The mass consisted of a fully developed lower limb attached to the sacrococcygeal region (figure 1). The limb had four toes on the foot, subluxation of the ankle joint and good range of movement over its attachment to the sacrococcygeal region. On the medial aspect of the extra limb was a bag of skin like an empty scrotal sac (figure 2 -B); more medially was a roll of three teeth on a pinkish, soft tissue (figure 2 -A). The cardiorespiratory and abdominal examinations were not contributory. The occipito-frontal circumference was 36.2cm. Digital rectal examination revealed normal anal sphincteric tone, with no evidence of intrapelvic extension of the sacrococcygeal mass. The relevant haematological and biochemical investigations were all within normal limits. A plain radiograph of the lumbosacral region revealed a clear demarcation between the limb and the spine. The alpha-fetoprotein done in an outside laboratory was normal, but CT Scan was not possible due to financial constraints. After an informed consent, surgical excision (including coccygectomy) was accomplished via a right lateral flap based on the junction between the extra limb and the back of the patient. The flap was then flipped over to cover the defect medially and to the left (figure 3). Histological examination of the excised tissue was consistent with mature SCT (with no evidence of malignancy). The baby had an uneventful postoperative recovery and was discharged home on the 9th postoperative day. Follow-up at three years revealed that the child had normal developmental milestones, a well-healed scar that was barely visible, and no clinical or biochemical evidence of recurrence. Discussion The newborn with sacrococcygeal teratoma (SCT) has an excellent prognosis depending on the timing of diagnosis, malignant potential of the tumour and the ease of surgical resection 4. Although prenatal diagnosis is possible in some cases, this was not possible in our patient since the mother did not attend antenatal care. SCT could be diagnosed from the second trimester of pregnancy when there is polyhydramnious and/or a uterus larger than the gestational age 14,15. Prenatal diagnosis is of significance since early prenatal presentation is associated with high fetal morbidity/mortality, while presentation after 30 weeks gestation is a relatively good prognostic indicator for fetal survival 15,16. In addition, such early diagnosis may predicate delivery by caesarian section in centers with good neonatal facilities where early surgical treatment can be offered to the baby. Similarly, fetal surgical interventional procedures could be undertaken when the diagnosis is made early in pregnancy 9,16-19. Since our patient's mother had no antenatal care, and delivery was not supervised by trained personnel, the chances of both maternal and child mortalities from obstetric complications were high. Because of the disposition of the tumour, this particular case could have led to dystocia, prolonged labour and damage to maternal birth canal. The case presented here is a male. Although about 75% of cases are seen in females, the exact reason for female preponderance is not fully understood 4,5. As in most congenital abnormalities, the parents were psychologically disturbed, since the baby could not be shown to relations, or taken along for social events. This appears to have prompted them to present in hospital for treatment. It is however gratifying that the parents did not think about terminating the life of the child, because such babies have been victims of infanticide 6,7. A well-planned surgical excision was undertaken in our patient, including preoperative skin markings to enable flap reconstruction of the defect (figure 3). Care was also taken to ensure inclusion of the coccyx in the excision material in order to forestall possible recurrence. Apart from age at diagnosis and treatment, and the extent of resection, the prognosis is also determined by the histologic type and stage at the time of resection, and not the size of the tumour 4. Complete excision (including coccygectomy) as in our own case, is the primary therapy for all SCT and it is adequate if the tumour is benign. Chemotherapy and radiotherapy are however indicated in malignant cases 14. Where the tumour is adjudged malignant, a recurrence as high as 37% has been reported if the coccyx is not removed in the primary surgery 20,21. Follow-up in patients with SCT is necessary especially during the first three years of treatment when recurrence is more likely 22. Extensive surgery in the pelvic and perineal region may involve disruption of nerves and muscles which supply the urinary/ano-rectal sphincters and provide maximum support in normal working respectively. In the 3-year period of follow-up of our patient, he has maintained good urinary and ano-rectal function, with no clinical, biochemical or radiological evidence of recurrence. Longer period of follow-up is however required, in order to make our claim more authentic. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08012f1.jpg] [hs08012f3.jpg] [hs08012f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}