 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 67-73 Non-adherence to diabetes treatment at Mulago Hospital in Uganda: prevalence and associated factors Joan N Kalyango1,2, Erisa Owino 1, Agatha P Nambuya 3 1Makerere University Medical School, Department of Pharmacy, 2Makerere University Medical School,
Clinical Epidemiology Unit, 3Mulago Hospital, Department of Medicine, Uganda Code Number: hs08017 Abstract Background: Non-adherence to diabetes treatment leads to poor glucose control and increases the risk of disease complications.
The prevalence and factors associated with non-adherence in resource limited settings should be determined so as to lower the impact
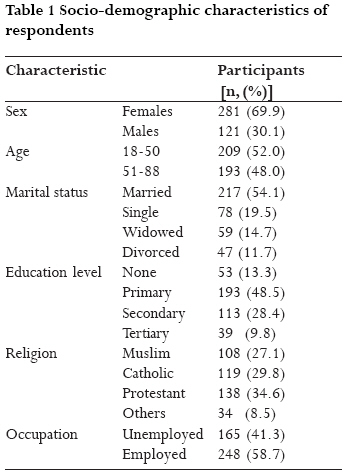
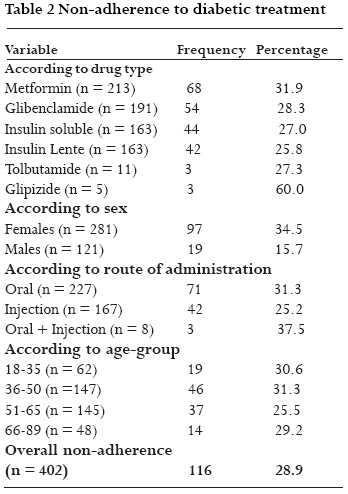
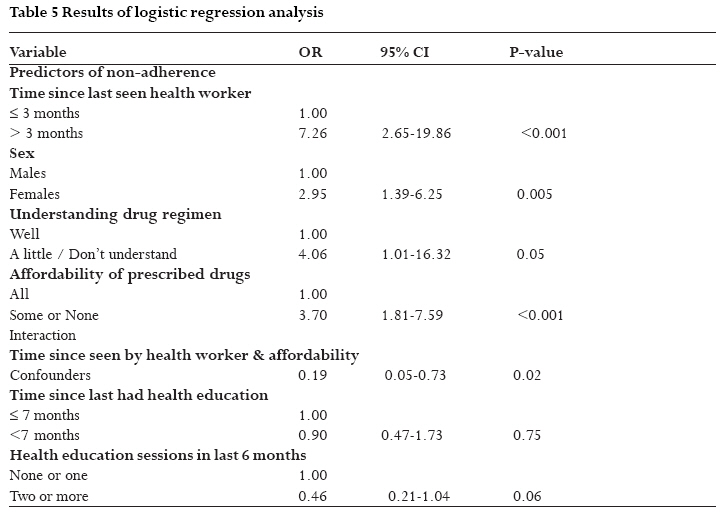
of a disease that is on the increase, on the health systems which are already overburdened with communicable diseases. Introduction Non-adherence to prescribed drugs schedule has been and continues to be a major problem the world over. Studies on this subject show that adherence is about 50% for medications in chronic diseases and much lower for lifestyle prescriptions (1, 2). Diabetes is considered to be one of the most psychologically and behaviorally demanding of the chronic diseases (3). It requires frequent self monitoring of blood glucose, dietary modifications, exercise, and administration of medication on schedule (3-5). Studies have emphasized the importance of achieving optimal glucose control through strict adherence to medications, diet, and exercise in order to minimize serious long term complications (2, 3, 6). These complications affect the patient's quality of life, increase mortality, morbidity and economic cost to society (2, 3, 7). It is imperative that patients adhere to their prescribed regimens to minimize the burden of the disease on the health systems (2, 7). Non-adherence in chronic diseases has been described as taking less than 80% of the prescribed treatment (1). Previous studies have found adherence to diabetes treatment generally to be sub-optimal ranging from 23 to 77% (2, 8-11). In addition, these studies have generated varied results of the factors associated with non-adherence to diabetes treatment. A number of health service and medicines related factors that have been cited in the literature include: poor patient provider relationship, longer time since diabetes education, side effects of the medication and pill burden (3, 9, 12, 13). The sample sizes used in some of the studies have been very small and the method of selection of participants in some cases has led to highly selective samples that are not representative of the populations from which they are picked. Furthermore, most of the studies were carried out in developed countries, leaving a gap in knowledge about the prevalence and factors that may be associated with non-adherence to diabetic treatment in Uganda, a developing country. This study was therefore carried out among a sample of 402 diabetic patients to determine the prevalence and factors that are associated with non-adherence to diabetes treatment. Methods This was a cross sectional study with quantitative methods of data collection. The study was approved by Makerere University Faculty of Medicine Research and Ethics Committee. Patients Patients for this study were obtained from Mulago hospital, a national referral and teaching hospital in Uganda. The hospital is located within Kampala City, in the Central region of Uganda. It operates an out-patients diabetic clinic once a week and has in-patient facilities where medical care is provided throughout the week. The patients receive free medical care including medicines when available in the hospital. A total of 402 diabetic patients were sampled from the out-patients diabetic clinic from February to April 2004 using systematic sampling. The first patient was selected on each clinic day by writing down the names of the first two patients each on a separate piece of paper and randomly selecting one. Thereafter, every other patient that met the selection criteria was selected. The sample included both Type 1 and Type 2 diabetic patients. Inclusion criteria: The main inclusion criteria were: having diabetes, aged at least 18 years, attending the diabetic clinic during the study period and giving written informed consent to participate in the study. Exclusion criteria: Patients who were very ill and those newly diagnosed with diabetes (less than one month) were excluded from the study. Using these criteria, 7 patients were excluded because they were very ill and 32 patients because they were newly diagnosed with diabetes. Only one patient was approached and refused to participate in the study. Data collection Trained interviewers used a pre-tested semi structured questionnaire to obtain information on patients' demographic characteristics and some risk factors to non-adherence to diabetes treatment. These included: health education attendance, number of prescribed drugs, route of drug administration, patients' self rating of how well they understood their drug regimens, adverse drug reactions, patients' affordability of the prescribed drugs, duration of diabetes and use of alternative medicines. The patients' health cards were used to ascertain their medication regimens. Non-adherence was assessed using patients self reports of how they had been taking their medication in the week preceding the interview. Patients were asked to recall if they missed any doses of medication on a day by day basis over a period of one week. The number of tablets missed was calculated basing on the prescribed dose. Patients who reported taking less than 80% of their prescribed diabetes medicines were considered not to be adhering to treatment. In statistical analysis, descriptive statistics were used for general description of study participants and to obtain the prevalence of non-adherence to diabetes treatment. Bivariate analysis was then performed between the various independent variables and non-adherence to diabetes treatment. Odds ratios, their 95% confidence intervals and p-values were obtained. Independent variables whose p-values did not exceed 0.2 were selected for the multivariate analysis in order to determine which variables were independently associated with non-adherence. Logistic regression was used for multivariate analysis. STATA 8.0 statistical software (Stata, College Station, TX, USA) was used for analysis. Results The average age of the participants was 50 years (standard deviation =13.8) and more than half of them were females (69.9%). The majority of the participants were married (54.1%, n = 217) and about half of them (48.5%, n = 193) had primary education as the highest level of education attained. Only 58.8 % (n = 235) were employed. The median duration with diabetes was 4 years (range 1 month 38 years). Socio-demographic characteristics of the participants are summarized in Table 1. The overall prevalence of non-adherence among the respondents was 28.9% (n = 116, 95% CI = 24.5 33.3%). About one third of those taking Metformin (n = 68, 31.9%), 34.5% of the females (n = 97) and 31.3% of those taking oral hypoglycemics (n = 71) were not adhering to treatment. Almost one third of respondents in the age group 36 to 50 years were not adhering (n = 46, 31.3%). Results of non-adherence to diabetes treatment are summarized in Table 2. Factors found to be significantly associated with non-adherence on bivariate analysis were: sex (OR = 2.83, CI=1.62-4.95), education level (OR = 0.58,CI=0.36-0.92), patients self rating of how much of the prescribed drugs they or their caretakers could usually afford (OR = 1.91, CI=1.22-2.98), number of health education sessions attended in the previous six months (OR = 0.51, CI=0.27-0.95), duration of time since last health education session attended (OR = 1.73, CI=1.02-2.92), patients' self rating of how well they understood their drug regimens (2.61, CI=1.19-5.71) and time since last visit to a health worker (OR = 3.22, CI=1.85-5.59). Age, marital status, occupation of the respondent, duration of diabetes, route of drug administration, number of anti-diabetic drug types prescribed, use of alternative medicines and adverse drug events experienced by the patients were not significantly associated with non-adherence. However, only about 18% of respondents reported experiencing adverse drug event to anti-diabetic drugs and the majority of these reported Insulin (n = 36, 49.3%) as being the cause followed by Metformin (n = 20, 27.4%). Only 10.9% (n = 8) attributed the events to Glibenclamide and the rest were not sure of the cause. Having ever attended a health education session was also not significantly associated with non-adherence. The general health education sessions usually involve advice to patients about diet, physical activity, medication administration; self monitoring of urine and blood glucose and general self care for diabetic patients. They are usually conducted early in the mornings while patients wait to see the doctor. Results of bivariate analysis are summarized in tables 3 and 4. When the factors were fitted into a logistic regression model for multivariate analysis 64.9% (n = 261) of the respondents were retained in the analysis mainly because some had never attended health education (n = 88, 21.9%) and there was also some missing data on some of the variables fitted in the logistic model. Among the 141 participants that were missing from the logistic regression analysis 64.5% were females, 49.6% were in age group 51 to 89 years and 40.7% had attained secondary or tertiary education. These proportions are only slightly differing from those in the general sample (69.9%, 48% and 38.2% respectively). Generally there was no selective elimination of participants from logistic regression with regards to important demographic characteristics. Factors that were found independently associated with non-adherence after controlling for other factors were: female gender (OR = 2.95, CI=1.39-6.24), not understanding the drug regimen well (OR = 4.06, CI=1.01-16.32), patients or their caretakers being able to afford only some or none of the prescribed anti-diabetic drugs (OR = 3.70, CI=1.81-7.59), and longer time since last since last visit to a health worker (OR = 7.26, CI=2.65-19.86). Although time since last health education session attended and having attended two or more health education sessions in the six months prior to the study were not significantly associated with non-adherence, they were retained in the model because removing them from the model changed the odds ratios of the other variables (understanding drug regimen, time since last visit to health worker and how much of the prescribed drugs patients or their caretakers could usually afford) by more than 10% i.e. they were confounders. There was also statistical interaction between time since last visit to health worker and affordability of drugs. Stratified analysis showed that among the patients who rated themselves as able to afford all the prescribed drugs (n = 127), there was significant association between longer time since last visit to a health worker and non-adherence (OR = 6.88, p < 0.001). On the other hand among those able to afford only some or none of the drugs (n = 134), the association was not significant (OR = 1.37, p = 0.52). Likewise among those who had taken a shorter time since last visit to a health worker (n = 212), there was significant association between affordability of some or none of prescribed drugs and non-adherence (OR = 3.87, p < 0.001). Among those who had taken a longer time since last visit to health worker (n = 48), the association was not significant (OR = 0.69, p = 0.53). Results of logistic regression analysis are shown in table 5. Other factors that were fitted into the logistic regression model that were not retained were: education level attained, using alternative medicines and route of drug administration. Discussion More than one in every four respondents was not adhering to diabetes treatment. This level of non-adherence is quite high considering that cost of drugs which is one of the main barriers to adherence that has been quoted in the literature has been minimized by provision of free drugs to patients when they are available in the hospital. In addition, it is expected that the level of non-adherence found is an underestimate of the true prevalence of non-adherence in this population. This is because with self-reports that were used to assess non-adherence patients usually overestimate their adherence (1). Furthermore, patients may get problems recalling their medication taking practices but the errors arising from this were minimized by asking them to recall over a period of only one week. The prevalence of non-adherence to diabetes treatment found in the current study was lower than that of 75% found in the study done in India (11) which also used self-reports. This difference is possibly because the patients in the current study receive free medical care and drugs when they are available whereas in the other study patients had to pay for their treatment. Furthermore in that study, socio-economic status of the patients was associated with non-adherence implying that costs of treatment may have been an inhibitory factor in adherence. Therefore since the costs of treatment in the current study have been minimized, this lowers the risk of non-adherence. Other studies assessing non-adherence to diabetes treatment using other methods have found the prevalence ranging from 23 to 77% (2, 8-11). Non-adherence is likely to lead to increased complications of diabetes. These complications may increase the costs of health care because of increased morbidity and may also decrease productivity of the affected persons. The risk of non-adherence in this study was increased among patients who had taken a longer time since their last visit to a health worker and those who rated themselves or their caretakers as able to afford only some or none of the prescribed drugs. In addition, women had almost threefold increase in risk of non-adherence as compared to men and those who did not understand their drug regimens well had higher risk of non-adherence than those who understood them well. The relationship between some of these factors and non-adherence was modified by time since last health education session attended and number of health education sessions attended in the six months prior to the interview. The protective effect of shorter time since last visit to a health worker against non-adherence is probably due to the fact that apart from general health education sessions given in the clinic, the health workers give some health education talks to individual patients. It is likely that the health workers remind patients to take their medicine. However, it could also be that patients who take long to come to the clinic have certain characteristics that promote non-adherence, which also delay them from coming for review and possibly collecting drugs from the hospital since this is when they refill their diabetes medicines. Furthermore there is a possibility that the patients who have had a shorter time between visits to health workers perceive their illness as more severe and are therefore more likely to adhere to their treatment. In this study, adverse drug events were not significantly associated with non-adherence. The small proportion of respondents experiencing side effects could have been the reason why a significant association was not found. This finding is in contrast to findings in other studies in which patients who experienced side effects with anti-diabetic drugs were more likely not to adhere to treatment (9, 13). In one of these studies (9) the proportion of patients experiencing side effects was bigger than that found in the current study i.e. 26.5% as compared to 18% in the current study. There was no association between number of drug types taken, route of drug administration and non-adherence. This implies that these factors do not predict non-adherence among these respondents. This finding is similar to that found in other studies (13, 15). The relationship between sex and non-adherence could be due to a difference between males and females on another characteristic that was not assessed in this study. The result is similar to that found in another study among African Americans in which the men scored higher than women on self care adherence (16). The women in that study also scored higher on monitoring barriers than the men. Other studies have not found any association between sex and non-adherence (2, 5, 9). This could be due to the smaller number of participants (64 to 150 respondents) in these studies as compared to the current study (402). The proportions of the different sexes among participants are almost similar in all the studies done (ratio of about 1 male to two females) except in the one study (9) where 90.3% were females and 9.7% were males. The significance of the association between education level attained by the respondent and non-adherence seen at bivariate analysis diminished on multivariate analysis. The initial significant association of education with non-adherence could have been due to association of education to other variables that are associated with non-adherence which when controlled for are able to cater for possible confounding effect of this variable. The finding of a relationship between non-adherence and education on bivariate analysis is similar to that found in another study done in Mexico (2). However in that study, multivariate analysis was not done. Other socio-demographic factors like marital status, age, occupation, and religion were not significantly associated with non-adherence. These findings are consistent with other studies (2, 4, 15). However some studies (9) have found an association between age and non-adherence. The distribution of age in the two studies was also different. The mean age in the current study was 49.9 years (range 18 88) while in the other study (9) it was 56.4 (range 30-74). This could have been the reason why the results observed were different. Taking alternative medicines was not significantly associated with non-adherence although the patients not taking alternative medicines seemed to be at lower risk of non-adherence. The findings are similar to another study (2) where there was no significant association between using alternative medicines and non-adherence. Patients who could only afford some or none of the prescribed drugs could have been at a higher risk of non-adherence because of the failure to buy the drugs if they did not get them from the hospital. Some studies have found an association between socio-economic status and non-adherence (11). Although the patients get free drugs when they are available, sometimes they are not sufficient to cater for duration over which drugs have been prescribed. Patients who did not understand their drug regimens well were probably at higher risk of non-adherence because they had not understood how and when to take their drugs causing them to miss their drugs. Patients thus need to be told more about their drug regimens so that they can clearly understand them. Health workers need to determine which categories of people usually find problems with this aspect so that they can be specially assisted. Although health education attendance was not significantly associated with non-adherence, it was an important factor to control for as shown by the confounding effect of time since last health education session attended and number of health education sessions attended in the six months prior to the study on other independent factors in the multivariate model. It is possible that understanding the drug regimen is the important factor that enables patients to adhere and those patients who attend health education sessions are able to understand their regimens better. This is supported by the confounding relationship between understanding drug regimens and health education. Importance of health education has also been found in other studies (12, 14). There is need to design strategies to help patients understand their drug regimens in order to improve their adherence. This is to help prevent the complications of diabetes mellitus which are debilitating and if not prevented can increase the burden of a disease that is already on the increase. The time interval between visits to health workers should also be kept short and drugs should be availed at the health units so that patients who cannot afford to buy them can get them readily. Further studies are also needed to study the complexity of the relationship between time since last visit to a health worker, affordability of prescribed drugs and non-adherence. These studies should involve big numbers of respondents so that the numbers in the various strata can be sufficient. Acknowledgements We thank DAAD Scholarships Program for funding this study. We thank staff members of Mulago Hospital diabetic clinic that were involved in data collection and Dr. Charles Karamagi from Clinical Epidemiology Unit of Makerere University for advice on writing in this article. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08017t1.jpg] [hs08017t5.jpg] [hs08017t4.jpg] [hs08017t3.jpg] [hs08017t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}