 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 80-84 Factors associated with carcinoma of the oesophagus at Mulago Hospital, Uganda Ponsiano Ocama,1 Magid M Kagimu,1 Michael Odida,2 Henry Wabinga,2 Christopher K Opio,1 Britt Colebunders,3 Sabrina van Ierssel,3 Robert Colebunders3 1 Department of Medicine, Makerere University, 2 Department of Pathology, Makerere University, 3 University of Antwerp, Belgium Code Number: hs08019 Abstract Background: In Uganda, as in many other parts of the
world cancer of the oesophagus (CAE) is on the rise. Squamous cell
carcinoma and adenocarcinoma are the common subtypes. Risk factors for this cancer have been identified but not studied systematically
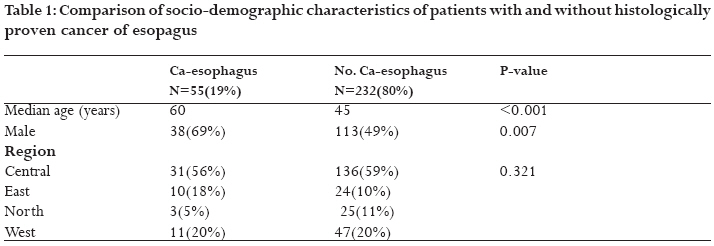
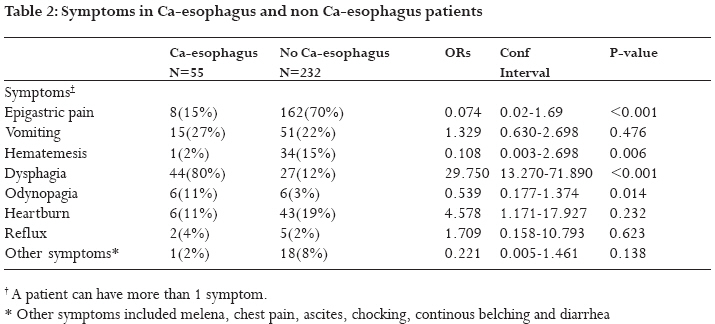
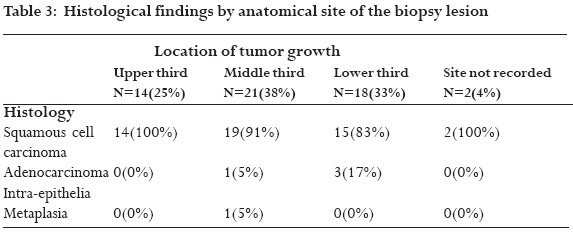
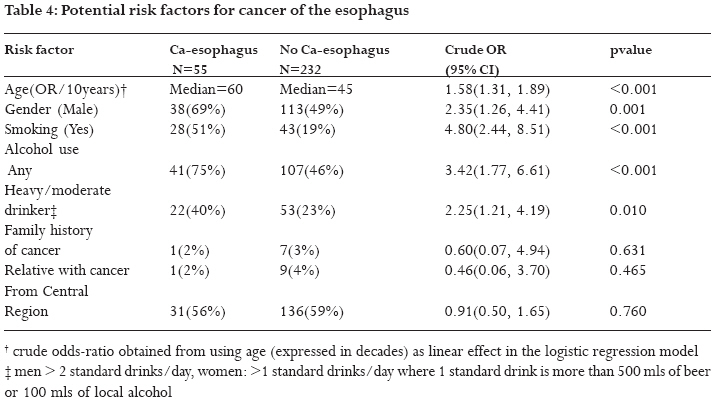
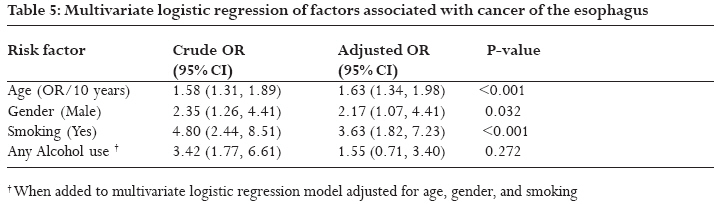
in Uganda. Identification of these factors would enable establishment of preventive measures. Background Cancer of the oesophagus (CAE) is generally on the increase worldwide1. Adenocarcinoma of the oesophagus is increasing at a faster rate now surpassing squamous cell carcinoma, reversing the trend that had been seen in the 1970s when the latter was the most common CAE. 1,2 In Uganda, the incidence of CAE is also on the rise. 3 Treatment of cancer of the oesophagus is problematic and mortality rates are very high with no cure in the majority of cases. Unlike in the West where treatment trials are on-going in Uganda, only palliative care can be offered and mortality is almost 100% within 6 months of diagnosis. CAE can occur at any site of the oesophagus, but its distribution has not been uniform for all the histological types. Cancers in the upper one-third of the oesophagus are mainly of the squamous type while those of the lower one third are generally adenocarcinoma; in the middle third of the oesophagus either adenocarcinoma or squamous cell carcinoma can be found. Squamous cell carcinoma of the oesophagus occur more often in patients with a long standing exposure to tobacco and alcohol4,5, achalasia6, tylosis7, lye ingestion 8 and celiac sprue.9 The etiological role of the Human Papilloma Virus in squamous cell carcinomas is still being investigated. 10-11 In Uganda, Human Papilloma Virus has been implicated in squamous cell carcinoma not only of the cervix but also of the conjunctiva. 12 Oesophageal adenocarcinoma has been associated with gastro-oesophageal reflux disease13-17 and a 0.5% annual risk of developing adenocarcinoma has been reported in patients with Barrett's esophagus. 18 Previous studies about CAE in Uganda were done based on data obtained from the cancer registry and all the tissues studied originated from one county in the country. 3 This is the first cross-sectional study reporting the prevalence and factors associated with CAE among patients referred to an esophageal-gastro-duodenoscopy (EGD) unit in a Ugandan hospital (Mulago hospital, the national referral hospital). Patients from various hospitals and clinics around the country are referred to this unit. Various risk factors for CAE have been identified but these factors have not been studied systematically in Uganda. Identification of these factors will enable establishment of preventive measures for this almost universally fatal cancer which has no effective treatment. Patients and Methods From September 2004 to September 2005 we performed a 1-year cross sectional study of all patients presenting for EGD at Mulago Hospital, Patients were enrolled after informed consent was obtained, if they were more then 18 years old, and if there were no contra-indications for EGD or biopsies. Data about patient demographics, reason for referral, possible risk factors for CAE, details of endoscopic findings, and histology of the CAE were collected. A CAE was defined when there was endoscopic evidence of tumour growth arising from the oesophagus with histological evidence of malignant cells on microscopy. EGD was performed using a Fujinon endoscope. Lidocaine 2% spray was applied to provide local anaesthesia. For patients with suspicious lesions, the anatomical site of the lesions was described and biopsies obtained with a forceps device passed through the working channel of the endoscope. Eight biopsy tissues of each lesion were taken, fixed in 10% formal saline solution, appropriately labelled, then dispatched for evaluation by the pathologist. In those patients in whom it was possible to pass the endoscope through the oesophageal stricture caused by the tumour, the mucosa of the stomach and duodenum were inspected and additional biopsies were taken if lesions were observed. . Biopsy tissues were embedded in paraffin wax before they were sliced by microtome to the appropriate size. The samples were then stained with haematoxylin and eosin. All biopsies were examined by any one of two senior pathologists of Makerere University. Data were entered into Microsoft excel spread sheets, coded and later exported to STATA 8® statistical package. The degree of association was determined by Mann-Whitney test for continuous variables and Fisher's exact test for categorical variables. Risk factors for CAE were identified by univariate logistic regression. Factors significant at the 5% level were selected in a multivariate logistic regression model to identify independently significant risk factors. Faculty Institutional review board authorization was obtained from Makerere University Faculty of Medicine before commencement of the study. Endoscopy was done as part of routine patient management and informed consent was sought from each study participant Results Two hundred nineteen patients were enrolled into the study. Three patients were excluded because they could not withstand the EGD procedure. Endoscopic diagnosis included: CAE 57 patients (20%), oesophagitis 11 patients (4%), oesophageal-varices 14 patients (5%), oesophageal ulcers 1 patient (<1%), candida oesophagitis 15 patients (5%), oesophageal stricture 7 patients (2%), cancer-stomach 11 patients (4%), gastritis 60 patients (21%), gastric ulcers 7 patients (2%), duodenal ulcers 16 patients (%) and duodenitis 13 patients (%). In 75 patients (26%) there were no abnormalities. Fifty five (19%) subjects had a histologically proven CAE, 92.5 % of them were squamous cell carcinomas (Table 1). The median age of those with a CAE was 60 years in contrast to those with no CAE, which was 45 years (p < 0.001). The majority of patients presenting with CAE were men (69%), compared to approximately half (49%) in non-CAE patients 49% (p = 0.007). Epigastric pain (70% vs. 15%) and haematemesis (15% vs. 2%) were reported more frequently by patients without CAE compared to those with CAE, (p<0.05) (Table 2). On the other hand dysphagia (80% vs. 12%) and odynophagia (11% vs. 3%) were reported more often in patients with CAE (p<0.05). In 49 out of 76 patients (64%) referred with a clinical diagnosis of CAE or oesophageal stricture and in 51 of 57 patients (89%) with an endoscopic diagnosis of CAE, a diagnosis of CAE was confirmed histologically.CAE were located 26% in the upper third, 40% in the middle third and 34% in the lower third of the oesophagus (Table 3). Squamous cell carcinoma was found in 100% of tumours of the upper third, 91% of tumours of the middle third, and 83% of tumours of the lower third. Four patients had a histological diagnosis of adenocarcinoma of the oesophagus; one patient had a histological diagnosis of intra-epithelia metaplasia. More subjects with CAE smoked in contrast to those without CAE (51% vs. 19%, p<0.001) (Table 4). Alcohol was consumed in 75% of subjects with CAE and in 46% of subjects without CAE (p=0.001). More CAE patients were moderate/heavy drinkers compared to the non-CAE patients (40% vs. 23%, p= 0.010). The use of spring/well drinking water was more often reported by patients with CAE compared to those without CAE (64% vs. 47%, p = 0.024), conversely use of tap drinking water was less often reported by patients with CAE compared to those without CAE (24% vs. 48%, p = 0.002). HIV serology was performed in only 37% of all of the study subjects; 19% of them were HIV seropositive. Mulitivariate logistic regression identified gender, age and smoking as significant independent predictors of CAE. Use of spring/well drinking water or alcohol use was no significant predictor of CAE when adjusted for age, gender and smoking habits (Table 5). DiscussionA high percentage (19%) of patients referred for endoscopy at Mulago hospital was found to have a CAE. In the majority of them, the CAE was a squamous cell carcinoma. A nearly equal number of squamous cell carcinoma was observed in all parts of the oesophagus but in the lower part, as expected, a few adenocarcinomas were also detected. In industrialized countries, a rise in adenocarcinoma of the oesophagus, surpassing squamous cell carcinoma, has been noticed. In Uganda the prevalence of squamous cell CAE has remained high compared to adenocarcinoma 19,20 Secondly, in contrast with a male to female ratio of squamous cell carcinoma of for example 5:1 in Ireland 21 in this study this ratio was 2:1, as was also previously reported in other studies from Uganda 19,20 , The reason for this difference is not clear but could be a result of smoking habits in the two populations. In nearly all patients referred with a clinical diagnosis of CAE this diagnosis was confirmed histologically. It has to be mentioned however that certain patients were referred for endoscopy based on the result of barium swallow.Smoking was associated with CAE. This is in congruence many other studies that have identified smoking as a risk factor for CAE, more so for squamous cell carcinoma than for adenocarcinoma. In our study, squamous cell carcinoma was the most common CAE. This concurs with a retrospective study carried out in western Kenya where also 90% of the CAE were squamous cell carcinoma. Conclusion Many patients referred to endoscopy unit of Mulago hospital present with CAE and squamous cell carcinoma is the commonest histological type. Older age, male gender and smoking were identified as risk factors in this study. Therefore there is need to strengthen anti- smoking campaigns also to prevent CAE. The contribution of other potential risk factors such as human immunodeficiency syndrome and Human Papilloma Virus needs to be investigated. Acknowledgements J Menten for statistical advice and the SIDA-SAREC grant for the funding this study through the Faculty of Medicine. The authors do not have a conflict of interest. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08019t2.jpg] [hs08019t1.jpg] [hs08019t4.jpg] [hs08019t5.jpg] [hs08019t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}