 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 97-102 Felt stigma among people living with HIV/AIDS in rural and urban Kenya Violet N Yebeia,b, J D Fortenberryc, David O Ayukua aDepartment of Mental Health and Behavioural Sciences, Moi University School of Medicine Code Number: hs08022 Abstract Background: Individuals suffer from felt stigma when they internalize negative perceptions regarding themselves. People living
with HIV (PLWH) employ diverse coping mechanisms when their self worth and networks are disrupted by stigma. The social
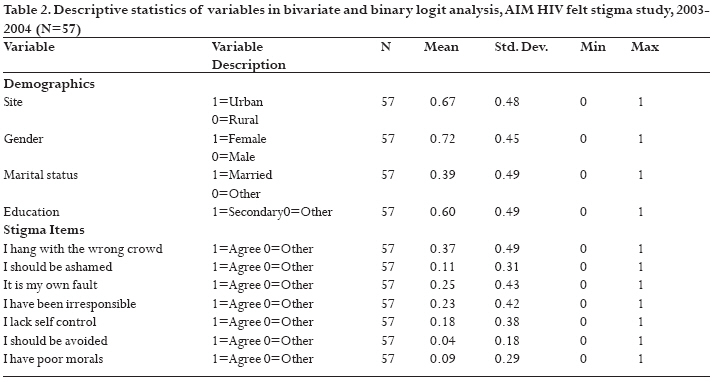
network perspective suggests response to stigma is shaped by social context. Introduction Stigma is a discrediting attribute that reduces individuals into degraded persons1. Stigma is conceptualized in different ways. Instrumental stigma is based on risk and resource concerns while symbolic stigma employs distancing of people2. Others distinguish felt stigma as what individuals perceive, and enacted stigma as acts of discrimination1. Generally, stigma hinders HIV prevention, disclosure, care-seeking and is linked to harmful unnecessary social polices3, 4, 5. The AIDS Initiative Movement (AIM) Kenya is composed of PLWH who work to combat stigma and share HIV information. AIM was initiated in 2002 by the Academic Model for Prevention and Treatment of HIV/AIDS (AMPATH), based at the School of Medicine, Moi University, Kenya6. Three types of stigmatized statuses are common; physical imperfection, character flaw and membership in `deviant' groups1. Disease stigma suggests people with specific diseases are different from others. Such judgments look beyond disease agents and add negative social baggage associated with the condition7. Stigma effects depend on stigma characteristics such as visibility, pervasiveness, salience, relevance, locus of responsibility, and removability8. When removal fails, different strategies are engaged like concealment, deflection of attention to less discrediting attributes, hiding information and avoidance of fellow sufferers1, 8. Irrespective of coping mechanisms, many still experience felt stigma by considering themselves inferior9. Those held responsible for their stigma find it more difficult to integrate with other members of society10. HIV/AIDS is highly stigmatized because it is associated with deviant groups, related to sex, linked to irresponsible behavior, and perceived to be contagious and dangerous10, 11. The social network perspective proposes that all societies are organized around a set of relationships12. This study utilizes the network perspective with special emphasis on Simmel's13 work on group affiliation. Using network theory allows us to link individual experiences such as HIV stigma, to broader social concerns. Simmel13 argues that social groups affect members, hence suggesting that an urban and rural dweller's social experiences would vary due to differences in social composition and constitution. Our study's objective is to explore whether HIV felt stigma differs with demographic characteristics and rural or urban location. Further, we explore whether there is variation in magnitude of change at the two sites over time. Methods In 2003, participants were drawn from the AIM support groups based at HIV clinics in Eldoret and Mosoriot, Kenya. Eldoret is the administrative centre of Uasin Gishu district, Kenya. The second site is a rural clinic at the Mosoriot Rural Training and Health Centre, which is situated in Mutwot location in Nandi District, Kenya. Participants were interviewed in two waves over a one year period14.The study was submitted to the Institutional Research and Ethics Committee based at Moi University School of Medicine for protocol approval prior to all research activities. The support groups served as points of contact with PLWH. Thus, all AIM members (80 urbanites and 23 in the rural) were approached during monthly support group meetings for face-to-face interviews. Each potential participant was given information on study objectives and expected involvement for one year. They were all informed that the study would examine whether HIV felt stigma differed with demographic characteristics and rural/urban location. Participation was voluntary and a sum of two hundred Kenya shillings ($2.50) was offered for lunch and transportation. While many urbanites expressed interest, not all availed themselves for interviews. Thus, in Wave one (2003), 41 (50%) Eldoret (urban) AIM members were interviewed, whereas in Mosoriot all 23 (100%) members were interviewed successfully because most Mosoriot (rural) members were from the region surrounding the clinic and were easily available. In Wave two (2004), a total of 38 interviews were conducted at the urban site, while the rural follow up realized 17 interviews. The attrition rate was higher in the rural (26%) than the urban site (7.3%). Loss of participants was attributed to death, migration, absenteeism, and inability to trace respondents. Research assistants were employed to conduct interviews. Most of the interviews took place within and in the vicinity of the two health facilities. Interviews were offered in both Swahili and English languages depending on the respondents' choice. Many preferred a combination of both languages which ensured a better understanding of the questions and enabled respondents to effortlessly provide answers. A semi-structured questionnaire was used to find out why AIM members joined the support group, whether their expectations were fulfilled, and on personal experiences of HIV stigma. All stigma items were standardized through utility of a likert scale. This paper focuses only on the felt stigma data. We specifically examine whether felt stigma varies by demographics, over time, and with rural-urban disparity. Analysis The dependent variable `felt stigma' was measured using seven stigma items that generally derive from dimensions of stigma described by Fortenberry15. They include: `I hang with the wrong crowd'; `I should be ashamed'; `It is my own fault'; `I have been irresponsible'; `I lack self control'; `I should be avoided'; and `I have poor morals'. These items reflect notions of deviance, shame, guilt, and isolation. Felt stigma description was on a 5 point scale ranging from strongly disagree (1) to strongly agree (5). Participants were asked to indicate the extent to which the scale items applied to them. To assess the properties of the stigma scale in this sample, Statistical Package for the Social Sciences (SPSS) was used to perform factor extraction through principal axis factor analysis and varimax rotation. Descriptive statistics are used to summarize general findings on the level and direction of change in all stigma items over time. Using the total sample in Wave one, all relevant variables for analysis are selected, recoded, cleaned and analyzed using STATA version 9. They include the seven felt stigma attributes as dependent variables and site, sex, age, education, employment and marital status as the independent variables. All cases missing on any of the variables of interest are dropped leaving a total of 57 cases. Dummy variables for site, sex, education, marital status and all felt stigma items are then created for the bivariate and logit analyses (see Table 2) which allow us to examine the relationship between demographics and participants that agreed/strongly agreed with felt stigma items. Given that only two respondents agree that they should be avoided in Wave one, this item is dropped out of the models. Finally, T-tests are used to compare each stigma item by waves and site. Results In Table 1, variables were coded as follows: gender (female=1, male=0); age (years lived); marital status (married=1, others=0); employment (unemployed=1, employed=0); and education level (1=incomplete primary, 2=complete primary, 3=secondary; 4=college level). Most respondents were female at both sites, and rural respondents were older. At least 46% (n = 19) urban and 35% (n = 8) rural respondents were married. More urbanites had completed secondary school education and although unemployment rate was high in both groups, it was relatively higher in the rural. Descriptive findings (see Table 2) for Wave one show that respondents had varying levels of felt stigma across the 1-5 scale. Factor analysis shows the correlation between scale items ranges from .004 to .739. To determine the number of factors to rotate, factors with eigen values greater than one were selected. Varimax rotation results in a 2-factor solution and a total of five items with 63.6% of the total variance explained. The first factor (self blame) includes three items on self control, fault and responsibility. The correlation between scale items ranges from .67 to .74 and this factor accounts for 37.7% of the variance. The second factor (self censure) includes two items on shame and avoidance, and they are correlated at a .69 level. This factor accounts for 25.9% of the variance. Internal consistency for both scales is high; self blame scale á = .87, while the self censure scale á = .82. Bivariate analysis (table available on request) shows that avoidance and poor morals items are insignificant when analyzed with demographic factors. Only 13% (n = 5, p<.05) of urbanites agree that HIV is a sign of irresponsibility while another 10% (n = 4, p<.10) of the urbanites agree HIV infection suggests lack of self control. About a third of the women agree HIV infection implies that one hang with wrong company (29%, n = 12, p<.10) and another 14% (n = 6, p<.05) agree if one gets HIV it is their own fault. Only 14 % (n = 6, p<.05) of the women agree HIV signifies that they have been irresponsible. Additionally, only one participant (p<.05) with secondary education agreed that he/she ought to be ashamed for getting HIV infection. In Table 3, binary logit findings suggest that gender and site differences are associated with levels of selected stigma attributes. Being female significantly decreases agreement with all stigma items except items on shame and poor morals. Being urbanite decreases agreement with being irresponsible and lacking self control. Looking at change in felt stigma over time, t-test analyses of Waves one and two in the urban show evidence to support the claim that there is a significant difference between the means in three items (see Table 4): `I hang with the wrong crowd' (t=2.13, p<.05); `I should be avoided' (t=1.99, p<.05); and `I have poor morals' (t=2.32, p<.05). In contrast, rural experience indicates insignificant change with time. Does the experience with various stigma attributes differ with location irrespective of the wave? There is a significant rural-urban difference (see Table 5) in items on: `It is my own fault' (t=-2.83, p<.05); `I have been irresponsible' (t=-2.52, p<.05); and `I lack self control' (t=-2.56, p<.05). This rural-urban discrepancy persists over time since we find significant difference after one year in all stigma items except for the shame item. Discussion This study describes AIM members' reports of felt HIV stigma. We examine whether felt stigma varies by socio-demographic characteristics, over time, and with rural-urban disparity. Findings suggest that gender and location influence individual's experience of felt HIV stigma. Being female significantly decreases agreement with the belief that HIV infection is a sign of having wrong company; HIV infection is their own fault; that they have been irresponsible; and that they lack self control. This finding may be explained by gender norms in Kenya that consent to multiple sex partners among males16. Hence, men may be blamed for infecting their female partners with HIV, and this may explain lower levels of internalized stigma among women. Unlike the rural group, urbanites experience significant difference in felt HIV stigma over time. To better understand site differences, we apply the network perspective. Simmel13 describes traditional forms of networks that are similar to many rural Kenyan communities such as the Nandi of Mosoriot. Individuals live in proximate environs, share a common culture and are interlocked in overlapping social networks17. Their networks form in concentric circles since participation in the smallest group implies participation in the larger groups 13. Albeit the inevitable social changes over time in Mosoriot, the Nandi are conservative and resistant to change18, 19. Langley18 and Oboler19 show that Nandi society is characterized by social classification in which individuals are controlled by group members. The Nandi are polite, respectful, quiet, hardworking and honest people who also have a proud independent spirit. A good Nandi is courageous and works hard for his family and community19. Langely18 adds that the Nandi traditionally limit behaviors such as beer drinking, child discipline, and sexual behavior. They maintain close family ties; in fact, female kin make conscious efforts to get married in the same region in order to support each other in times of need. Furthermore, close friendships are commonly converted to ties of affinity where it is convenient19. Compared to urbanites, AIM members in the rural may therefore maintain felt stigma overtime due to their premodern knit networks. On the other hand, Eldoret is a rapidly expanding melting pot of cultures. With continuous migration in Kenya, many settle in urban areas where interactions with similar tribal others persist, albeit to a limited extent. Therefore Eldoret can be classified as a modernizing area characterized by diverse social circles13. Reports of felt stigma may differ in Eldoret and Mosoriot because rural and urban regions vary in social networks; thus unlike their rural counterparts, PLWH in urban social circles may have opportunities to present identities free of the HIV label in some of their interactions. However, there may be other plausible explanations for the rural-urban differences noted. For example, the presence of large numbers of infected individuals in African urban areas20 may be associated with lower HIV felt stigma among urbanites. Factor analysis suggests two HIV felt stigma scales (self blame and self censure) that are relevant to issues of self-stigma and are applicable to this sample. We are considering further research utilizing more refined designs to illuminate these findings. The AIM support group has grown tremendously since 2002; the urban (Eldoret) clinic currently has 4,283 adults while the rural clinic (Mosoriot) has 1,455 members. Future research could examine how HIV stigma is shaped by participation in support groups. Conclusion This study describes changes in felt stigma over a period of one year in two sites in Kenya, one urban and one rural. Findings show that internalized feelings of HIV stigma may vary with social context and gender. Females significantly disagree with selected stigma items while urbanites experience significant change in felt HIV stigma over time unlike the rural sample. Experiences of felt stigma at the two locations irrespective of the study wave also show a significant rural-urban difference. This study has a few shortcomings that limit its generalizability. We had few participants; possibility of history and instrument reactivity; and Hawthorne effect21. To minimize these problems researchers dropped redundant questions in Wave two; had one year break between Waves; and encouraged commitment on the part of respondents and staff. Despite study limitations, this study suggests internalized feelings of HIV stigma may vary with social context and gender, hence, as AMPATH seeks to deliver all encompassing HIV/AIDS care in diverse localities, the experience of stigma ought to be addressed because stigma increases stress associated with illness, and thereby affects quality of life and physical well being (10). Additionally, interventions to support PLWH must take into account gender and unique social configurations that influence responses to illness. Future research utilizing larger populations of study can illuminate further why being urbanite and female seems to decrease agreement with HIV felt stigma attributes. Acknowledgements This research was supported by Bill and Melinda Gates foundation, Gates Grant No. 19135, within the broader activities of the Academic Model for Prevention and Treatment of HIV/AIDS, Kenya. We acknowledge the enormous contribution made by our dedicated research assistants and AIM support group members. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08022t5.jpg] [hs08022t3.jpg] [hs08022t2.jpg] [hs08022t4.jpg] [hs08022t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}