 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 103-107 Community understanding of pneumonia in Kenya Grace Irimu, R W Nduati , E Wafula, J Lenja University of Nairobi, Department of Paediatrics and Child Health, P. O. Box 19676-KNH, Nairobi,
Kenya., University of Nairobi, Department of Community Health Code Number: hs08023 Abstract Background: Effective management of pneumonia demands active participation by the caretaker to facilitate early seeking
of appropriate health care and adequate compliance to home
care messages. This would only be possible if the caretakers' perception of pneumonia is appropriate. This study aims to
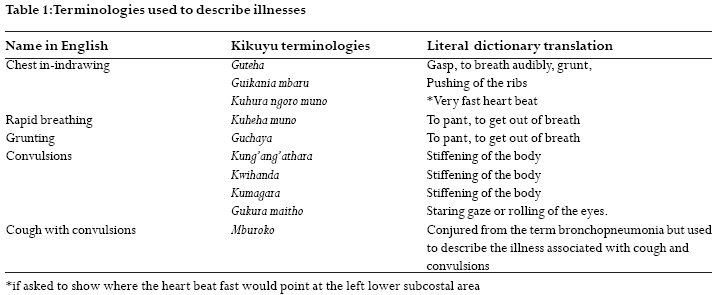
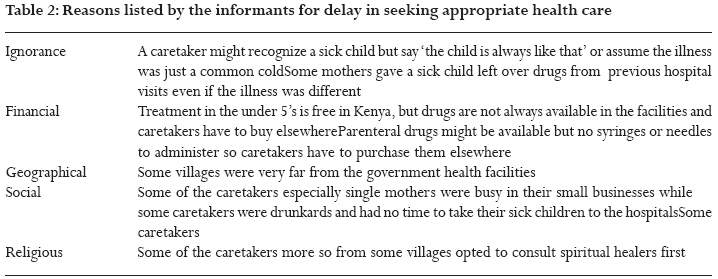
determine community's perception of childhood pneumonia in a suburb of Nairobi. Introduction Pneumonia is a major public health problem in children aged less than 5 years developing countries, with 150 million new clinical cases occurring each year, between 11-20 million ( 7-13%) of the children require hospitalization and two million die1. The World Health Organization (WHO) and UNICEF initiated a strategy for integrated management of childhood illnesses (IMCI) such as pneumonia at the health facility and community level. The community component of IMCI consists of education messages and programs in support of key family practices focused on health promotion, development as well early care seeking and compliance with health workers advice. Effective management of pneumonia entails active participation by the caretaker seeking appropriate health care and adequate adherence to home care messages. Adequate participation is only possible if the caretakers' perception of pneumonia is appropriate. Hitherto, the community perception of childhood pneumonia in suburban Nairobi, Kenya, has not been described. This study sought to establish the community's perception of the signs, symptoms and treatment of childhood pneumonia. Methods We carried out the study in Waithaka location of Kiambu district at the outskirts of Nairobi. Most families live in inadequate and overcrowded houses. About 80% of the inhabitants were Kikuyus who lived on family land. This was a descriptive study, which utilized qualitative data collection methods. These included in-depth interviews with the key leaders in the community and focus group discussions (FGDs) with the children's caretakers. Interviews were conducted in Kikuyu language and were audio recorded and later transcribed verbatim for analysis. Prior consent and permission to record the interviews was sought and confidentiality assured to respondents. The use of vernacular was aimed at gaining an understanding of the terminologies and phrases that the community used to describe childhood respiratory tract illnesses including the signs and symptoms. We therefore used terminologies understood by the community in the FGDs as gathered from the key informants interviews. Two secondary school leavers who were residents of Waithaka Location and were fluent in Kikuyu language were recruited to work as field assistants. They received one day training on recording verbatim of discussions and interviews. Individual in depth interviews After consulting with the village elders, six key informants were purposively selected one week before the study. The key informants were required to be articulate, willing and interested in talking about childhood illnesses. They included two community health workers (CHWs), one traditional birth attendant (TBA), one church leader, one elderly mother and a village elder. Even though the CHWs and TBA said they were not usually consulted on the care of sick children, they were interviewed as members of the community interested in childhood illnesses. The CHWs were involved in environmental sanitation and visiting homes of the sick to ensure they sought medical help but were not allowed to dispense any medication. The interview techniques used included free listing, paired comparative methods and open-ended questions. A pre-designed flexible topic guide was used for the key informant's in-depth interview. A pre-testing exercise of the study tools was used to assess their suitability and comprehension among respondents. During this exercise we realized the need of actual demonstration of the signs by the respondents to avoid misinterpretation. Information was sought on common illnesses in the locality: the illnesses were then ranked in order of severity. The informants were asked to list the illnesses presenting with cough and for each of the illnesses, they were asked to list the signs and symptoms. Precision of the description was confirmed by asking the informants to demonstrate the signs where possible. The reasons for categorizing one illness more severe than the other were explored. Paired comparative technique was applied for the frequently listed illnesses. The key informants explored terms and phrases used to describe the common illnesses in the locality. The reasons for categorizing one illness a being more severe than the other were probed. Focus group discussions Focus group discussions (FGDs) were carried out with mothers selected randomly from the community. We randomly selected four villages out of the nine villages in the study area. In each of the village, with the assistance of the village elders and the community health workers, we listed the names of the heads of the households with children aged less than 5 years on individual pieces of paper which were then put in a basket and the households to be studied were selected by the lottery method. Fifteen households were randomly selected from each village. From each household we recruited one mother with a child aged less than five years and in household with more than one eligible mother the youngest one was recruited. The mothers were subsequently grouped into eight groups. Each group had 6-8 participants. The participants in any given group were not familiar with one another so that they could be to free to discuss in the FGD. The principal investigator (PI) with the assistance of an anthropologist conducted the FGDs using an interview guide. The discussions were written verbatim and audio-taped. The discussions lasted 60-90 minutes per group. The participants were presented with a hypothetical case scenario of sick children followed by a series of questions to guide the discussion focusing on diagnosis made in the community and the recommended treatment. The terminologies and phrases used to describe signs and symptoms of pneumonia as revealed in the key informants' interview were applied in the description of the case scenarios. The PI demonstrated some of the signs to ensure they were understood precisely by the participants. The scenarios described two weeks old neonate, six months old infant and a two year old child with a cough for three days with varying severity of ARI. An example of a case scenario is depicted below. (Box 1). Each group was presented with three or four distinct scenarios. Box 1. Case scenario of an infant with cough, no pneumonia. You have visited your friend, Mumbi, a mother to six months old Alice. Mumbi usually seeks advice from you. She tells you that Alice has been running nose and coughing for the last two days. She does not feel hot on touch and her breathing has not changed. She is worried and asks you what the baby is likely to be suffering from. How and on what should she feed the baby on? What else can she give Alice at home? (Probe) Would you recommend her to seek care elsewhere? If the baby feels hot, what would you tell Mumbi the baby is likely to be suffering from and what can she do or give the baby at home. How and on what should she feed the baby? What else can she give Alice at home? (Probe)Would you recommend her to seek care elsewhere? Data analysis Although the common trend nowadays is to use qualitative data analysis software, this analysis was done manually. Recorded transcripts were transcribed verbatim and read severally to gain an in depth understanding of the key issues raised. These transcripts and the notes made during the interviews were then shared with another researcher not privy to the study, who together with the PI, independently identified the key themes which further informed the final analysis and interpretation. Key themes were identified using the terminologies and phrases used to describe pneumonia and the perceived signs and symptoms and constant comparison techniques were applied. Themes identified by the two researchers were then compared for consensus. During the initial identification of the themes, methodological triangulation of data collected using different techniques was done to obtain a consensus of the interviews. Results In-depth key informants interview Terms and phrases used to describe pneumonia The key informants listed `diarrhoea and vomiting' or cough as the most common illnesses. `Diarrhoea and vomiting' was mentioned as a single entity. Others listed were measles and malaria. Pneumonia, malaria, measles, asthma and common cold were illnesses perceived to present with cough. All the informants ranked pneumonia as the most serious childhood illness in the locality, measles was ranked second and `diarrhea and vomiting' third. The key informants used diverse terminologies and phrases to describe signs and symptoms of pneumonia. `Rimunia' is the Kikuyu word used for severe pneumonia by all the informants. It was notable that fever, difficult in breathing, chest in-drawing and convulsions were mentioned by all the informants as features of pneumonia. The terminology commonly used to denote chest in-drawing was `guteha' . `Guteha', literally means grunting but in the study area it was used to denote chest indrawing. In fact in this area, chest in-drawing (guteha) was synonymous with rimunia or severe pneumonia. Other terms used to describe chest indrawing were `guikania mbaru' and `kuhura ngoro muno'. The former literally translates to `pushing of the ribs' while the latter translates to `very fast heart beat'. Although `kuheha muno' means `to breath fast', it was not used to describe fast breathing without chest in-drawing (Table 1). There was no word used to describe fast breathing without chest in-drawing. The key informants believed that fever was crucial for diagnosis of severe pneumonia or rimunia. A child without fever was unlikely to have rimunia except if rimunia was `hidden' and in such cases only the doctor could make the diagnosis. Chest in-drawing without fever was also perceived as "hidden pneumonia". Two of the informants said that if a child with cough developed fever without chest in-drawing , that would be recognized as `mild pneumonia' while once the child had chest in-drawing that would be considered as severe pneumonia.Five of the informants said chest pain in a child with cough was also perceived as rimunia. The older child would complain of it but the younger child would cry if held by the chest. Pneumonia was also associated with startling at night in contrast to malaria, which was associated with startling throughout the day and night. One of the informants said pneumonia could present as grunting while all the others said it was due to malaria. Refusal to feed was also associated with pneumonia. Some informants said that any serous illness could make a child unable to feed. However if a child did not look sick that illness was generally perceived as malaria. Rimnia nini or `mild pneumonia' in this community was used to describe cough associated with fever with or without fast breathing so long as there was no chest indrawing. This was not a taken seriously by the community and was treated with an anti-malarial or antipyretics. All key informants listed shedding of tears, running nose and nasal blockage as features of common cold `homa'. The child would feed well in most cases. Two of the informants said that if the children had fever the illness would be perceived as `mild pneumonia'. If the child developed convulsions then the child would be said to have `mburoko'. Convulsions were described using different names indicating stiffening of the body (kung'ang'athara, kwihanda, kumagara) and rolling of the eyes (gukura maitho). All the key informants perceived fever, grunting and startling all the time as features of malaria. Grunting and startling all the time were features that differentiated rimunia from malaria. Other signs and symptoms for malaria listed by at least five of the informants included refusal to feed, `diarrhoea and vomiting', hallucination and chills. Health seeking and causes of delayed care seeking There was no known home treatment for rimunia and the informants said a child had to be taken to hospital `immediately'. Other reasons why a caretaker sought immediate health care for a child with a cough were high fever and convulsions (`mburoko'). The informants cited various reasons for delay in seeking immediate care namely ignorance, financial, geographical, social and religious (table 2). Focus group discussions Consensus of diagnosis made for the case scenarios There was consensus that a child with cough, running nose or blocked nose, but without fever, regardless of the age, had common cold in all the groups. When fever was added to the scenario there was still consensus that the neonate had `rimunia' and the two year old child had common cold. There was no consensus in any of the groups for the diagnosis of the scenario of a febrile six months old infant with similar symptoms and signs; some of the participants thought the infant had common cold or malaria. Case scenarios of children with different ages with a cough, fast breathing but no chest in-drawing were presented to the groups. For the two weeks old neonate with fever there was consensus in all the groups that the neonate had rimunia but few participants said the child could have stomachache too. However there was no consensus on diagnosis in the scenario of afebrile neonate. Participants felt the child could have pneumonia or stomachache. Regarding the six months old infant and two year old child there was consensus that the children had `mild pneumonia'. If fever was added to the scenario there was no consensus with some participants making a diagnosis of malaria or rimunia. There was consensus in the case scenario of a child with cough and chest in-drawing with or without fever that the child had rimunia. However in the scenario for the neonate some participants felt the child could have stomachache too.Sugar salt solution (SSS) was recommended for treatment of stomachache, antipyretic for mild pneumonia, and an antimalarial for malaria. All the groups agreed there was no home treatment for "rimunia" and the child should be taken to hospital. The participants also said a very young child was not to be given drugs `just like that'. The participants were asked how they would manage a child with fever. There was consensus that a child with fever should be undressed, wiped with luke-warm water and given antipyretics. But the participants thought that the neonate was too young to be exposed and to receive home treatment with antipyretics and all recommended that a neonate with body hotness should be taken to the hospital. Regarding feeding during illness there was consensus in all the groups that the very young child should be fed on breast milk only. The older child would continue with feeds but was denied some food stuffs namely fried foods, cold foods, milk and fruits like avocadoes and bananas. These were believed to be too strong for the sick child and that their consumption would make pneumonia worse while eggs were believed to cause a child with a cough to develop pneumonia. Discussion The study community was familiar with and used medical terms like pneumonia, malaria and bronchopneumonia. However the signs, symptoms and treatment for each of these differed considerably from the biomedical concept. Health workers and the caretakers may be using the same words but their understanding of these terminologies may be different. This qualitative research provided an opportunity to elicit the differences and careful explanation of what the terms used to describe pneumonia were understood by the community. Terms for chest in drawing, labored breathing and convulsions were diverse and yet specific. Other ethnographic studies in ARI have documented similar diversity of terms 2,3. Chest in-drawing was synonymous to `rimunia' or severe pneumonia. Severe pneumonia was therefore easily recognized and appreciated as the most severe childhood disease in the community. Inability to differentiate severe pneumonia from stomachache in neonates in case scenarios was noted in the FGDs. This could lead to inappropriately treating the neonate with severe pneumonia with SSS at home. The community had no term for rapid breathing; this is in contrast with what has been found in a community in Western Uganda, although even in this community it rarely prompted health care4. Even with description in the scenario in FGDs, caretakers were unable to recognize the significance of rapid breathing. Fast breathing in a child with cough is the key sign of pneumonia 5-7. In developing countries according to the IMCI case management guidelines, pneumonia is presumed to be of bacterial origin, antibiotic therapy should be instituted promptly. Many of the ARI deaths occur within 3-5 days of disease onset 8. Failure to recognize fast breathing may result in delay in seeking appropriate health care and hence delay treatment resulting into avoidable deaths. Mild pneumonia, though it refers to an illness that requires antibiotic treatment, in this community, it was regarded as a mild illness that could be treated with antipyretics or anti-malarials. Early recognition of pneumonia by the child's caretaker and appropriate health seeking are essential for the reduction of mortality. Understanding how locally recognized signs and symptoms relate to the clinical definition of pneumonia is important in constructing messages that families can understand and which they are likely to adhere to. Caretakers continued giving a sick child feeds during an ARI event but denied the child certain important foodstuffs like fried foods, eggs and milk. This is detrimental in a country in which the prevalence of underweight in the children aged less than 5 years is as high as 20% 9. Community health education is required to empower the caretaker with an understanding to appreciate and recognize signs and symptoms of pneumonia as well as understand the appropriate supportive care. This will enable the caretaker to perceive pneumonia disease for what it should be, and improve adherence to health care messages. There were several reasons for delayed care seeking in this community which should be addressed in the community IMCI. Financial constraints and perception that an illness is not serious have similarly been described in a city slum in Kenya to be main reasons given for failure to seek health care outside home10. The findings of this study cannot be generalized to the national level but they do identify strengths and weaknesses in community perception of pneumonia that will be of interest in the development and adaptation of the training materials for community IMCI. Acknowledgement The authors are grateful to Prof. W. M. Macharia for having reviewed the manuscript and for his useful comments. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08023t1.jpg] [hs08023t2.jpg] |
| |||||||||

{kind=link}
{kind=link}