 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 114-119 Malaria and mosquito net utilisation among schoolchildren in villages with or without healthcare facilities at different altitudes in Iringa District, Tanzania Leonard EG Mboera*1, Mathias L Kamugisha2, Susan F Rumisha1, William N Kisinza1, Kesheni P Senkoro1, Andrew Y Kitua1 1National Institute for Medical Research, P.O. Box 9653, Dar es Salaam, Tanzania Code Number: hs08025 Abstract
Background: The endemicity of malaria in Tanzania is heterogenous, mainly associated with physical factors such as
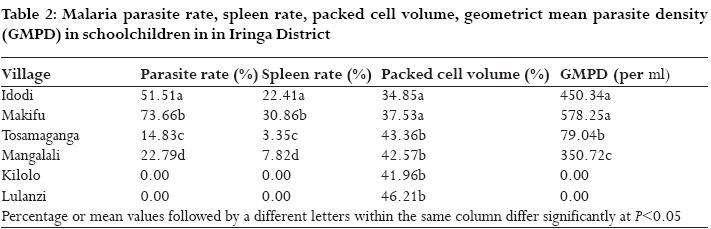
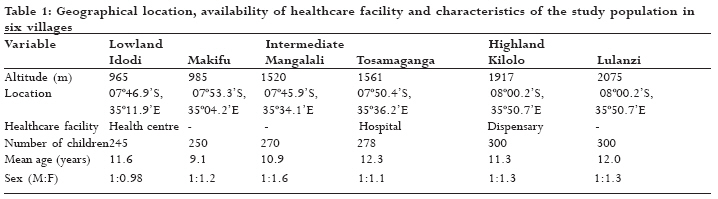
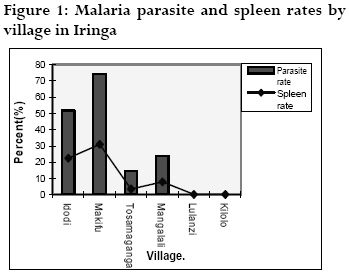
topography, climate and socio-economic status. The contributions of these factors in many regions of Tanzania have not been studied in detail. Introduction Malaria remains a major cause of morbidity and mortality, with an over 600 million cases and over 2 million deaths each year worldwide. Over 90% of the cases occur in sub-Saharan Africa where falciparum malaria is pervasive and the the major killer of children <5 years old1. For many years malaria in Africa has been categorized into levels of endemicity (as hypo-, meso-, hyper- or holoendemic) or as stable and unstable transmission 2, 3. Such classification does not consider fine differences in transmission intensity that may influence the outcome of malaria associated morbidity within the same geographical locality. Comparing areas of different endemicity is a means of understanding the relationship between the environmental and socio-economic risk factors in malaria transmission and acquisition of parasites and hence malaria morbidity. Factors that influence malaria transmission and malaria risk are manifold, but a major distinction can be made between intrinsic and extrinsic risk factors. Intrinsic factors may be defined as characteristics belonging either to the parasite, vector or host and which are not part of the natural environment 4. Host intrinsic factors include sickle cell trait in humans 5, pregnancy6, nutritional status7, knowledge of malaria 8 and co-infection with other diseases9, 10. Extrinsic factors which include physical and biological factors mostly affect the development and survival of the mosquito and the parasite (temperature, rainfall, humidity, vegetation, alternative hosts, etc), while human activities, behaviour and living conditions (socio-economic factors) may provide an additional risk as a result of an increased exposure to the disease. Recently in a study in central Tanzania malaria prevalence was observed to vary between villages with and without healthcare facilities, located at similar altitudes11. To what extent environmental, socio-economic and other factors indeed contribute to an increased risk of malaria remains unclear in most parts of Tanzania and are subject for further research. It was therefore the objective of this study to determine malaria parasitaemia and transmission and utilisation of mosquito nets among schoolchildren in villages with or without healthcare facility in Iringa District, Tanzania. Methods Study area This cross-sectional study was carried out in Iringa district (7o35'S, 35o30'E) in Tanzania. The district comprises of three distinctive landscape zones which were categorised for the purpose of this study as high-, intermediate and lowland zones. The highland zone (>1600 m) is characterised by mountainous and undulating topography. The mean annual rainfall is about 1300mm. The highlands are usually cold with an average temperature of 15oC. The intermediate zone (1001-1600m) is characterised by scattered mountain hills and flat areas with swamps and ponds. The area receives a mean annual rainfall of 600-1000mm. The annual mean temperature ranges between 15 and 20oC. The lowland zone (≤1000 m) lies within the Great Rift Valley, and is usually dry, hot with mean annual rainfall of 500-600mm and mean annual temperature of 20-30oC. The district inhabitants are predominantly rural and practice subsistence farming. Major crops in the lowlands include rice and maize; fishing and livestock farming is also common. In the intermediate zone, major crops include maize, tobacco, onions, sweet potatoes, sunflower, sorghum, and tropical fruits. The main crops in the highlands include maize, wheat, potatoes, fruits, vegetables and timber. The district was stratified into three strata based on the altitude. Then a random sample of two villages (with and without healthcare facility) was selected in each stratum. The villages were Idodi and Makifu (lowlands), Mangalali and Tosamaganga (intermediate) and Kilolo and Lulanzi (highlands). Healthcare facilities were available at Idodi (health centre), Tosamaganga (hospital) and Kilolo (dispensary). The average distance between villages in the same stratum was 11 km. The altitudes and coordinates of the selected study areas were determined at the central point of each village using a hand-held Global Positioning Satellite receiver. The sample size calculation was based on the anticipated malaria prevalence to be between 20-30% according to the proportion of malaria cases reported in the district. The true value was expected to be within 95% confidence interval with relative precision of 0.10. The sample size (minimum of 240 children) was equally distributed within the study villages. Malariometric surveys Malariometric surveys were carried out to cover a sample of schoolchildren in schools, one in each village. The aim was to screen 1800 schoolchildren in the six villages. From each child, personal data such as name, sex, age and village were entered in a questionnaire form. Each child was examined clinically and thick and thin blood smears were collected from a finger prick. The blood smears were stained with 10% Giemsa in phosphate buffer (pH 7.2) and examined under a microscope at 1000x magnification to identify any malaria parasite species present. Enumeration of the malaria parasite was made and parasites were counted against 200 leukocytes. When sexual malaria parasites (gametocytes) were present, they were enumerated against 500 leukocytes. Parasite rate, geometric mean of parasite density, gametocyte rates and density indices were then determined. All schoolchildren were palpated in a horizontal position for the presence of enlarged spleen by a medical doctor3. Each child screened for malaria parasite was asked whether he/she slept under a mosquito net during the previous night. Fingerprick blood from a representative sample of pupils (50 children) from each village was taken into heparinised capillary tubes for packed cell volume (PCV) determination12. Entomological surveys Entomological surveys were conducted in the same villages where the parasitological surveys were done. Mosquito collections were done in 10 houses in each village using pyrethrum spray catch technique. As much as possible, sentinel houses were of similar construction to avoid the effect of variability caused by differences in construction. All mosquito collections were morphologically identified, sorted according to site of collection, house, date and species. Female Anopheles gambiae s.l. were dissected to determine parity by observing the degree of coiling of ovarian tracheoles (13). Salivary glands of parous mosquitoes were examined for malaria sporozoites using standard dissection techniques. Data analysis All data were entered and verified in Microsoft Excel or Access and analysed using STATA statistical analysis software package version 8 (Stata Corp., College Station, TX, USA, 2003). In order to investigate whether there was a relationship between parasitaemia and the absence or presence of healthcare facility, we explored the distribution of variables and summarised the statistics of each individual variable. For the continuous variables such as age of children and PCV level, Shapiro-Wilk test was used to check for normality. Chi-square test was done to determine whether there was an association between malaria parasitaemia and other categorical variables such as altitude and presence of healthcare facility. The magnitude of the effect between strata and presence of healthcare facility in relation to malaria prevalence was obtained using logistic regression analysis. Ethical consideration In each school, meetings were held with the teachers, to explain the purpose and methodology of the study before the screening was done. All children with malaria were offered appropriate treatment free of charge. Ethical clearance was granted by the Medical Research Coordination Committee of the National Institute for Medical Research. Results There was a high participation, with 91.3% of the target sample recruited in the survey. A total of 1643 children (mean age range = 5.9-12.3 years) were screened for malaria parasites. The sexes were almost equally represented; however, girls formed a slightly higher proportion of the study subjects in all schools except in Idodi (Table 1). Plasmodium falciparum (93.1%) was the predominant species of malaria in the district. P. malariae and mixed infections of P. falciparum + P. malariae and P. falciparum+P. ovale and P. malariae+ P. ovale accounted for 2.5%, 3.7%, 0.5% and 0.2%, respectively. The overall district mean prevalence rate of P. falciparum was 25.9% (418/1614). Parasite prevalence decreased with increasing altitude. It was 62.6% in the lowlands, 18.8% in the intermediate and 0% in the highlands. Children in villages in the intermediate transect were at lower risk of getting malaria infection by 16% (95% CI: 10% - 24%, P<0.01) than those in the lowlands. Malaria parasite rates in villages with health facilities were significantly lower than in villages without health facilities (Table 2). Communities living in areas without health facilities in the lowland and intermediate transect were at a higher risk of acquiring malaria infection by 35% (95% CI: 24% - 52%, P<0.001) and 55% (95% CI: 34% - 88%, P=0.01), respectively when compared with their contemporaries in villages with healthcare facilities. The geometric means of parasite density (GMPD) for P. falciparum in the lowlands and intermediate transects were 499.8 and 231.5/ml of blood, respectively. The GMPD was 2.4 higher among children in the low than in the intermediate altitudes (P<0.01). Higher mean parasite density was observed among schoolchildren in villages without healthcare facilities than in those with healthcare facilities (P<0.01) (Table 2). P. falciparum gametocytes were observed in 0.73% (12/1635) of the children. The gametocyte rate was significantly higher in the low- (1.5%) than in the intermediate altitudes (0.6%) (P< 0.0001). A total of 172 (10.5%) of the children had enlarged spleen. Of the children with enlarged spleens, 82.6% were from villages in the lowlands. Spleen rate was higher (26.6%) in the lowlands and lower (5.6%) in the intermediate transect. Spleen enlargement was not observed among children in the highlands. The spleen rates were significantly lower in villages with healthcare facilities in both lowland (Idodi=22.4% The packed cell volumes (PCV) were significantly higher among children in the highland than in the lowland villages (P<0.05) (Table 1). There was no significant difference between PCV in children between villages with and without healthcare facilities.Of the screened children, 16.1% (264/1643) slept under a mosquito net during the previous night. Mosquito net coverage was 41.1, 16.5, 24.2, 16.3, 1.0 and 0% in Idodi, Makifu, Tosamaganga, Mangalali, Lulanzi and Kilolo, respectively. Mosquito net coverage was higher in lowland villages, accounting for 61.7% (163/264) of the total net use in the district. The majority (75.5%) of the mosquito net users were from village with health facilities (P<0.001). Further analysis showed that in 73.6% (253/344) of the schoolchildren who had malaria parasites were not using mosquito nets. Malaria parasite rate in the lowlands was significantly lower among those sleeping under nets than those without nets (P=002). However, this variation was not observed among infected children in the intermediate transect villages (P>0.05). A total of 228 mosquitoes were collected in six villages. Of these, 53.5% (N=122) were An. gambiae s.l., 1.8% (N=4) were An. funestus, and 43.4% (N=99) were Culex quinquefasciatus. Other species accounted for 1.3% (N=3). Larger numbers of An. gambiae s.l. and Cx quinquefasciatus were collected in Makifu and Tosamaganga, respectively. The average density of the An. gambiae s.l. was 4 per room. Overall, 8.7% of An. gambiae s.l. were infected with malaria sporozoites. The sporozoite rate was highest in mosquitoes collected in Idodi (14.3%). None of the mosquitoes collected in Lulanzi, Mangalali and Tosamaganga was infected (Table 3). Discussion Malaria parasite prevalence in Iringa district varied markedly with altitude, ranging from 0 to 73.66%. Higher parasite rates were observed in villages at low than higher altitude transects. Children from villages at higher altitudes (>1900m) were not infected with malaria parasites. Previous studies around Iringa Municipality (1600m) showed a lower prevalence of 13% among children aged up to 10 years old2. In the lowland villages of Iringa district, malaria parasite rates of between 59.3% and 80.6% among children have been reported by other investigators13, 14. The inverse relationship between malaria prevalence and altitude has been reported elsewhere in Tanzania. In a study in Usambara Mountains in north-east Tanzania, a prevalence of malaria in children was observed to decrease by 5% for every 100 m increase in altitude from 82% in the lowlands (300m) to 12% in the highlands (1700m) 16. In another study in northern Tanzania17 a 19% and 21% decrease in malaria prevalence has been observed, for every 100m altitude increase. The lower malaria prevalence in the higher altitude is likely to be attributed to the low ambient temperatures19. Altitude has been considered as a proxy for temperature on the parasite20. However, local variations in seasonality of malaria transmission including vector species composition, topography, host and parasite genetics, and socio-economic factors influence malaria prevalence in any given area17. Malaria parasite and spleen rates and malaria parasite densities among children in villages with healthcare facilities were significantly lower than in villages without healthcare facilities. Similar observations have been made in a nearby district of Mpwapwa11. The accessibility of the community to early treatment is likely to play a significant role in the lower parasite and spleen rates in villages with health facilities. It is likely that the availability of prompt treatment reduces the number of individuals with malaria parasite and the density of parasite circulating in their blood (as shown by the low gametocyte rates among children in villages with healthcare facilities). The presence of gametocytes is commonly used as a parameter of malaria transmission 20. Moreover, communities close to health facilities are expected to be more aware of the disease and its treatment and control; the knowledge which may be obtained from health facilities. On the other hand, those living far from health facilities are likely to seek treatment late and thus live with the parasites in their blood and hence providing a reservoir of malaria infection. In this study, higher spleen rates were observed in villages located in lower altitudes and those without healthcare facilities. Usually, spleen enlargement indicates the endemicity of malaria in a given region. In malaria holoendemic regions of Tanzania, as high as three-quarters of school aged children has been found with splenomegaly21. Such high spleen rates indicate an intensive malaria exposure of the population to malaria parasite. The low spleen rates among children in villages with healthcare facilities are likely to be attributed to easy accessibility to early malaria treatment. Higher packed cell volume, an indication of haematocrit level was observed among children in the highland villages. Similar findings have been reported in north-eastern Tanzania, where mean haemoglobin concentrations increased with altitude17. An. gambiae s.l. is the predominant malaria vector in the district. Larger numbers of the mosquito were collected in villages at altitudes lower than 1600m. It is in the same villages that mature and infective mosquitoes were collected, indicating that more malaria transmission is taking place in the lowland than intermediate or highland transect villages. Like in our study, in Kenya, mosquito vectors have been found at altitudes from 1600m to 3000m19, 22. The low mosquito densities found in our study are likely to have been due to ecological factors or the sampling technique used. Spray catches have been found to under-estimate the abundance of exophilic Anopheles mosquitoes in northern Tanzania23. In this study, the proportion of sporozoite-infected mosquitoes (sporozoite rate) was found to be quite variable from village to village. The higher sporozoite rates (4.3-14.3%) found in this area were probably due to a small sample size of the mosquitoes collected. However, these are among the highest sporozoite rates ever recorded in Tanzania21, 24. Similar to our findings, the pattern of malaria transmission elsewhere in Tanzania varies markedly from area to area, depending on climate and biogeography17, 21. Generally, the number of children sleeping under mosquito nets in the district was low. However, it was relatively higher among residents of villages at low altitudes where malaria was more prevalent. Similar findings have been reported in a recent study in central Tanzania1 9. At high mosquito densities and high malaria prevalence, people tend to protect themselves by using mosquito nets25, 26. Moreover, mosquito net use coverage was significantly higher among children in the villages with health facilities than from those without. This is likely to be a result of continuous health education provided at health facilities, creating awareness of the importance of self-protection against malaria. In a recent study27 in a nearby district of Dodoma, it was observed that most of the information, education and communication materials such as posters are found at health care facilities than elsewhere in the district and that healthcare facilities are among the most important source of health education. This means, communities living close to such facilities have much more access to health information than those living far from the facilities. It has already been established that a population which is knowledgeable about the use of personal protection measures and can afford them, which understands the importance of seeking effective treatment at the first sign of illness, and can pay for health services and drugs, have substantially reduced disease morbidity, despite being in an area of high risks28. The use of mosquito nets has shown a beneficial effect in Iringa district where the majority of the children with malaria parasites were reported not using nets. Results of our study indicate that the prevalence of malaria infection is likely to be higher among communities who live at great distances from health care services and those not using mosquito nets. In conclusion, the results of this study show that malaria prevalence and intensity varied considerably throughout the district, with children from villages at low altitudes and/ or without healthcare facilities forming the largest proportion of malaria-infected populations. Mosquito net ownership and coverage is high in areas with health facilities than in those without. These results provide more evidence of the existence of the relationship between altitude variability or accessibility to health services, and the burden of malaria in rural communities of Tanzania. These relationships are however, complex and must be viewed in the context of other environmental and socio-economic factors. Acknowledgements The authors wish to thank G.J. Chuwa, B. Mkumbwike, A. Khihatura, L. Kadete, F. Mgohamwende, M. Mohamedi, B. Chambika, D. Mwanjeluka and A. Mathias for their excellent technical assistance. Special thanks are due to Dr. Jasper Ijumba for his invaluable comments on an earlier version of the manuscript. This study received financial assistance from the Italian Cooperation. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08025t3.jpg] [hs08025t2.jpg] [hs08025t1.jpg] [hs08025f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}