 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 120-125 Effect of sex education programme on at-risk sexual behaviour of school-going adolescents in Ilorin, Nigeria Mary Ogechi Esere University of Ilorin, Nigeria Code Number: hs08026 Abstract Background: Adolescents display sexual behaviours and developmental characteristics that place them at risk for Sexually
Transmitted Diseases (STDs). Because young people experiment sexually and because of the consequences of indiscriminate sexual activities on
the youth, there is the need to mount sex education programmes that are geared towards enlightenment and appropriate education
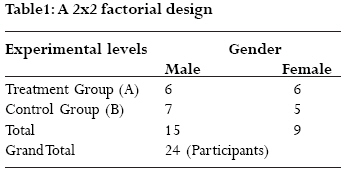
about sex and sexuality. Key words: Sex Education; At-Risk Sexual Behaviour; School-Going Adolescents, Nigeria. Introduction The period of adolescence occupies a unique stage in every person's life. It is a period of transition from childhood to adulthood1. Adolescence has been described as a stage among human beings where a lot of physiological as well as anatomical changes take place resulting in reproductive maturity in the adolescents2. Many adolescents manage this transformation successfully while others experience major stress and find themselves engaging in behaviours (e.g. sexual experimentation, exploration and promiscuity etc.) that place their well-being at risk3. Adolescents display sexual behaviours and developmental characteristics that place them at risk for Sexually Transmitted Diseases (STDs). A primary source of risk of HIV/AIDS for instance is unprotected /indiscriminate sexual activity4. By the time they are 18, most adolescents in Nigeria are sexually active). Despite increased sexual knowledge6, adolescents in Nigeria are poor contraceptive users7. They are less likely than adults to consistently use condoms or other methods of protection that could reduce their chances of infection8. Neither specific teaching about contraception nor improving the contraceptive service consistently increases effective contraceptive use by young teenagers9. Adolescents having sexual intercourse before age 16 are more likely to take risks10. They have more sexual partners during their lifetime and more partners per year and they start sexual activity earlier in new relationships than those who become sexually active after age 1611. In Nigeria today, sex education is yet to be incorporated into the curricula of secondary school education12. Many Nigerians are reluctant to discuss sexuality and sexual health openly. In most African countries, Nigeria in particular, matters relating to sex and sexuality are usually shrouded in secrecy13. Neither the adolescent boy nor girl has free access to the information he or she needs on sexuality. Questions bordering on sexuality and girl-boy relationships are usually hushed up and regarded as taboos14. The consequence of this action is that Nigerian adolescent boys and girls find answers to sex-related questions on their own, often from questionable sources that are likely to give them wrong information15,16, making them more likely to indulge in reckless and unguarded sexual experimentation. Some adolescents lack adequate communication and assertiveness skills to negotiate safer sex17. Some feel unable to refuse unwanted sex or feel compelled to exchange sex for money.18, 19. Because young people experiment sexually20 and because of the consequences of indiscriminate sexual activities on the youth, there is the need to mount sex education programmes that are geared towards enlightenment and appropriate education about sex and sexuality. This is the focus of this study. Consequences of Early Sexual Activity In Nigeria, problems associated with adolescents' sexual health include high rates of teenage pregnancy21; a rising incidence of sexually transmitted diseases22, 23, high rates of abortion mortality24, etc. Medical problems associated with adolescents' sexual behaviour are a major health burden to Nigerians. Problems are not confined to pregnancy but include secondary infertility and development of cervical abnormalities in adolescents25. Early sexual activity has negative consequences for young people. Adolescents who become sexually active enter an arena of high-risk behaviour that leads to physical and emotional damage 26. Each year, influenced by a combination of a youthful assumption of invincibility, and a lack of guidance (or misguidance and misleading information), millions of adolescents ignore those risks and suffer the consequences. Young men who have sex with men are at high risk for HIV and other sexually transmitted diseases. It has been found that individuals infected with an STD are at least two to five times more likely than uninfected individuals to acquire HIV if exposed to the virus through sexual contact27. One study found that among gay male clinic patients screened for STDs, those 15 to 20 years old had the highest age-specific rates of rectal Chlamydia and gonorrhea28. These findings suggest the need for effective sex education for the young ones. Sex Education Sex education is a process whereby information is given or imparted to a group of young ones and which takes into account the development, growth, the anatomy and physiology of the human reproductive system and changes that occur from youth all through stages of adulthood29. Sex education is the acquisition of knowledge that deals with human sexuality30. It consists of instruction on the development of an understanding of the physical, mental, emotional, social, economic and psychological phases of human relations as they are affected by sex. In other words, sex education involves providing children with knowledge and concept that will enable them make informed and responsible decisions about sexual behaviours at all stages of their lives. The aims of sex education, according to British Medical Association Foundation for AIDS, 31, are ambitious relating to the lifelong quality of relationships and personal behaviour. It should be age appropriate and available to everyone through a variety of forms and informal settings. Since adolescents' characteristics predispose them to high risky sexual activities, behavioural interventions are needed to reduce their at-risk sexual behaviours. The present study is an attempt in this direction. Objective: To determine whether Sex Education Intervention Programme would reduce at-risk sexual behaviours of school-going adolescents. Method Research Design This study adopted pre test, post test control group quasi-experimental design using a two (2) by two (2) factorial analyses (See Table 1). The treatment group and the control group constituted the row and gender formed the column. Participants and Setting A total of twenty four (24) students, drawn from a mixed sex secondary school in Ilorin Metropolis constituted the study sample. Initially, a total of 200 students were involved in the preliminary screening exercise. The "At-Risk Sexual Behaviuor Scale" was administered to all the 200 students. After scoring, the scores ranged between 20 and 50. A cumulative frequency of the scores was prepared and those with scores corresponding to the 66th percentile and above were classified as having high at-risk sexual behaviour. Eighty (80) out of the 200 students fell into this category. The 80 students were then selected using a stratified random sampling technique to gather a cross-sectional sample across gender, ethnic groups, age and religious affiliations. Through this process the sample was reduced to 40. A couple of criteria were satisfied by the participants before they were deemed qualified for selection into the experimental programme. These include:
On the recruitment day, the participants who met the requirements for selection were randomly assigned to the two experimental groups (The treatment group and the control group). The mean age of the participants was 15.50 years, while the age range was between 13 and 19 years. Instrument The participants completed the At-Risk Sexual Behaviour Scale (developed by the researcher) before and after the experimental programme. The instrument was formatted on a 4-point Likert type scale, consisting of two sections. Section A deals with personal characteristics of the participants while section B has 20 items comprising statements on at-risk sexual behaviour such as: I i) Have multiple sexual partners; ii) Participate in group sex; iii) Do not use condoms while having sex; iv) Get involved in anal sex,; v) Get involved in oral sex etc. For the purpose of this study, the higher the total score, the higher the at-risk sexual behaviour of the adolescents and vice versa. Requesting experts in the related field of study to vet the instrument established its content validity. The panel of experts made various suggestions which were taken into account, and necessary corrections were made. Following the consensus of the experts on the suitability of the instrument for use in the study, they were adjudged valid. The reliability of the instrument was determined, through Cronbach alpha reliability technique with a coefficient value of 0.73. This lends credence to the suitability of the instrument for the study. Procedure for Treatment The procedure for collecting data was divided and was carried out in two stages as follows:
Pre-treatment phase: On the recruitment day, after the introductory talk, those who would not find the programme convenient were asked to leave. Twenty six out of the fifty adolescents who met the requirements for inclusion (see the section on participants and setting) indicated their unwillingness to participate in the experimental programme and were allowed to leave remaining twenty four adolescents. These were randomly assigned to the following groups:
The author retained the control group and "tied" them down by giving them a placebo. A different day was used for the casual meetings with the control group so as to avoid "contamination" with the treatment group. Control of Extraneous Variables The author took certain steps to prevent or at least minimize the incursion of extraneous variables into the experimental programme. Some of those steps include:
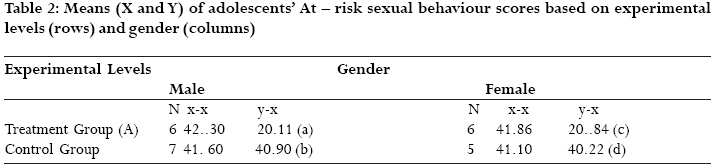
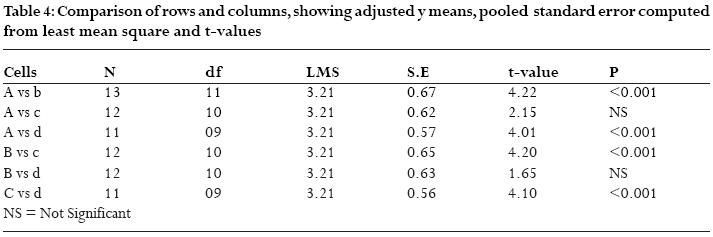
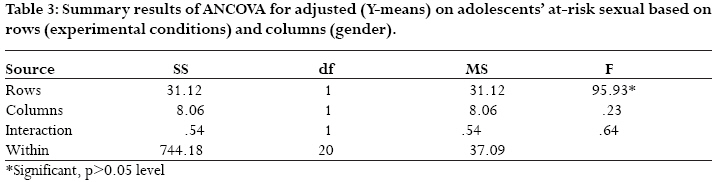
The Treatment Phase: The participants that received the treatment (SEP) were those in the experimental group A. The SEP intervention is an 8 sessions (1 session per week) programme. It is intended to reduce at-risk/unsafe sexual behaviours of school-going adolescents, and improve the quality of sexual relationships. The programme combines active learning (e.g. work in small groups and games), information leaflets on sexual health, and development of skills, primarily through role playing. It has the 10 characteristics identified by 32,33 as necessary for effective programmes. The content incorporated strategies identified as potentially successful from a review of health education literature and projects34. Subjects covered included puberty, reproduction, contraception, and negotiation in relationships, including training in assertiveness skills. The emphasis on avoidance of risks came not from instruction but from "empowered" personal choice gained through involving students in role plays and group work. In order to ensure that accurate information about medical issues is giving to the participants, a medical doctor was co-opted as a research assistant. Participants in the control group were involved in the pre-treatment meetings, assignment into groups and response to the pre-test and post-test questionnaire forms but there was no treatment for them. Data Analysis The data obtained for this study were analysed to determine the effects of the independent variable (Sex Education Programme) on the dependent variable (reduction in at-risk sexual behaviour). The Analysis of Covariance (ANCOVA), using the pre-treatment test scores as covariates was employed for the data analysis. Results In this section, the results of the data analysis for this study were presented. The results were presented according to the hypothesis that guided the study. Hypothesis 1: It states that there is no significant difference in the at-risk sexual behaviour of school-going adolescents exposed to treatment and those in the control group. In testing this hypothesis, three statistical analyses were carried out. The results were presented in Tables 2 and 4 The tabular details represented in Tables 2, 3, 4 showed the unadjusted and adjusted means of the two experimental groups. Significant differences can be observed between the x-means and the y-means of the treatment group while no such differences were recorded for the control group (Table 2). From this observation of pre-test and post-test means, it can be deduced that the Sex Education Programmme had a substantial impact in reducing the at-risk sexual behaviour of the adolescents their gender notwithstanding. The Analysis of Covariance that followed threw more light on the level of significant difference between the experimental groups. The result in Table 3 showed that a significant difference existed between the scores of participants who were exposed to the treatment package and those in the control group (F=95.93; df 1/20, p<.05). Thus the treatment (rows) was found to be significant while no interaction effect was observed between row (treatment) and columns (gender). This implies that male and female school-going adolescents benefited from the programme. Further insight into the hypothesis was provided by the results displayed in Table 4. Based on Tables 2 and 3, the null hypothesis which stated that there is no significant difference in the at-risk sexual behaviour of school-going adolescents exposed to treatment and those in the control was rejected. The comparison of the cells (Table 4) confirms the result as the hypothesis was rejected in 4 out of the 6 cells. The only area where no significant difference was recorded was between male and female participants exposed to the same experimental condition. Discussion The main purpose of this study was to investigate the effect of sex education programme on at-risk sexual behaviour of school-going adolescents in Nigeria. When the treatment (intervention) group was compared with the control group in an intention to treat analysis (see Tables 1, 2, 3, 4), there were significant differences in at-risk sexual behaviours of the two groups. Those in the intervention group reported less at-risk sexual behaviours than their counterparts in the control group. Lack of behavioural effect on the control group could be linked to differential quality of delivery of intervention. The present findings have corroborated such studies as Wight, Raab, Henderson, Abraham, Buston, Hart, & Scott 35 which tried to determine whether a theoretically based sex education programme for adolescents delivered by teachers reduced unsafe sexual intercourse compared with control programme. Participants were 8430 pupils aged 13 15 years. When the intervention group was compared with control group, pupils evaluated the intervention programme more positively and their knowledge of sexual health improved. The present findings also lend credence to the research findings of Kelly, et al. (36) whose peer-based interventions were found to be effective in reducing sexual risk-taking behaviour among adolescents. Within a broad-based sex education programme, the researcher detected changes in attitude, increases in sexuality knowledge and a relative decrease in at-risk sexual activity compared to the control group. The attitude changes included a decrease in adolescent's beliefs that multiple sex partners are not hazardous to health. The researcher considers this an indication of increased knowledge about at-risk sexual behaviours, one main objective of the programme. An examination of literature and a programme review37 suggested that applying principles of social learning in sex education (so that students learn, do role play, and observe their effectiveness in controlling relationships) rather than more traditional educational methods of didactic teaching, were more likely to be associated with behavioural change The researcher found that the level of adolescents' understanding of human sexuality limited their ability to make informed decisions. For instance almost half of the adolescents (49%) thought that the middle of the menstrual cycle equated with the "safe period". To this end, the researcher continued to include a considerable factual content in this programme but delivered the information by using group work and group discussion. Having a doctor present in the lessons helped in giving accurate information about medical issues but the researcher controlled the process of delivery. Conclusion Compared with the control group, this specially designed intervention sex education programme, reduced at-risk sexual behaviours in adolescents. Based on this finding, it was recommended that sex education be introduced into the curriculum of secondary school education in Nigeria. Sex and relationships education should not be regarded as a negative process that attempts to frighten teenagers away from a powerful biological drive. Whatever the effective components of sex education are, the positive aspects of sexual and intimate relationships should not be forgotten. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08026t4.jpg] [hs08026t2.jpg] [hs08026t1.jpg] [hs08026t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}