 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 126-132 Practice Points Breast cancer guidelines for Uganda (2nd Edition 2008) A.Gakwaya1, M.Galukande1, *, A.Luwaga3, J.Jombwe1, J.Fualal1, E.Kiguli-Malwadde2, P.Baguma2, A. Kanyike3 , J.B Kigula-Mugamba3 1Department of Surgery, Mulago Hospital, Kampala, Uganda, 2Department of Radiology, Mulago Hospital, Kampala,
Uganda, 3Department of Radiotherapy, Mulago Hospital, Kampala. Uganda Code Number: hs08027 Clinical specialties: General surgery, oncology, radiation oncology, internal medicine, palliation medicine, obstetrics and gynaeclology, family practice, radiologist, pathologist. Intended users: Doctors, nurses, clinical officers, allied health personnel, students, and patients. Introduction Breast cancer in Uganda is the third commonest cancer in women coming only next to cancer of the cervix and Kaposi's sarcoma. The incidence of breast cancer in Uganda has doubled from11: 100,000 in 1961 to 22:100,000 in 19951,2,. Many patients are often seen in late stages thus the outcome of treatment is mostly unsatisfactory. The present day knowledge of this disease does not have any effective primary prevention. It is thus imperative that efforts should be made to detect the disease in its early stages. Mammography has been found to be useful but it is not feasible for mass screening in Uganda, as there is a limited number of units accessible to the general public. Public education towards Breast Self Examination (BSE) should be propagated because it is practical and affordable 3. These guidelines were compiled by the Uganda Breast Cancer working group whose objectives are to improve the quality of life of the breast cancer patients and their families by working towards encouraging early detection; harmonize treatment, referral of patients and to create a reference document for health workers dealing with breast cancer. In addition it aims at creating awareness about breast cancer to health workers and the community and to be part of the National Cancer Society creating a breast cancer registry and cancer control program. This edition is an updated version of the one published in 20034. This version highlights the importance of Breast Self Examination (BSE), which is still practical and affordable though it is discouraged in other resource rich settings. It includes a section on pathological specimen reporting in an effort to information sharing and therefore decision making. It includes a section on prognostication. It presents a relaxed view on and recommends Breast conserving surgery a different stand from the previous edition and lastly it presents a one-page reader friendly, at a glance overview of Breast cancer treatment for easy reference by the user. Objectives of these guidelines:
Methods: This is a consensus document, a result of a team of mostly Uganda experts reviewing the past guidelines, incorporating new ideas accruing from accumulated experience through a multidisciplinary clinic that runs weekly over a seven year period dealing with Ugandans Cancer patients. Breast self- examination (BSE) detection of breast cancer 5,6, The woman stands in front of a mirror, puts up her arms and observes her breasts; she may note wrinkling of skin, elevation of the nipple, and a mass may also be seen. Then the woman lies flat on her back, puts one hand behind her head and uses the opposite hand to palpate the opposite breast. If she notices any abnormality she should seek attention of health care provider immediately. In pre-menopausal women BSE should be done on every 10th day of the menstrual cycle. Triple assessment of symptomatic cases This is essential before treatment is undertaken and includes clinical evaluation, breast imaging and histopathological examination, it is done for any patient suspected to have breast cancer. i. Clinical assessment: History of a mostly painless breast mass, nipple discharge especially if from one duct, nipple or skin retraction, axillary mass, arm swelling, hair loss and development of other symptoms with reference to possible metastatic disease. A past medical history of breast disease and family history of breast cancer should be sought. The reproductive history is also important. This should include age at menarche, menstrual history, age at first pregnancy, and age at on set of menopause, number of pregnancies and abortions, breast-feeding duration and history of contraceptive pill use. Physical examination should include weight, height and surface area (BMI). The local examination should be done with the patient both in sitting and in supine positions. One should look for breast masses, skin and nipple changes, axillary and supraclavicular lymph nodes as well as arm swelling. ii. Breast imaging: Patients are divided into 3 categories:
Imaging procedures offered include: mammography, breast ultrasound, galactography and pnuemocystography. Mammography is the imaging technique of first choice in symptomatic patients. The ages at which mammography should be done were adopted depending on our clinical experience and may be reviewed. Mammography is done for the symptomatic group for those over 25 years, and testing is done for those over 30 years. The BISM system of reporting a mammogram is recommended. Normal -1. Benign lesion- 2. Indeterminate- 3. Suspicious- 4. Malignant- 5. iii. Pathological examination: · Fine needle aspiration cytology Biopsy has a high degree of accuracy 7,8 and with minimal discomfort9 when malignant cells are noted and definitive surgery may go ahead based on this provided the results are in agreement with the clinical and/or mammography assessment. For impalpable lesions, ultrasound or mammography guided fine needle aspiration (FNA) is advocated.
Staging Staging investigations include bilateral mammography to exclude multifocal or bilateral disease, breast ultrasound for accurate tumor size assessment and other tests. Full blood count, urea & electrolytes, liver function tests and baseline chest X-ray. The routine uses of liver ultrasound, skeletal survey and skeletal scintigraphy in asymptomatic women has very low yield and does not improve survival or quality of life. The TNM classification of breast cancer is recommended10, 11. Treatment Like in all cancers the diagnosis of breast cancer is frightening and exposes the patient and her family to psychosocial trauma. Adequate counseling, pain and other symptom control should be part and parcel of the entire management strategy. Good counseling enables the patient and her family to cope with the stress that is part and parcel of cancer. It enables them to adjust their life styles. For example if she was the breadwinner some one else may have to take up that role as she undergoes treatment. Counseling should continue during treatment and follow up. Management of early breast cancer Ductal carcinoma-in-situ (DCIS) We recommend wide excision (Breast Conserving Surgery) and adjuvant radiotherapy as effective methods of treating DCIS 12, 13, 14 unless in presence of multicentric tumors in more than one quadrant, or diffuse malignant looking micro calcifications through out the breast15. The other relative contraindication to breast conserving surgery is pregnancy, previous radiotherapy to breast area and collagen vascular disease of BCS is not possible or feasible a mastectomy is done. Mammography detected ductal CIS or palpable ductal CIS with no multicentric or diffuse micro calcifications qualifies for breast conserving surgery and axillary dissection 16,17 The likelihood of axillary involvement in DCIS is about 2-3% and axillary dissection is therefore not recommended 12, 16, 17. Role of sentinel mode biopsy is unresolved in literature and not yet available in Uganda. Routine use of tumor matters, imaging for metastases and LFT tests in DCIS is not useful and discouraged 18. Post operative Clinical reviews We recommend 3-6 monthly follow up for first year then annually for life, unless concerns or complications arise17. Postoperative mammography may be done after 1 year when surgery and postoperative treatment changes resolve after that 2 yearly if possible Lobular carcinoma in situ (LCIS) Lobular carcinoma in situ is generally considered a pre cancerous condition. It is lobular because the cancer is confined to the lobules (the glands that secrete milk). Lobular carcinoma is situ is an unusual histological pattern of non-invasive neoplastic disease of the breast 18. Lobular carcinoma in situ is frequently multicentric and bilateral and there is evidence that it is associated with an elevated familial risk of breast cancer 19. We offer a wide excision and give tamoxifen for a 2 to 5 year period. Prophylactic mastectomy is an option. Paget's disease 20,21 Paget's disease of the breast is a rare malignancy of the nipple-areola complex22, 23; it is manifested by progressive eczematoid changes of the areola with persistent soreness or itching 24. It is mostly associated with at underlying ductal carcinoma in-situ or invasive carcinoma even when there is no palpable mass or mammography findings 25,26. Simple mastectomy and adjuvant radiotherapy are given as well as tamoxifen. If breast-conserving therapy is a choice it must be carefully indicated24. Invasive breast cancer Surgery Surgery with or without radiotherapy remains the mainstay of treatment for early breast cancer. Surgical treatment may consist of tumor excision with surrounding margins or mastectomy (removal of the entire breast tissue and the fascia overlying pectoralis major muscle). Breast conserving surgery should be followed by radiotherapy as it has been shown that local recurrence is minimized 12,14. T1NoMo and T2NoMo tumors (T< 3cm) may be considered for breast conserving surgery plus radiotherapy. The tumor-free margin should not be less than 10mm at surgery. If the tumors are central, breast-conserving surgery could be done if other factors allow like tumor breast size ratio. Patients should have mastectomy if these cancers are multifocal or central or larger than 3 cm 16,17. The mastectomy incision should be short and transverse to ease execution of radiotherapy. Physiotherapy of the ipsi-lateral shoulder joint should start on the first postoperative day to ease radiotherapy planning. Adjuvant radiotherapy A number of patients may fail to get radiotherapy because of socio-economic constraints and the long distances they may have to travel. However, health workers throughout the county should know that most of the patients would need radiotherapy after surgery. Adjuvant radiotherapy is required to reduce the risk of local recurrence 18,25. There is evidence it improves survival 26. In circumstances where the clinical and histopathological information is not sufficient we recommended that radiotherapy to the chest wall and supra-clavicular region be given in all patients that have had mastectomy. To reduce the risk of shoulder joint fixation and arm oedema, the axilla should not be irradiated in patients that have had proper axillary clearance, With proper planning, radiotherapy to the chest wall should avoid irradiating the heart and more than 3 cm of lung tissue. Adjuvant radiotherapy is also indicated in localized non-invasive breast cancer where wide local excision has been done. Adjuvant radiotherapy to the chest wall following mastectomy with axillary clearance is given in many centers when the primary tumour is more than 5cm or is T4, or when the surgical margins are unclear, or if four or more axillary lymph nodes have tumour in them. Adjuvant systemic therapy Adjuvant systemic treatment is recommended in almost all patients in Uganda except ductal carcinoma in situ, lobular carcinoma in-situ, Paget's disease and patients for which it may be contraindicated for medical reasons. All patients with lobular carcinoma in situ should have tamoxifen after wide local excision or mastectomy. Cytotoxic chemotherapy and hormonal therapy are recommended in all other patients. The chemotherapy should start immediately after surgery and be augmented by radiotherapy. Neoadjuvant chemotherapy can be given to down- stage the tumour before local treatment (radiotherapy or surgery) can be offered. The dose of tamoxifen is 20 mg once daily for as long as 2 - 5 years. Active drugs include: methotrexate, 5-fluoro-uracil, anthracycline antibiotics and cyclophosphamide. Adjuvant therapy with tamoxifen, cytotoxic drugs and ovarian suppression all reduce the risk of recurrence, risk of cancer in the other breast and death in women under 50 years of age, with node positive and node negative breast cancers. Tamoxifen alone reduces recurrence and improves overall survival in all age groups. Elderly patients and those patients in poor performance status should ideally not be given cytotoxic chemotherapy, but they may benefit from hormonal treatment. Tamoxifen is withheld while patients are receiving tamoxifen. Follow up after treatment for early breast cancer The aim of follow-up is to detect recurrence at an early stage, and thus improve chances of salvage treatment, to screen for a new primary in the opposite breast, to detect and manage treatment related toxicity, and to provide psychological support. It is recommended that palliative care team such as Hospice Uganda get involved with breast cancer patients as early as possible. Hospice is able to offer psychosocial support, drugs for pain and other symptom control. It is also recommended that more health workers (doctors and nurses) be trained in palliative care delivery to be able to offer the necessary support quite early during the patient's illness. Patients who have had mastectomy should have mammography of the opposite breast every 2 years. For those that have had breast-conserving surgery, mammography of both breasts should be done every year. The incidence of local recurrence in a conserved breast is 10- 15% in Europe. Patients should be seen at 3 and 6 months following radiotherapy and then once every year for life or at any time that they develop symptoms. Special groups or circumstances:
After 32 weeks, induced delivery followed by conventional treatment is recommended. Prognostic factors and Pathology reporting It is clear that most important prognostic factors in breast cancer remain the traditional histopathological features of tumor size, lymph node stage and histological grade. 30, 31, 32, 33 Standardized Pathology reports to include the following information: Gross description
Diagnosis
Comments
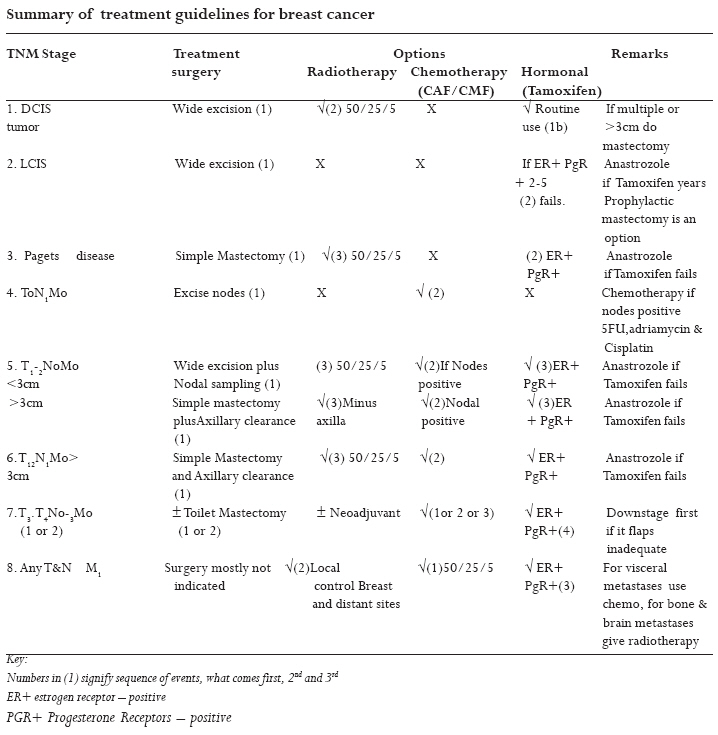
Summary of treatment guidelines for breast cancer
Recent Advances: Trails for use of Anastrozole instead of Tamoxifen, Molecularly targeted therapies e.g. HER 1 Inhibition – gefitnib, Lapatinib, HER 2 Inhibition–trastuzumab and Anti-angiogenic agents – bercizumab and taxanes for metastatic disease. Conclusion This guidelines document is a consensus document a result of work by a team of mostly Ugandan experts with hands on experience over the past seven years involved in the management of Breast Cancer patients. The first edition published in 2003 was deemed to be useful to the target audience; it has been referred to by students in training among others and cited in other publications. This updated version is enriched to capture changing view and much easier to reference. This shared work underpins our continued commitment to do the best we can with what we have for the good of our patients in a resource-limited environment like Uganda. Uganda Cancer Working Group:
References:
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08027t1.jpg] |
| |||||||||

{kind=link}