 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 2, June, 2008, pp. 133-134 CASE REPORT Is it safe to switch from stavudine to zidovudine after developing symptomatic hyperlactatemia? Barbara Castelnuovo1, Agnes Nanyonjo1, Moses Kamya2, and Ponsiano Ocama2. 1Infectious Diseases Institute. Kampala, Uganda, 2Makerere
University, Kampala, Uganda. Code Number: hs08028 Introduction: In resource limited settings patients on antiretroviral treatment who develop stavudine induced hyperlactatemia
are often switched to zidovudine on the basis of published
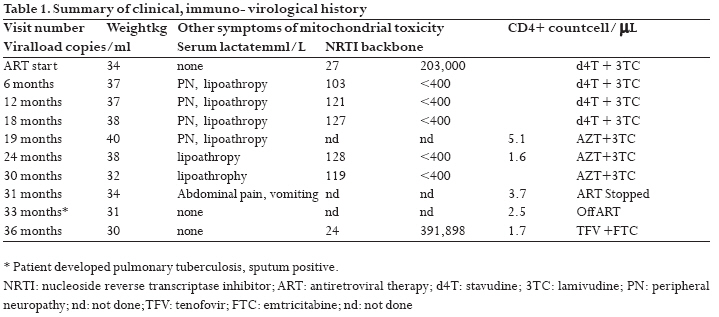
studies that demonstrate that this agent can be a safe alternative. Introduction: The prognosis of Ugandan patients with HIV infection has improved with increased access to free antiretroviral therapy (ART). The first-line combination therapy recommended by the National Guidelines includes zidovudine or stavudine plus lamivudine, in combination with either nevirapine or efavirenz 1. Stavudine 2-4 and to a much lesser extent zidovudine 5 use is associated with type B lactic acidosis (without hypoxemia). Because most of patients are started on stavudine containing regimens, this rare, but potentially fatal syndrome has become of great concern in resource limited settings (RLS) 6-7. Both diagnosis and management of this condition are difficult, leading to high mortality among patients (7- 21%) 6, 7. The treatment of lactic acidosis/symptomatic hyperlactatemia is supportive (intravenous fluids, mechanical ventilation, and dialysis) and presumed causative drugs should be discontinued and substituted with a nucleoside reverse transcriptase inhibitors (NRTI) less likely to cause this syndrome such as tenofovir and abacavir. However these agents are expensive and often not available in RLS. Therefore patients who develop stavudine induced hyperlactatemia are often switched to zidovudine on the basis of published studies 8, 9 that demonstrate that this agent can be a safe alternative.Recently however, we observed a case of relapse of symptomatic hyperlactatemia in a patient that was switched from stavudine to zidovudine. Case history A 60 year old female was started on free fixed dose combination of stavudine (30 mg) plus lamivudine plus nevirapine at the Infectious Diseases Institute, Mulago Hospital, Kampala, Uganda. The clinical, immuno-virological and treatment history is summarized in table 1. The baseline weight, CD4+ count and viral load were 38 kg, 27 cells/mL, and 202,000 copies/ml respectively. By month 6 on ART she developed features of lipoatrophy and complained of mild peripheral neuropathy. Nineteen months after starting on ART she started complaining of severe abdominal pain associated with vomiting. The clinician that assessed the patient suspected symptomatic hyperlactatemia and referred her for laboratory testing. Serum lactate was found to be 5.2 mmol/L (normal range 0.5-2.2 mmol/L) and the elevation was attributed to stavudine use. The patient was switched from stavudine to zidovudine without waiting for lactate levels to revert to normal. The lactate levels were constantly monitored and 5 months after the switch they had normalized (1.6 mmol/L). Ten months after the switch to zidovudine the patient presented with anorexia, vomiting, and 4 kg weight loss. A number of laboratory testing were done and these showed a CD4+ count of 129 cell/mL, viral load of < 400 copies/ml and serum lactate of 3.7 mmol/L; other common causes of hyperlactatemia such as malaria, sepsis, diabetes, liver/renal failure, excessive exercise, dehydration, were excluded. An ultrasound was performed and didn't show any liver abnormalities. Antiretroviral therapy was discontinued and she could not be switched to another combination for lack of tenofovir or abacavir in the free treatment program she was enrolled in. Two months after the interruption the patient deteriorated clinically, experienced weight loss, night fevers and persistent cough. Ziel- Nielsen (ZN) stain on sputum was positive and she was started on anti-tuberculosis drugs. At her last clinic visit her CD4+ count and viral load were 24 cell/mL and 391,898 copies/ml respectively; the patients was started on tenoforvir plus emtricitabine plus efavirenz since the Infectious Diseases Institute has agreed to pay for tenofovir after this case was presented in a weekly meeting where clinicians discuss and agree on the management of difficult and complicated cases. Discussion Lactic acidosis is classified into two categories: in type A lactic acidosis occurs in the setting of poor tissue perfusion or oxygenation while in type B lactic acidosis there is no clinical evidence of poor tissue perfusion and the high lactate levels are due to delayed clearance, accelerated aerobic glycolysis or biochemical alterations (dysfunction of the pyruvate dehydrogenase or oxidative phosphorylation). NRTI antiretroviral drugs can cause an increase in lactate levels interfering with the oxidative phosphorylation through the inhibition of the DNA polymerase γ and therefore depletion of mitochondrial DNA. Hyperlactatemia associated with zidovudine use is exceptional but has already been described in developed countries5. In those settings patients that develop lactic acidosis/symptomatic hyperlactatemia are switched to safe drugs such as tenofovir or abacavir. Bolhaar et al 7 concluded in their article that the substitution of stavudine with zidovudine could be safe. However the period of observation was relatively short; moreover this substitution could pose challenges in RLS where serum lactate testing is seldom available. This case shows that switching to zidovudine potentially can lead to a hyperlactatemia relapse. In the context of free antiretroviral treatment programs, the majority of patients are started on stavudine containing regimens but alternative drugs, such as abacavir and tenofovir are often not provided as well as lactate measurement facilities. Therefore we recommend close follow up for patients that are switched from stavudine to zidovudine and, in case lactate measurement is not possible, free programs should provide safer drugs such as abacavir and tenofovir for patients that develop hyperlactatemia. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08028t1.jpg] |
| |||||||||

{kind=link}