 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 3, Sept, 2008, pp. 136-141 Post traumatic stress disorder among former child soldiers attending a rehabilitative service and primary school education in northern Uganda. Emilio Ovuga1, Thomas O. Oyok2, E.B. Moro3 1 Faculty of Medicine, Gulu University, P.O. Box 166, Gulu, 2 Gulu Regional Referral Hospital, P.O. Box 160, 3 Gulu, Faculty
of Medicine & Hoima Regional Referral Hospital, P.O. Box 5, Hoima Code Number: hs08030 Abstract Background: This study was prompted by the psychiatric hospitalization of 12 former child soldiers of the Lord's Resistance
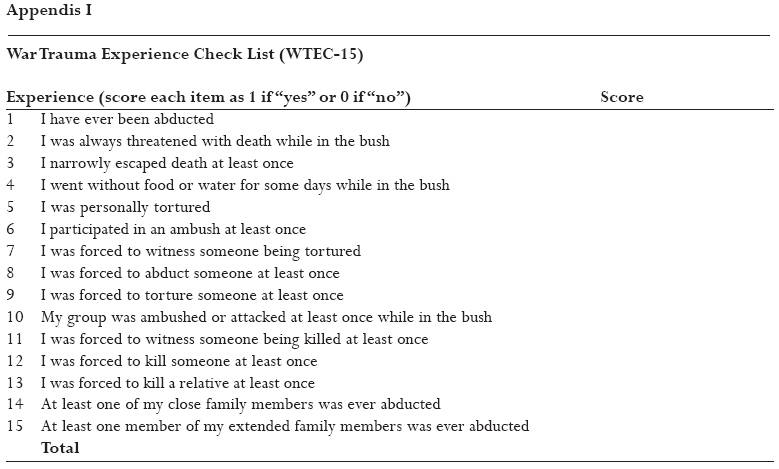
Army (LRA) at a rehabilitation school in northern Uganda with a case of mass psychotic behavior. Introduction Reports from schools and communities in northern Uganda about former child soldiers of the Lord's Resistance Army (LRA) suggest that these children suffer from varying degree of symptoms of post-traumatic stress disorder (PTSD). A number of articles on post-traumatic stress disorder among different population groups exposed to violence and war have been published1-3. However no article on the existence of post-traumatic stress disorder on a large scale among school children has been reported. Research in Uganda has indicated that more people in war-affected Adjumani district in northwestern Uganda than those in relatively peaceful Bugiri district in southeastern Uganda were suicidal4 and depressed5. Derluyn et al6 have reported that 19% of the rebel child soldiers who quit the war in northern Uganda suffered from severe post-traumatic stress disorder. Recently Roberts and colleagues7 have reported high levels of mental health problems among adults in camps for internally displaced persons (IDP) in northern Uganda. In this paper we report a clinical study of 102 primary school children aged 6-18 years at a rehabilitation primary school in northern Uganda, following the hospitalization of 12 of them to the psychiatric ward at Gulu Regional Referral Hospital (GRRH) in November 2006 with what appeared to be mass psychotic behavior. MethodsThe setting: Participants came from an ultra-modern boarding primary school established in July 2006 to rehabilitate and prepare former child soldiers of the Lord's Resistance Army (LRA) for community life and or to join the formal education system. Situated 4 kilometers from Gulu town center, the school was designed to provide "accelerated learning" to its inmates. Children who were abducted when they had been to primary school for at least three years were to study at the school for one year in order to be promoted straight to standard 6 of the Ugandan formal seven-year primary education system. Children who were abducted while in primary 2 were being prepared to join primary 6 after a two-year instruction at the school, and those who had never been to school were to study at the school for three years in order to be promoted to standard six for eventual preparation for primary leaving examinations in primary seven. However children aged 16 years or older receive vocational training instead. The academic environment at the school is thus quite stressing if not demanding in nature. The boarding school housed 673 children at the time of this study. Out of these were 14 pregnant girls, 46 child mothers, and 26 who had various war-related physical disabilities. The youngest child was aged 3 years, born in captivity, and the oldest, 18. Neither the youngest child, the child mothers nor pregnant girls was identified with any form of mental health or surgical problem prior to or at the time of the study. During recess children sat idly by in small groups, mainly according to sex and age groups. A keen observation quickly revealed the militaristic behavior of some of the children as they moved about the compound, quite akin to the atmosphere in rebel captivity. There was no contact between the children and the community surrounding the school. The children instead were referred to as olum olum (bush man or bush woman), a description that was particularly upsetting to the older children. The order and close clustering among the children vividly reminded them of their days in rebel captivity, a situation that enhanced the re-experience of flashbacks and reminders of their life in the bush, including horrifying nightmares and occasional dangerous physical assaults on one another or even staff at the school. For instance on seeing a school mate lying asleep in the compound, one child remarked: `The neck of this one is in perfect position for cutting with a machete'. A typical day at the school consisted of an orderly routine of early morning prayers, cleaning, breakfast, classes, meals, games, and evening prayers before bedtime. The mass psychotic behavior that prompted this study followed one of the routine evening prayer sessions that went out of control and ended up in what the School Administration referred to as demonic possession (cen). Participants The primary sample comprised of 12 children who had been hospitalized at Gulu Regional Referral Hospital in November 2006. Of this sample, 11 were girls and 1 was a boy (the primary patient) aged 16 years. A visit to the school as part of the crisis intervention procedure revealed 14 others who had been "possessed by demons" and were awaiting the arrival of a church minister from the capital city, Kampala, over 330 kilometers away. For each of the 26 demon-possessed children at least one control of the same sex age and class at school was randomly recruited with the help of the Head Teacher resulting in the recruitment of 30 controls. Following satisfactory outcome of intervention the school identified 22 additional children with various degrees of war-related physical injuries for assessment for possible surgical intervention. Thereafter 24 more children with behavioral symptoms were selected by the administration for mental health intervention, bringing the total number of children to 102. Data collection instruments All children including those who were "possessed" or had behavioral symptoms but were not hospitalized, and those with physical injuries were assessed using three different survey instruments as follows. Socio-demographic tool designed for the purpose was used to elicit information on each child's sex, age, history of abduction, educational attainment, current residence, parental health, parents' occupation, and family history of common mental health problems. Data to determine the extent of each child's experiences with war events in northern Uganda was collected using a 15-item War Trauma Experience Check-list (WETC-15) instrument, which was constructed based on the most severe forms of war related traumatic experiences and activities that former rebel abductees previously reported upon their return from the bush. (See appendix I). Further data was collected using the 16-item Harvard Trauma Questionnaire (HTQ-16) 8 designed to screen for post-traumatic stress disorder, and the Hopkins Symptom Check-List for Depression (HSCL-15) 9, 10.The HSCL 11 is a 15-item instrument that has previously been used to screen for depression in several settings elsewhere; the item on libido was removed as it did not apply to most of the children. All instruments were translated into luo, the native language spoken in the area and pre-tested before the start of the study. Calculation of scores on the HTQ-16 and the HSCL was carried out using published guidelines for these instruments. Scores on the WTEC-15 was arbitrarily dichotomized into two categories; those who experienced up to 9 severe traumatic events and those who experienced 10-15 such events. Data collection procedure All interviews were conducted in luo by a psychiatrist (TO) who was assisted by a clinical officer in mental health supervised by the principal author (EO). Both interviewers came from the Acholi ethnic group. The children with physical injuries were examined by a senior consultant surgeon (EBM). Radiological evaluation was made on each of the children with physical disabilities. ResultsParticipants: The total number of girls in the study was 58 and there were 44 boys, aged between 6 and 18 years. The distribution of the children by sex, age, clinical status and social history are shown in table 1. Socio-demographic findings Sex: Boys were twice as likely as girls to have physical injuries sustained while in captivity while girls were more than 7 times as likely as boys to have been hospitalized or twice as likely as boys to be referred to the mental health professional (X2 = 21.6, df = 3, p = 0.000). Only one out of the 12 hospitalized children was a boy (X2 =10.6, df = 2, p = 0.005). Age: Boys were older (Mean age 14.93 years sd = 1.32) than girls (Mean age years, 13.69 sd = 2.07); (F = 3.234, t = 3.478, df = 100, p = 0.001; 95% CI = 0.534-1.951). Education level at the boarding school: Thirty one (30.4%) of the participating children were attending vocational training at the school while 71 (69.6%) were at various levels of the accelerated learning program. War-related findingsAbduction: Ninety six (94.1%) of the participants had been abducted and 6 (5.9%) were born in captivity in the course of the war in northern Uganda. Return from captivity More than 70% of the children (71.9%) escaped from their abductors within two years and only one child, the primary patient, escaped after 10 years in captivity. Fifty four participants (52.9%) returned from the bush via one of several reception centers that had been established to provide screening, debriefing, facilitation of resettlement and re-integration with the children's families and communities; there was no information about one child in relation to his/her mode of return. Cleansing ceremony Forty nine participants (48.0%) passed through some form of traditional cleansing ritual upon their return from the bush (stepping on an egg at the entrance of the home) aimed to purify the children from atrocities they might have committed while in the bush. Findings related to family background Parents' marital and health statusEighty three children (81.4%) reported their parents as married during their lifetime and 10 (9.8%) reported that their parents were separated. Sixty one mothers (59.8%) and 74 fathers (72.5%) were reported dead. Type of home Forty three children (42.2%) lived with at least one parent, 52 (51.0%) lived with relatives, 5 (4.9%) came from child-headed homes while 4 (2.0%) others lived in the camps for internally displaced persons (IDP). Family mental health Forty three children (42.2%) reported a positive family history of severe mental illness; 11 (10.8%), a family history of suicide; 23 (22.5%), a family history of suicide attempt and 46 (45.1%) reported a family history of alcohol abuse. Physical findings The children with surgical conditions had a variety of physical disabilities including (in order of frequency) foreign body in situ, chronic osteomyelitis, various forms of arthritis, paresis of the upper or lower limbs, keloids, chronic skin rashes, fracture malunion, contracture and pleurisy complicating penetrating chest injury. Test scoresWar Trauma Experience Check-list (WTECL-15) The WTEC-15 was a 15-item instrument designed to assess the number of war-related events that the children might have experienced in the course of captivity in the bush. The instrument comprised of the most severe forms of war-related events ranging from being abducted to being forced to kill a family member, most commonly, parents or siblings. Eighty nine (87.3%) of the children experienced 10 or more such events. In particular, 54 (52.9%) children reported having been forced to kill someone (including their own colleagues in the bush), and 17 (16.7%) reported having been forced to kill a close family member. (See appendix I). Boys reported significantly more war-related traumatic events (Mean 12.45, sd = 2.8) than girls (Mean 10.67 sd = 3.7); (F = 7.097, t = 2.66, df = 100, p = 0.009; 95% CI = 0.455-3.109). Children who returned from the bush via any reception center also reported a higher number of war-related traumatic events (Mean 12.82, sd = 1.7) than children who returned straight to their communities (Mean 10.09 sd = 3.966; (t = 4.628, F = 32.366, df = 99, p = 0.000; 95% CI = 1.570-3.926). Similarly children who passed through some form of traditional cleansing ritual reported more war-related traumatic events than children who did not pass through any form of cleansing ceremony (Mean 12.29 sd = 2.372; F = 9.165; t = 2.227; df = 99; p = 0.028; 95% CI = 0.155-2.686). The Harvard Trauma Questionnaire (HTQ)A score greater than 2.5 on the HTQ denotes probable diagnosis of post-traumatic stress disorder. In this series 57 (55.9%) children scored greater than 2.5. However mean scores on the HTQ were not significantly different between children of both sexes, or in relation to the mode of return from the bush, the performance of cleansing ritual, or family history of mental illness, suicide, attempted suicide or alcohol abuse. Hopkins Symptom Check-List (HSCL)A test score higher than 1.75 on the HSCL denotes probable diagnosis of depressed mood. Ninety (88.2%) children attained test scores greater than 1.75. Participants (aged 16 years or older) from the vocational training wing of the school attained higher HSCL scores (Mean 2.78 sd = 0.59) than children from the "accelerated learning wing" (2.45 sd = 0.68) (F = 5.510, t = 2.347, p = 0.021, 95% CI = 0.05-0.60). Scores on the HSCL for depression were not significantly different in relation to sex, family history of mental health problems, route of return from the bush or history of traditional cleansing ritual. Relationship between scores on test instruments Children with high scores on the HSCL were more likely to score 10 or higher on the WTEC-15 (X2 = 10.229, df = 1, p = 0.007). However there was no statistically significant relationship between the distribution of the children according to test scores on HSCL and HTQ, or between the children's distribution on test scores on HTQ and WTEC-15. Relationship between clinical groups on the basis of mean test scores Means scores on the WTEC-15, HSCL-14 or the HTQ-16 were not significantly different between the different clinical groups of the children; namely: demon-possessed, children with behavioral disorders, children with physical injuries or control children suggesting a uniform impact of war experiences among the children in rebel captivity in terms of depressed mood and post-traumatic stress disorder. DiscussionGeneral comment This clinical report presents the case of 102 former LRA child soldiers at an ultra-modern boarding primary rehabilitation school in northern Uganda, following the hospitalization of 12 children with what appeared to be mass psychotic disorder. The report is limited as most participants were selected by the school administration on the basis of the children's suspected possession with demons or the children suffering from various physical disabilities related to war injuries. Though it would have been beneficial to recruit at least one control for each of the 70 children with any form of health problem, this was not considered essential as it soon became clear that nearly every child suffered from some form of war-related psychological disorder, which was subsequently evidenced by 88% of the children having screened positive for depressed mood on the HSCL-14 and 57 (55.9%) of the children having screened positive for post-traumatic stress disorder. War trauma experience Overall the participating children, aged between 6 and 18 years, reported their own exposure to and participation in horrific acts of war in the bush against the background of constitutional predisposition to poor mental health characterized by family history of mental illness, completed suicide, suicide attempt, alcohol abuse and the loss of significant other person in their lives. As expected boys reported more exposure to war-related traumatic events as judged by mean WTECL-15 scores (12.45 vs 10.67), were more likely to experience war-related injuries and complications though they were less likely to be hospitalized or referred to mental health professionals. It is not immediately clear whether this observation reflects the expected behavioral norm for males not to exhibit stress-related emotional reactions or succumb emotionally to combat experiences. Observation of the children at the school both during and outside interviews revealed their masked emotionless faces during their interactions with other people. Return from the bush The majority of the children returned to their communities within two years of abduction. Children who returned directly to their communities without going to any reception center reported significantly fewer war-related traumatic events than those who returned through one of several reception centers or the government's amnesty commission centers (10.09 vs 12.83). Similarly children who did not go through any form of traditional cleansing ritual reported fewer traumatic events (10.87 vs 12.29). These results are difficult to explain. It is possible that the children who committed more atrocities in their communities feared for their safety and were more likely to seek the initial protection of available reception centers and the services of the government's Amnesty Commission whose task was to receive, pardon and resettle former LRA rebels and child abductees in their communities. As expected, children who experienced 10 or more war related traumatic events also scored higher on the HSCL-14 than children who experienced 9 or fewer such events (mean 12.89 vs 10.09). These results are in line with previous reports indicating a dose-effect relationship between the extent/severity of exposure to traumatic events and scores on HSCL 12. Many of the children reported the death of either a mother (64%) or a father (74%) with others living in child-headed homes (4.9%) or with relatives other than biological parent (51%). Although the social support system in northern Uganda is rich, the circumstances of the children and their communities overstretched the capacity of any existing social support network; the burden of war trauma experience in the children's communities would be expected to predispose them to severe psychological distress. This situation is aggravated by the `accelerated' education system and policy at the school requiring children with a minimum prior educational level of three years to study at the school for only one additional year after their return from the bush in order to proceed to standard six. Although the concept of `accelerated' education was meant to enable older children to catch up with their age-mates within the primary and secondary education systems, this arrangement placed many of the children under severe strain in the circumstances of limited educational resources and few teachers at the school. Children aged 16 years and older attained significantly higher scores on HSCL than those from the `accelerated learning' wing (mean score 2.78 vs 2.45) for obvious reasons; such children missed the opportunity for further education and were thus condemned to a limited educational attainment, future poverty and poor mental health, a situation that understandably aggravated their emotional situation. Implications This clinical study, which was prompted by the admission to a psychiatric ward in northern Uganda, highlights the urgent need to screen for post-traumatic stress disorder and depression among former child soldiers of the LRA and the need to provide psychological support to those at risk for any form of psychological distress within the school environment. A proportion of the children have physical disabilities arising from their involvement in combat operations and these need surgical intervention. The needs of the children at the school stretch far beyond the provision of education and vocational training to their future reintegration in their communities. Comprehensive psychosocial rehabilitation including psychological therapy should therefore form the basis of resettlement, reintegration and the return of former children from LRA-captivity to normalcy. Reference:
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08030t1.jpg] [hs08030a1.jpg] |
| |||||||||

{kind=link}
{kind=link}