 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 3, Sept, 2008, pp. 160-162 Hydrocelectomy under local anaesthesia in a Nigerian adult population Agbakwuru EA, Salako AA, Olajide AO, Takure AO, *Eziyi AK 1 Department of Surgery, Obafemi Awolowo University Teaching Hospital, Ile Ife, Osun State. Nigeria. Code Nmber: hs08034 Abstract Background : Hydrocele is abnormal collection of serous fluid in the tunica vaginalis or a patent processus vaginalis. It is
commonly encountered in our practice and often requires surgical treatment. However in our setting and in many underdeveloped
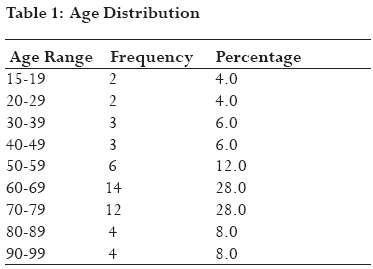
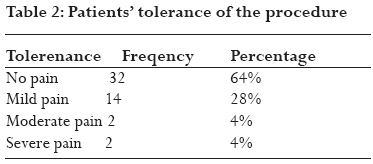
countries, availability of general anaesthetic service is poor due to lack of trained personnel and equipment. Key words: Hydrocele, hydrocelectomy, local anaesthesia,sedation Introduction Hydrocele is a collection of serous fluid in the tunica vaginalis or a patent processus vaginalis. It may arise in the spermatic cord in the males or canal of Nuck in the females.1,2 Hydrocele is idiopathic in most cases but in some cases may be secondary to various pathologies like infections (orchitis, epididymitis, tuberculosis or filariasis), testicular torsion, tumour or trauma.3,4 The diagnosis is essentially clinical, but where doubt exists, scrotal ultrasound can be used to differentiate it from other scrotal lesions5,6.Controversies exists about the treatment of hydrocele; aspiration of the fluid and injection of sclerosants has been described, this is however associated with high rate of infection and recurrence4,5.Some workers have described the use of di-ethylcarbamazine in the treatment of hydrocele due to filariasis.7,8 However, hydrocelectomy remains the treatment of choice for the management of hydroceles.4,9,10 Hydrocelectomy can be done under general or local anaesthesia using either bupivacaine or lignocaine11,12,13. The advantages of this method include cost reduction, alleviation of the risks associated with general anaesthesia and suitability for patients who have co-morbid medical conditions or are afraid of general anaesthesia.Consideration of safety and cost-effectiveness by many of our patients also argue strongly for performance of most hydrocele repairs as outpatient procedures under local anesthesia.13 In this study, we assess the practicability of hydrocelectomy as a day-case procedure under local anaesthesia using spermatic cord block and intramuscular diazepam sedation and evaluate the acceptability of this procedure in Nigerian adult patients with hydrocele. Patients and methods Fifty consecutive adult patients, age above fifteen years, with diagnosis of hydrocele,small and moderate sized, excluding giant hydroceles(big as the patients head) underwent hydrocelectomy as day case procedure with local anaesthesia using spermatic cord block and scrotal skin infiltration with local anaesthetic,0.5% plane lignocaine and intramuscular diazepam sedation. Intramuscular diazepam 10mg was given 30mins before commencement of the surgery. Thereafter spermatic cord block was done by the assistant holding the spermatic cord gently between the fore finger and thumb both at the inguino-scrotal junction and just above the scrotum in order to stabilise the spermatic cord. 10 mls of 0.5% plane lignocaine (constituted by diluting 2% lignocaine with three times volume of normal saline) was injected around the stabilized spermatic cord at three different angles using size 23G needle, each done without completely withdrawing the needle through the skin. Before injecting, the plunger of the needle was aspirated to avoid inadvertent intravascular injection of the local anaesthetic. Thereafter, scrotal skin and subcutaneous tissue at the site of the incision were infiltrated with 5 10mls of same reconstituted lignocaine solution after a negative aspiration test.Patients with giant hydrocele were treated with general or spinal anaesthesia. Hydrocelectomy proceeded 35minutes later using either the Jaboulay's or Lord's method4,9,1O as appropriate, after ensuring satisfactory local anaesthesia by stimulating the infiltrated skin with toothed dissecting forceps. Communication was maintained with the patients throughout the period of the operation and the patients were questioned or observed for subjective symptoms of local anaesthetic complications or pain. Pain score was assessed using 4 point categorical verbal score (0=no pain, 1=mild pain, 2=moderate pain, 3=severe pain) from the time of the incision,midway and at the end of the procedure. The wounds were dressed with scrotal support and the patients were discharged 2 3hrs after the procedure. They presented for wound inspection and change of wound dressing on post operative day three and for removal of stitches on the post operative day seven. However, they were to present earlier if there was any complaint before the appointment day. Patients' satisfaction with the treatment was assessed on the post operative day seven on a scale of 1 4 (1=very satisfied, 2=satisfied, 3=dissatisfied, 4=very dissatisfied. Results Fifty consecutive adult patients were studied. The age ranged between 15 and 94 years with mean age of 62 years. Eighty percent of these patients were above 50years. (Table 1). Most of the patients presented late with 41patients (82%) presenting after 1 year of onset of the scrotal swelling.Eighty percent (80%)were unilateral with almost equal frequency of occurrence on both sides (38% left and 42% right). Bilateral disease was found in 20% of the patients. All the cases were non-communicating with vaginal hydrocele being the commonest (94%), encysted hydrocele constituting 4% and infantile hydrocele 2%(sac extended to external inguinal ring,but non communicating with peritoneal cavity). Forty (80%) of the patients had Jaboulay's procedure done while eight (16%) had Lord's procedure and two (4%) had excision of encysted hydrocele of the cord. The complications recorded are haematoma in 4 patients (8%), and wound infection in 3 patients (6%) (Table 2), all of whom were managed conservatively. All the patients had the procedure using local anaesthesia as described in the method,thirty two patients( 64% ) had no complain throughout the period of the operation, fourteen patients( 28%) had feeling of pressure or pulling sensation (mild pain), two(4%) had pain referred to the lower abdomen but could still tolerate this (moderate pain) and preferred to have the operation completed under local anaesthesia. Another two ( 4%) had severe pain which they could not tolerate and preferred conversion to general anaesthesia, both of whom were not given diazepam because they were elderly (above 80years) with poor cardio-pulmonary reserves as determined by the attending physician preoperatively (Table 2). All the patients were discharged home within 4 hrs of the procedure except the 2 cases converted to general anaesthesia that stayed on admission for 48 hrs. None of the patients had complaint serious enough to seek consultation before the appointment days and all were satisfied with the treatment on final review and all except one will prefer local anaesthesia for future surgeries because of the severe pain necessitating conversion to general anaesthesia. Discussion Forty (80%) of the patients in this series were older than 50 years with the mean age of 62 years and 22% of the patients were farmers. This is not surprising since hydrocele resulting from orchitis, epididymitis or tropical infections such as filariasis causing either excessive secretion from irritation of tunical vaginalis or reduced drainage from lymphatic obstruction occur in the adults14,15 All the patients in this study presented with painless scrotal swelling and their reasons for seeking treatment was the weight of the scrotum causing dragging sensation and the cosmetic considerations of the swelling. The majority of the patients were asymptomatic and hence presented with duration greater than a year1,2 The complications were not different from those of scrotal surgery performed under general anaesthesia and they were managed conservatively on out-patient basis. Doing this procedure under local anaesthesia reduced the cost of treatment to 50-70% of what in-patient hydrocelectomy under general anaesthesia would have been.13 The risks associated with admission and general anaesthesia in the elderly is eliminated. There is also no need for starvation post operatively and the patients have the benefit of domiciliary care with the comfort of staying with their relatives while recovering. Patients that are afraid of general anaesthesia, and who would have preferred to endure their ailment than risk general anaesthesia readily find solace in local anaesthesia. In addition a surgeon will be more comfortable with this method when the patient is an elderly with some co-morbid conditions which may increase the risk of general anaesthesia. This has made several authors to recommend local anaesthesia for many scrotal surgeries including testicular biopsy, aspiration of spermatozoa, spermatocelectomy and hydrocelectomy.6,13,16 The use of an anxiolytic agent like diazepam as pre-medication for local anaesthesia in day care procedure can reduce fear and anxiety, the pain and allow the patient to cooperate with the surgeon during surgery.16 All the patients were satisfied with the outcome of their treatment at the last review and 98% prefer local anaesthesia for subsequent procedure. Limitations In this study, all patients who consented to hydrocelectomy were included. A randomized controlled trial would have been a better design to avoid bias in the results. However,many of these patients were either afraid of general anaesthesia or had co-morbid conditions that may increase the risk of general anaesthesia Conclusion Hydrocelectomy under local anaesthesia is practicable and was tolerated and accepted by the adult patients studied. Acknowledgements We thank the consultant surgical staff of the Wesley Guild Hospital for their co-operation. We thank Mrs Funmi Ogunwo for the secretarial assistance. Reference
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08034t2.jpg] [hs08034t1.jpg] |
| |||||||||

{kind=link}
{kind=link}