 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 3, Sept, 2008, pp. 180-185 Youth of west-Cameroon are at high risk of developing IDD due to low dietary iodine and high dietary thiocyanate. Ibrahim Taga1,2,*, Valere Aime Soh Oumbe1, Robert Johns2, Mohsin Abbas Zaidi2, Jeanne Ngogang Yonkeu2, Illimar Altosaar2. 1 Clinical Biochemistry and Nutrition Unit, Biochemistry Dept, Faculty of Sciences, PO Box 24157 Dla University of
Douala, Cameroon, Code Number: hs08038 Abstract Background: Hypothyroidism in utero leading to mental retardation is highly prevalent in developing countries where
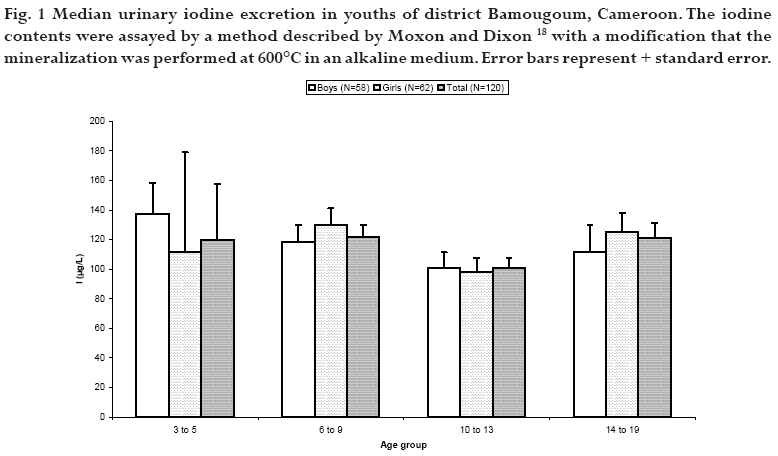
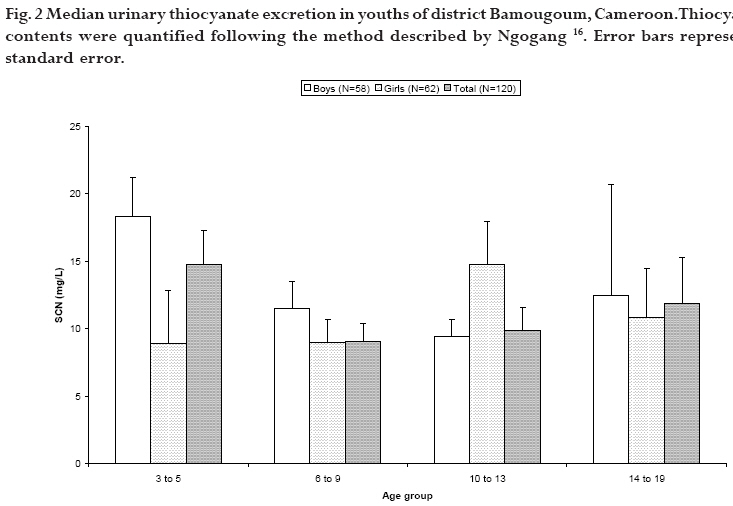
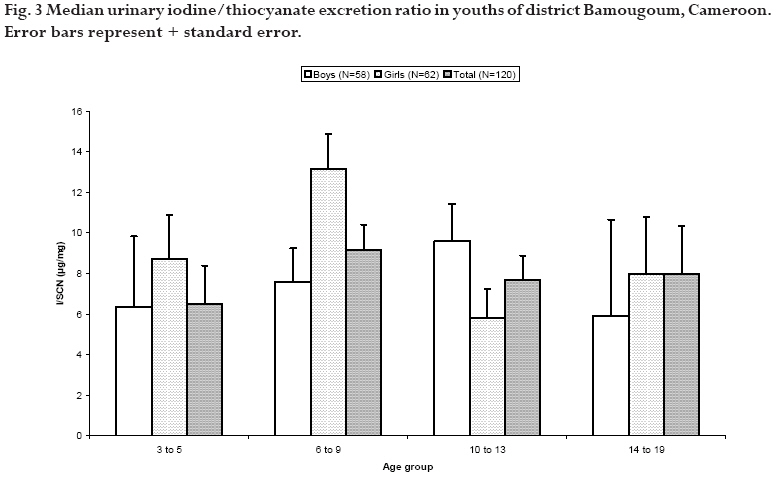
iodine deficiency and thiocyanate overload are combined. Key words: iodine deficiency, Cameroon, iodine, thiocyanate, food, urine. Running title: IDD in West Cameroon Introduction Several minerals and trace elements (iodine, iron, selenium, and zinc) are essential for normal thyroid metabolism. Deficiencies of these minerals can impair thyroid function. Iodine is most commonly known for its effect on thyroid function. Production of thyroxin (T4) by the thyroid and later generation of its active metabolite triiodothyronine (T3) relies on iodine availability. Thus, low-levels of bioavailable iodine can cause low thyroxin levels. Goiter, a classic symptom of iodine deficiency is caused by an over-stimulation of the thyroid tissues by thyroid stimulating hormone (TSH) due to insufficient T3/T4 feedback inhibition. 1 Low levels of thyroxin, especially during fetal development, cause damage collectively known as iodine deficiency disorders (IDD) such as mental retardation, brain damage, impaired physical development, spontaneous abortions, low birth weight, infant mortality, cretinism, dwarfism and endemic goiters. 2, 3, 4 More than two billion people worldwide are at risk of developing IDD due to the inadequate dietary intake of iodine either from plant or animal sources. 5, 6 The soils of the countries at high risk of IDD are often deficient in iodine. This leads to insufficient uptake of iodine by their food crops. Furthermore, they often lack access to iodine-rich sea foods, increasing the risk of IDD development. 7 Iodine is not the only micronutrient that can impact thyroid function. Thiocyanate (SCN) is believed to be a goitrogenic compound. It is a competitive inhibitor of the human thyroid sodium/iodide symporter NIS. 8, 9, 10 Thus, the adverse effects of thiocyanate overload are especially noticeable when iodine availability is low. Intake of goitrogenic substances causes an adaptive increase in T3's binding to brain nuclear receptors and in the activity of type II 5'-deiodinase, which generates T3 from T4. This altered function and availability of T3 is detrimental to the developing brain. 11 Thiocyanate is also known to modulate activity of mammalian peroxidases although the biological impact of this mechanism is unknown. 12 Cassava, grown and consumed widely in Africa, is a major source of thiocyanate. The digested cyanogenic glucosides of unprocessed cassava generate cyanides, which are metabolized to thiocyanate. 11 Unfortunately, goiter is endemic in many of the distal inland regions of Cameroon. As such, the effects of IDD remain a drain on the economic and human potential of Cameroon. Estimates suggest that IDD afflicted children may forfeit 10-15 IQ points while the World Bank suggests that up to 5% of the world economic output is sacrificed due to micronutrient deficiency like iodine deficiency. 13, 14, 15 In such a situation, it is crucial to assess the risk of developing IDD in children and youths of at least one of the distal inland regions of Cameroon using quantifiable indicators. Therefore, the present investigation was undertaken to explore the risk of IDD with the aim to prevent and to fight against them in Bamougoum, a mountain region of western Cameroon, by studying urinary iodine and thiocyanate excretion levels in children. Methods Study areaThe study was conducted from August 2002 to September 2003 in Bamougoum, a large district comprised of 9 villages located on the leeward side of the mountain chains of western central Cameroon. The study was carried out after informed consent of children's parents and approval by the University of Douala, Cameroon, for the use of human subjects. Sample collection Samples collections were undertaken during August 2002, which is a school holiday period in Cameroon, when all children are supposed to be at home. Selected subjects were visited in their homes by specially-trained nurses who obtained subjects' demographic information by questionnaire. Dried bottle of two liters, decontaminated with concentrated nitric acid and rinsed with double distilled water, was given to the child the evening before. Under the supervision of parent, each child was supposed to pass urine into a bottle every time s/he needed to void. Twenty four hours later, the bottle with urine was collected, mixed. Only 10 mL of that were aliquoted in small sterilized bottle (10 mL) containing HCl (0.5% V/V), to prevent oxidation16. The same was repeated during three consecutives days (that is Monday, Tuesday and Wednesday). Urine samples of 120 children (58 boys and 62 girls) aged 3 to 19 years were collected. All samples were stored at room temperature overnight until analysis was performed in the laboratory the next day. Although the study did not directly attempt to follow the diet and provenance of foodstuffs consumed by youth subjects, iodine levels in common foodstuffs can still be linked to subjects' urinary iodine. Quantification of thiocyanate and iodine The iodine in urine samples is released after mineralization at 600°C in an alkaline medium. Released iodine catalyzes the reduction of yellow-orange ceric ions (Ce4+) to colorless cerous ions by arsenic ions (As3+). 16, 17, 18 Potassium iodate (KIO3; 5mg/dL) was used as standard solution whereas distilled H2O was used as blank sample. Thiocyanate contained in urine was quantified colorimetrically following the method described by Ngogang. 16 In this method, thiocyanate is allowed to react with ferric ions in a neutral or slightly alkaline medium, yielding a red color. Serial dilutions of ammonium thiocyanate (NH4SCN; 50, 100, 150, 200 mM) were used as standard curves whereas distilled H2O was used as blank sample. Statistical analysis The iodine status was based on the median values obtained from urinary iodine excretion. The data were analyzed using SigmaStat (version 2.03) statistical software, student's T tests and ANOVA 2 to compare medians and to identify significant differences in iodine contents between values and groups. Statistically, difference between sex or age groups was significant for p<0.05. Urinary excretion and the estimated iodine deficient (I<50µg/L) proportion of the population were calculated in accordance with the World Health Organization's (WHO) recommendations. 19 Furthermore, median I/SCN ratios and estimated thiocyanate overloaded (I/SCN<3µg/mg) proportions were also calculated. Results The median urinary iodine excretion of the studied population is shown in Figure 1. Median iodine excretions of all groupings were approximately 100µg/L. Similarly, Figure 2 shows median excreted thiocyanate contents of collected urine samples. Median values were estimated to be 15mg/L. Statistically, no significant differences for T-test between medians of various age or sex groupings were detected. Median I/SCN ratios of the children are shown in Figure 3. Again, the medians of the groupings were approximately 9µg/mg with large standard deviations. Statistically, significant differences for T-test were detected with boys between 3-5 and 14-19, 6-9 and 14-19, and 10-13 and 14-19 age groups. Same with girls, between 3-5 and 6-9, and 3-5 and 14-19 age groups. The youths who excreted iodine levels below 50µg/L were considered as iodine deficient according to the World Health Organization's (WHO) recommendations. 19 Results from analysis of youths' urine samples are shown in Table 1. The results indicate that 22% of boys between the ages of three and five years were iodine deficient. Further, 29% of boys age six to nine years and 17% of 14 to 19 year old boys were iodine deficient. The prevalence of iodine deficiency in girls was a bit smaller compared to that in boys. Among the results, 18% of girls between the ages of three to five were iodine deficient. Sixteen percent of girls aged six to nine years were iodine deficient while 21% of 14 to 19 year old girls had urinary excreted iodine levels below 50ug/L. The data on the population with excreted thiocyanate overloaded is also presented in Table 1. I/SCN ratios below 3µg/mg were considered as indicative of thiocyanate overload, as per World Health Organization (WHO) recommendations. 19 The data indicates that 22% of three to five year old boys were thiocyanate overloaded. Twenty four percent of boys aged six to nine years were thiocyanate overloaded. Even greater, half of samples from 14 to 19 years old boys had an I/SCN ratio above 3ug/mg. Again, the girls fared slightly better than boys since the percentage of girls with thiocyanate overload was less. Twenty seven percent of samples from three to five year old girls had a thiocyanate overload. Eleven percent of girls aged six to nine years were thiocyanate overloaded. Fourteen percent of the samples from last age group of 14 to 19 year old girls had I/SCN ratio above 3ug/mg. When pooling data from both sexes, as in Table 2, the highest prevalence of iodine deficiency (23%) was found in children aged 6-9. The rest of the age groups studied had a 20% prevalence of iodine deficiency. Overall, twenty one percent of the total subject population was iodine deficient, which nears the 20% value characteristic of endemic goiter areas. Table 2 also shows the percentage of thiocyanate overloaded children. The highest prevalence of 23% of thiocyanate overload was found in children aged 3-5 and 14-19. The age groups 6-9 and 10-13 had a lower 18% prevalence of thiocyanate overload. Overall, twenty percent of the total subject population show thiocyanate overload. Discussion Iodine is an essential element that enables the thyroid gland to produce thyroid hormones. This element is ingested and absorbed in the gut almost completely in different forms. In a healthy person, 90% of ingested iodine is excreted through urine. If iodine deficiency is present, the ingested iodine will be further retained by the body reducing the levels of excreted urinary iodine. Therefore, the level of urinary iodine is used as an indicator for the assessment of IDD. The WHO defines iodine deficiency as excreted urinary iodine content below 50µg/L. Furthermore, a population is classified at risk of IDD if 20% of the population falls below the 50µg/L threshold or if the median excreted iodine content is below 100µg/L. 19 According to our study, 24% of boys had urinary iodine excretion levels lower than 50µg/L while 18% of girls were below this threshold (Table 1). When considering our whole study population, 21% of subjects had urinary iodine excretion levels lower than 50µg/L. Consequently, Bamougoum's youth should be considered at risk of IDD according to the WHO definition. 19 This can be explained by the strong consumption of staple foods that are low in iodine such as fufu maize and vegetables like black nightshade by the habitants of the Bamougoum area. Low urinary iodine excretion and low urinary ratio of I/SCN are the fundamental criteria for detection of IDD in any population. The former reflects iodine availability while the latter, the goitrogenic food consumption. It is known that a normally adequate intake of iodine may not ensure thyroid function in the presence of goitrogens. 11 In fact, intake of a goitrogen-rich diet can induce goiter even when iodine supply is sufficient. 20, 21, 22 In the present study, twenty percent of the total study population (24% for boys and 16% for girls) was suffering from thiocyanate overload. I/SCN ratios less than 3µg/mg suggest too little iodine and/or too much goitrogenic thiocyanate relative to each other. The food consumed by these children might contain goitrogenic substances such as thionamide-like compounds and thiocyanate which are known to affect thyroid function. 23 A geochemical goitrogen cannot be ruled out as a possible contributing factor. 24, 25 By applying similar WHO iodine deficiency criteria to the thiocyanate overload data, the prevalence of thiocyanate overload among the children studied suggests an endemic case throughout the general population. Table 1 shows the proportion of children in each group classified as either iodine deficient (I<50µg/) according to WHO or thiocyanate overloaded (I/SCN<3µg/mg). Except for the youngest age group (3-5 years of age), a smaller percentage of girls were classified as iodine deficient and thiocyanate overloaded compared to boys. Among the study subjects, the age distribution tended towards 6-13 year old children, especially among boys who were mostly 10-13 years old. When pooling data from both sexes, as in Table 2, the prevalence of iodine deficiency in children was more evident. In fact, this was especially true for children aged 6-9, among whom approximately 23% were iodine deficient. Roughly 21% of the total subject population was iodine deficient, which nears the 20% value characteristic of endemic goiter areas. The low I/SCN ratio can be attributed to consumption of fufu maize and cassava, which during processing, are mixed together. Cassava tubers are low in iodine especially those growing in Mountains regions as Bamougoum, where downpours wash minerals from apex of the mountain to the dregs. They also contain goitrogenic substances such as cyanogenic glycosides. 25 Thiocyanate (SCN) is a competitive inhibitor of the human thyroid sodium/iodide symporter NIS which can have adverse effects like developing IDD. Thus, a thiocyanate overload originating from consumption of poorly detoxified cassava can aggravate a mild or severe iodine deficiency. 26 Additionally, another complement of fufu maize is black nightshade, which has low iodine and high goitrogen contents. So, the existing goiter prevalence in the region could possibly be due to adequate but variable iodine supply along with an aggravating thiocyanate overload. 21, 22, 27, 28, 29,30 It is difficult to maintain a sufficient iodine intake in these villages as the individual foods are very low in this element and contain goitrogenic substances. Artificial iodine supplementation via iodized salt is one of the best strategies to ameliorate the incidence of IDD because of its efficacy. 31, 32, 33 However such an approach has proven to be far from `universal' because of inconsistent maintenance and storage throughout the edible salt chain, lack of political will, weak monitoring systems and lack of capacity for enforcing legislation in many developing countries. 34, 35, 36, 37, 38 The consumption of seaweed, which is rich in iodine, could be an easy, non-toxic way to meet dietary iodine requirements but is not readily available to those living in poorly developed areas such as Bamougoum. 39, 40 Changes in dietary habits could yield great improvements. By increasing consumption of high iodine foods such as the yam, kelen kelen or eggplant leaves would help prevent IDD. However, to successfully decrease the occurrence of IDD, SCN overload from other foods must be avoided especially among those with only adequate iodine contents. 22 It is necessary to further analyze the goitrogen contents in order to determine which goitrogen-rich foods should be avoided. As resource-poor people tend to be most at risk to IDD and tend to be limited in their dietary choices, nutritional improvement may prove difficult. Crop improvement strategies and improved soil management might be more efficacious in combating iodine deficiency and SCN overload. For example, development of low goitrogen Brassica cultivars, such as cabbage, would likely be more feasible than attempting to boost iodine levels. An effective iodine supplementation program, such as salt iodination, still holds great promise to help abate endemic goiter and IDD among the world's poor. Moreover, it is most encouraging to witness the advances being made in genetically engineered cassava for lowering cyanide content in the staple diet of these regions.41 Acknowledgments This work was funded by grants from The Rockefeller Foundation, l'Agence Universitaire de la Francophonie and the Natural Sciences and Engineering Research Council of Canada to IA. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08038f2.jpg] [hs08038t1.jpg] [hs08038f1.jpg] [hs08038t2.jpg] [hs08038f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}