 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
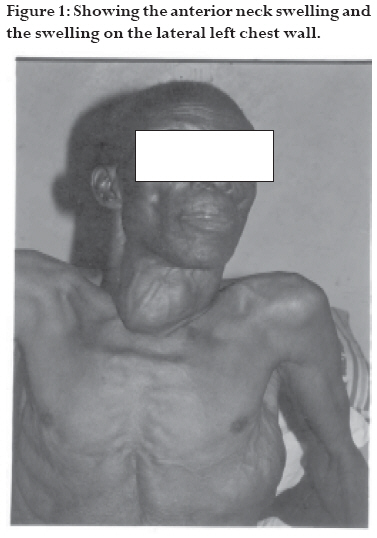
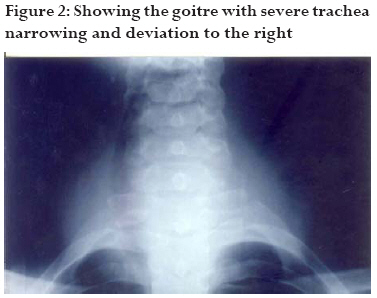
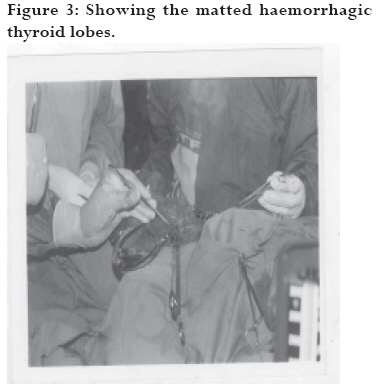
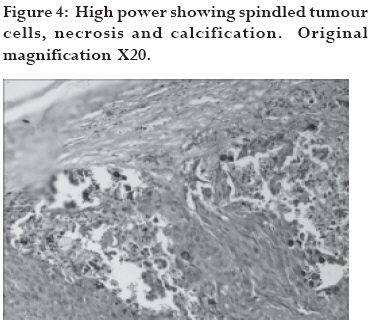
African Health Sciences, Vol. 8, No. 3, Sept, 2008, pp. 186-189 Case Report Emergency partial thyroidectomy under cervical block to relieve severe acute airway obstruction from thyroid cancer A.A. Musa1, S.B. Adebayo2, A.A.F. Banjo3, E.A. Oyewole4, S.O. Olateju5 1 Department of Surgery, Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria, Code Number: hs08039 Summary A 75year old male, Nigerian, retired civil servant presented to the Surgical Endocrine Unit of the Olabisi University Teaching Hospital, Sagamu, Nigeria with features of severe acute airway obstruction from advanced thyroid cancer. He was immediately worked up for an emergency partial thyroidectomy within an hour of arrival in the hospital under superficial bilateral cervical blockage using 2% xylocaine with aderanalin (30mls) 1:100,000 with mild sedation, using 10mg pentazocine and 5mg diazepam as other forms of anaesthesia were not feasible because of his worsening respiratory distress. Findings at operation were a very haemorrhagic, friable thyroid gland with all the lobes matted together. He had isthmusectomy with bilateral partial lobectomy to relieve pressure on the trachea. Respiration improved in the immediate post-operative period as reflected by the values of arterial blood gases. He was maintained on respiration and intranasal oxygen therapy in Intensive Care Unit (ICU) for 2 days. He had an uneventful recovery and was discharged 2weeks after surgery. He had radiotherapy and was followed up in the clinic for a year. Introduction Emergency thyroidectomy necessitated by severe upper airway obstruction is quite rare because most patients are asymptomatic1-5. Most often than not, presentations for treatment are prompted by recent rapid increase in size of goitre with symptoms relating to pressure on the trachea or oesophagus or presence of a mass in the neck1-5.Thyroidectomy is often an elective operation but occasionally this has to be done on emergency basis especially when there are features of airway obstruction (almost leading to acute respiratory arrest)1 5. We present a-75-year-old man who presented with an advanced carcinoma of the thyroid with associated severe airway obstruction. To the best of our knowledge, this is the first report of a male patient with an advanced carcinoma of the thyroid gland associated with severe airway obstruction having emergency thyroidectomy under regional block less than an hour on arrival in the hospital.2,4,5 Case presentation A-75-year-old retired Civil Servant presented with a 2½ year history of a painless, progressively enlarging anterior neck swelling and a left sided anterior chest wall swelling of almost equal duration (Fig. 1).There were no toxic symptoms. However, 6 months prior to presentation, he noticed hoarseness of voice which had been progressive and a rapid increase in the size of the neck swelling. There was associated increasing dysphagia to solid food and worsening early fatigability on mild exertion but no associated orthopnoea, paroxysmal nocturnal dyspnoea and no pedal oedema. He had lost considerable weight despite good appetite. The anterior chest wall swelling had been increasing gradually as well but denied any history of trauma. He was not a diabetic or hypertensive. Two days before presentation his breathing became increasingly difficult with associated dysphagia. He was initially seen at a private hospital from where he was referred to our hospital in an ambulance with intranasal oxygen therapy. His physical examination revealed an elderly man, chronically ill, cachexic and in respiratory distress, respiratory rate of 40 cycles min 1, using all accessory muscles of respiration with flaring of alae nasi. He was afebrile, not jaundiced and acyanotic. His pulse was 110 beats min 1, regular, good volume and no arrhythmias. And a blood pressure of 130/80 mmHg. The heart sounds were normal. He had a moderate size anterior neck swelling, which was nodular and hard in most areas measuring 12 cm by 10 cm with prominent veins. The mass extended from the submandibular region to the root of the neck (Fig 1). The trachea could not be palpated and the carotid pulsations were barely palpable. There was an oblong left anterior chest wall non tender mass with prominent veins measuring 20 cm by 7 cm. (Fig. 1). The air entry was normal but there was noisy respiration (audible wheezing and inspiratory stridor). A provisional diagnosis of severe respiratory distress secondary to advanced thryroid carcinoma with possible chest wall metastasis was made. In view of his worsening respiratory distress, he was prepared for an emergency thyroidectomy. Consults were sent to the otorhinolaryngologists as well as the anaesthetists for an urgent review. The electrolytes and urea and the haematogical results were within normal limits. Echocardiogram (ECG) was normal except for sinus tachycardia and atrial premature complexes. Plain X-ray of the neck revealed severe narrowing of trachea and marked deviation to the right (Fig 2). The thyroid function test results were T3 1.4 nmol/L (1.0 3.25), T4 36 nmol/L (65 175) and TSH 2.6 mU/L (0.5 6.5). Pre-operative assessment of the vocal cords was not possible because of the worsening respiratory distress. The anaesthetic assessment was a poor anaesthetic risk patient for general endotracheal anaesthesia with ASA IIIE, Mallanpati IV, SRC III, especially in view of X-ray features of tracheal stricture. He had 3 pints of blood urgently grouped and crossmatched for him and was rushed to theatre. Anaesthesia and surgery The patient in supine position with a slide head elevation and later put in lateral position, had bilateral cervical blockade using 30mls of 2% xylocaine with adrenalin 1:100,000. Facing the opposite direction from the side to be blocked with a slight head lift and tilt to make anatomy of the neck especially the borders of the scleidomastoid muscle prominent, the mastoid and transverse process of C6 cervical vertebra were identified. The midpoint of the distance between the two landmarks was identified at the posterior border of the scleidomastoid muscle. This marks the surface marking of the cervical plexus (C2 -C4) and the needle was inserted here perpendicularly at the level of investing layer of the neck. At this point 5mls of the anaesthetic agent was injected. Still maintaining the level at this point, the needle was now directed upwards at 30% to the horizontal and another 5mls was injected and finally the needle was directed distally at 450 and the last 5mls was injected. The same was repeated on the contralateral side. Before incision, a local skin infiltration of the agent was done along the incision line. A nasogastric tube was passed to guide our dissension and prevent injury to the oesophagus. The patient was finally placed in the classical position for thyroidectomy. Upper and lower flaps were raised accordingly and the findings at operation were a very haemorrhagic thyroid gland with the two lobes and the isthmus matted together (Fig 3). Hence, by a combination of scissors dissection and finger fracture technique, dissection was limited to the isthmus at the centre and extended laterally bilaterally to do partial lobectomy on the two sides in order to relieve pressure on the trachea by the thyroid cancer. Haemostasis was maintained. A rubber drain was left in place and closure was done in layers. The respiration improved in the immediate post operative as shown by the improvement in the arterial partial pressure of oxygen in the blood. He was nursed in Intensive Care Unit (ICU) with oxygen therapy for 24hours and observed for another 24hours before discharge to the wards. He spent 2 weeks in the hospital and was subsequently sent for radiotherapy. He was followed up for one year in the surgical out-patient department. The histology of the specimen was in keeping with medullary carcinoma of the thyroid gland (Fig 4). Discussion Malignant diseases of the thyroid causing compression, direct invasion of the trachea as well as obstruction of the anatomical structures passing through the thoracic inlet had been reported by many authors1-7. So also were benign goitres causing obstructive and acute respiratory arrest. 6, 7, 8. Nonetheless, upper airway obstruction by goitre is still uncommon because up to 75% of the tracheal lumen may be compressed without causing symptoms2. Acute or chronic respiratory failure secondary to tracheal compression by goitre is extremely rare2. In developed countries where medical services are readily available, patients with obstructive symptoms present early as against developing countries where goitre is often ignored probably due to ignorance, inadequate and inaccessible medical services 2, 9. Obstructive symptoms are usually insidious and evolve over a period of time especially in substernal goitre anatomically, there is enough room to accommodate the gland. This is in contrast to the retroclavicular goitre, which often causes acute respiratory distress that may progress to arrest of respiration 2, 6, 7. We believe in this patient, direct pressure on the tracheal might be responsible for this sudden severe respiratory distress. In an earlier work, Raftos, Ethell and Hilary established some of the factors which contribute to deterioration of upper airway in goitre patients to include old age; impairment of perception; dementia and rapid expansion of goitre if there is bleeding into its substance2,3,10, 11. We therefore believe that in addition, to the effect of direct pressure of the gland on the trachea, deteriorating upper airway in an aged patient with advanced cancer of the thyroid gland were part of the problems this patient was facing. Acute respiratory distress due to thyroid compression of the tracheal lumen especially with extrathyroidal tumours of the goitre is both surgical and anaesthetic emergency11 with a lot of challenges 11,12,13. Initially, we considered intubation but the X-ray of the neck and thoracic inlet showed marked deviation to the right, kinking and severe stenosis (Fig 2) that would make intubation difficult or impossible. The idea of awake intubation, spraying or traumatizing a narrowed and oedematous airway would worsen the situation. More so, the patient can go into respiratory arrest with muscle relaxants if intubations failed3,11. We therefore resorted to regional anaesthesia employing the technique of bilateral superficial cervical block using xylocaine with adrenaline. We had earlier reported that regional anaesthesia for thyroidectomy has become routine practice in our center (since 2001) for the past 5years due to inadequate anaesthetic manpower14. Though, other workers had also reported same and the use of other forms of anaesthesia other than endotracheal intubation anaesthesia for thyroidectomy 3. Our initial fear was that the nerves to be blocked C2-C415 might have been consumed in the malignancy process because of the wide spread matastases and thereby rendering the block ineffective. But the regional block was effective and debulking of the tumor was successfully done especially around the area of the isthmus to relieve the obstruction. A nasogastric tube was also passed intraoperatively to guide our dissection to avoid injury to the oesophagus1. The patient's respiration improved and had an uneventful post operative recovery. He spent about 2 weeks in the hospital and was subsequently discharged for external radiation. He was followed up in the surgical out-patient clinic for 1year. Conclusion This further reinforces our earlier work that regional anaesthesia for thyroidectomy is feasible both in rural and sub urban centres where anaesthetic equipment and manpower are inadequate. This could also be employed as an alternative form of anaesthesia when general anaesthesia endotracheal intubation is not advisable in surgical/anaesthetic risk patients. References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08039f3.jpg] [hs08039f1.jpg] [hs08039f2.jpg] [hs08039f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}