 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 3, Sept, 2008, pp. 190-195 Short Report Worsening and unmasking of tuberculosis in HIV-1 infected patients after initiating highly active anti-retroviral therapy in Uganda Joshua Baalwa,1* Harriet Mayanja-Kizza,1 Moses R. Kamya,1 Laurence John,2 Andrew Kambugu,1 & Robert Colebunders3 1. Makerere University, Infectious Diseases Institute, Kampala, Uganda, Code Number: hs08040 AbstractObjectives: To determine the proportion of patients developing active tuberculosis (TB) versus that of patients who
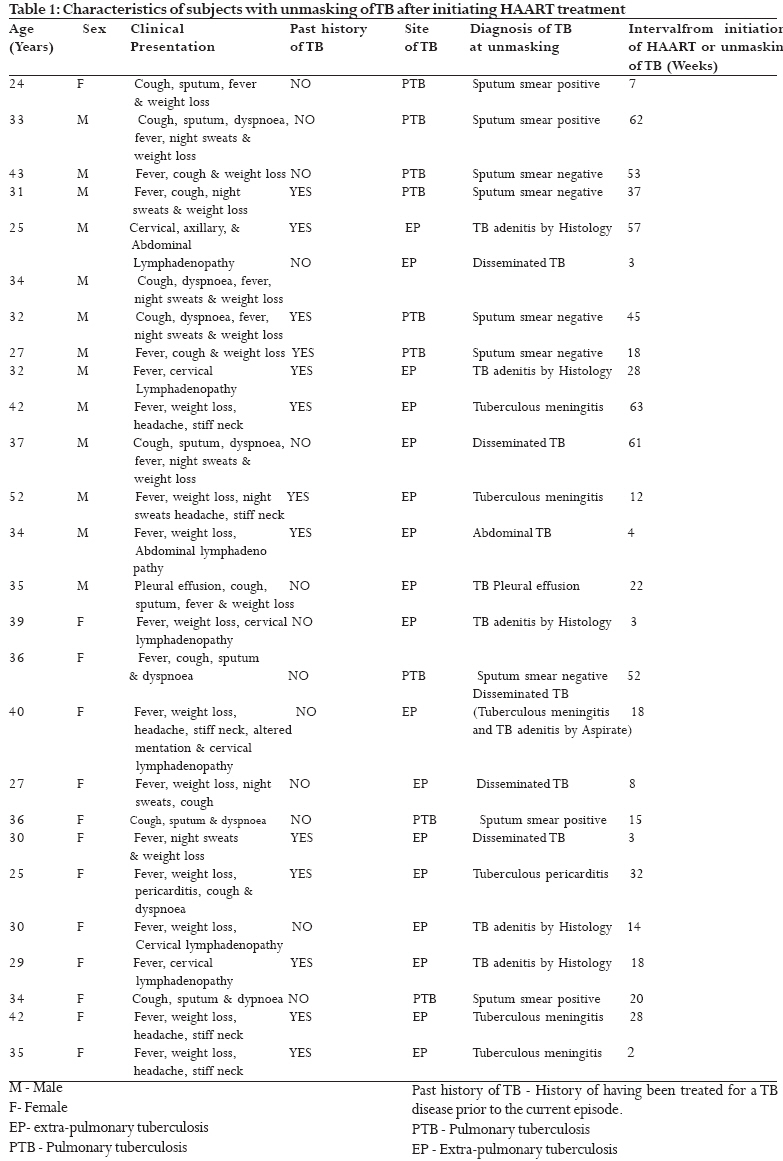
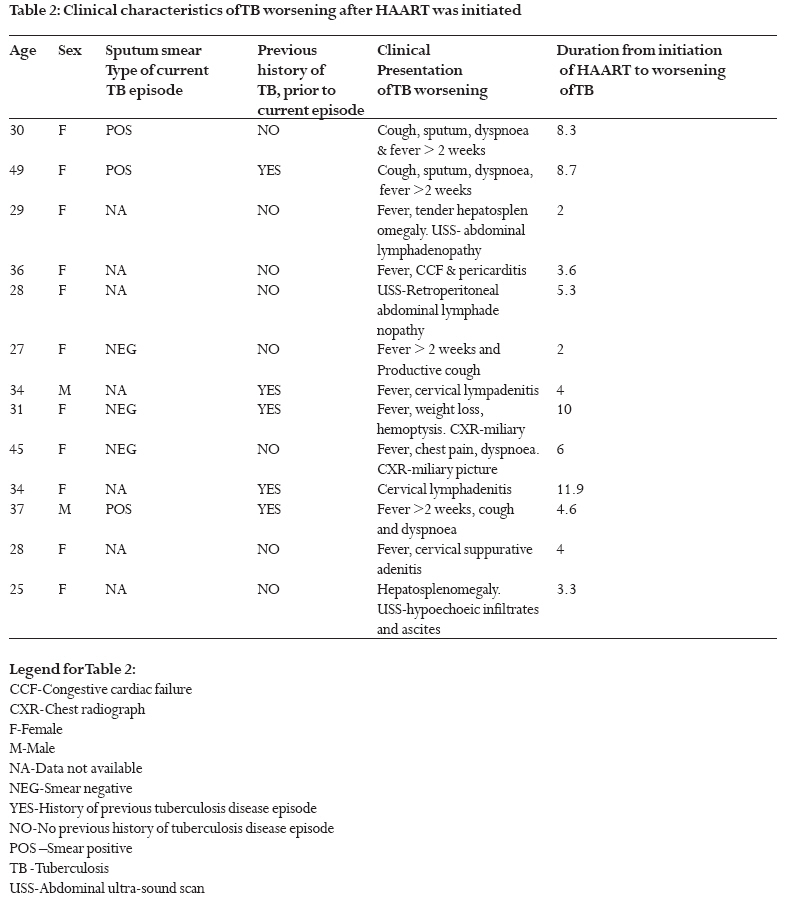
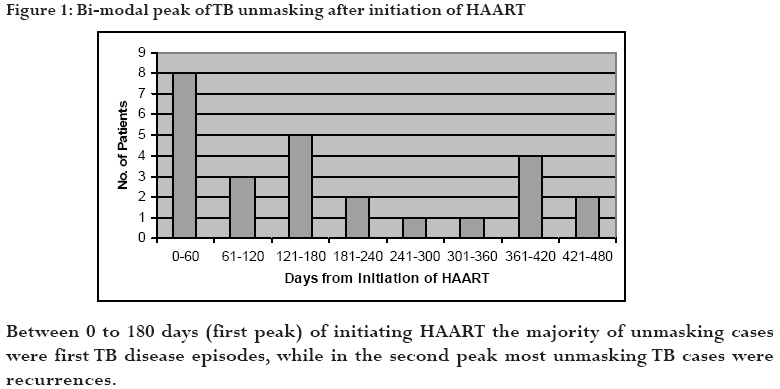
experience worsening of TB, after initiating highly active anti retroviral therapy (HAART). Keywords: Immune reconstitution, tuberculosis, antiretroviral therapy Introduction Restoration and preservation of immune functions by highly active anti-retroviral therapy (HAART), has led to a significant risk reduction for tuberculosis (TB) and improved survival of TB-HIV co-infected patients1-4. However in some instances HAART induces deleterious effects, such as increased morbidity, which are attributable to immune reconstitution enhanced inflammatory responses against TB antigens. This TB related morbidity following HAART may manifest itself as paradoxical worsening of active TB undergoing successful treatment or progression of latent TB infection to active TB (unmasking), and has been termed as TB immune reconstitution inflammatory syndrome (TB-IRIS)5-15. Few studies have systematically highlighted the burden of TB-IRIS in Sub-Saharan Africa, despite TB and HIV co-infection being highly prevalent in this region. In this study, we characterized patients with paradoxical worsening and new onset or recurrence of active TB after initiating HAART. Methods Design and study population We reviewed charts of 316 anti-retroviral therapy naïve patients who started HAART between March 2003 and September 2004 at the Infectious Diseases Institute, Makerere University Kampala, Uganda, and were still alive by March 2005. Using the HAART register, 271 charts of HAART naïve patients who commenced HAART without clinically active TB were identified and reviewed for development of new episode of active TB disease. Another 45 patients who commenced HAART during anti-TB treatment were identified using the TB and HAART registers and assessed for worsening of TB. Patient charts were reviewed from the time they commenced HAART up to the end of March 2005. All adult patients (age e"18 years), with confirmed HIV-1 infection and eligible for HAART according to the Ugandan ART guidelines were included. Patients were excluded if they had a prior history of default or clinical failure of TB treatment, if they were on HAART prior to March 2003 or if they were not adherent to HAART during the study period. Patients on TB treatment were eligible for the study if they were adherent to their current anti-TB medication, and if the decision to commence HAART was taken after their response to TB treatment was deemed satisfactory. The primary study outcomes were; new active TB disease or worsening of TB symptomatology, after initiating HAART. New active TB cases were further categorized into early or late unmasking TB groups, if TB developed within or after 6 months of initiation of HAART respectively. Case definitions Worsening of TB was presumptively confirmed if a patient responding to adequate TB treatment, paradoxically redeveloped clinical features and new radiological signs suggestive of TB after initiating HAART and did not respond to empiric broad spectrum antibiotic therapy or had no other cause identified after clinical and laboratory evaluation. A person with new active TB unmasking while on HAART was defined as having smear positive pulmonary TB if microscopy of their sputum revealed acid fast bacilli (AFB). Additionally, some patients with failure of B symptoms (fever, night sweats and weight loss) to respond to an antibiotic trial were presumptively diagnosed with disseminated TB if they showed clinical response to anti-TB trial therapy. Patients were presumptively diagnosed to have smear negative pulmonary TB if they had persistent B symptoms despite a trial of broad spectrum antibiotic and a chest radiograph suggestive of TB but with three or more negative sputum smears for AFB. Tuberculous meningitis, abdominal TB, tuberculous pleural effusion, TB adenitis and TB pericarditis were diagnosed as per the Uganda National TB Treatment guidelines16. Results Of the 271 HAART naïve patients without TB at baseline, 16 (5.9%) developed active TB within 6 months (early unmasking) and 10 (2.7%) after 6 months (late unmasking) after initiating HAART. The mean duration from initiation of HAART to unmasking of TB was 25 weeks, with a range of 2 to 63 weeks and median of 18 weeks. Seven of 10 (70%) late unmasking TB subjects had prior history of treatment for a TB disease episode, compared to 6 of 16 (37.5%) early unmasking TB subjects. Thirteen (29%) of 45 patients on TB treatment experienced worsening of TB symptoms and signs after commencement of HAART. The mean duration from initiation of HAART to worsening of TB was 6 weeks, with a range of 2 to 12 weeks and median of 5 weeks. Nine of 45 commenced HAART during the intensive phase of TB treatment, of whom 2 (22%) experienced worsening of their TB, while 36 of 45 started HAART during the continuation phase of TB treatment of whom 11 (31%), experienced worsening of their TB.Table 1 and 2 below summarize the characteristics of patients who developed new active TB or worsening of TB after HAART was initiated. Discussion Overall, this study reveals that a substantial proportion of patients develop active TB within weeks to months of initiating HAART or worsening of TB while on concurrent anti-TB and HAART medications. Our study limitations included the unavailability of CD4 count and viral load results at the time of TB worsening, and the diagnosis of active TB not being corroborated by positive culture results. Despite this, the study was similar in design to those reported elsewhere 7, 8,11, 16 and our findings provide vital baseline statistics regarding TB-IRIS in East Africa where HIV-1 clades A and D infections predominate.17 Moreover, all patients meeting the criteria of our study end points, had their records further scrutinized by the study team, composed of a panel of clinicians with considerable experience in HIV/TB treatment. This study also reaffirms what earlier studies had found, that despite significant reduction in the risk of TB acquisition during HAART treatment, a small proportion of patients remains at risk for TB disease especially those from TB endemic areas who might harbor undetected latent TB infection6, 18. In a study by Bonnet M.B. et al, conducted in 5 high TB burden countries, the risk for pulmonary TB after initiation of HAART ranged between 7.6 and 17.6% per 100 person years.19 In less TB endemic areas, unmasking of TB has been shown to occur in high proportions among immigrants from TB endemic areas and black populations who initiate HAART without concurrent active TB disease.7 Notably, our study found that the majority of patients (70%) who developed active TB six months after initiating HAART (late unmasking) were TB recurrences, while those who developed active TB within 6 months of initiating HAART (63%) were experiencing their first active TB episode. This finding apparently reveals a limitation in the protective effects of HAART against TB recurrence and arguably reiterates the need to consider TB chemoprophylaxis as a supplement to HAART in reducing TB incidence among HIV-1 infected populations in TB endemic areas20. Alternatively, studies are required to determine if earlier initiation of HAART, when CD4 counts fall < 350/mm3 , is superior in reducing TB incidence compared to what is conventionally practiced in Uganda and other developing countries today. In the past, some reports have suggested that delaying HAART may significantly reduce the risk for TB-IRIS.16, 21 However, this was not the case with our study since more than 80% of TB-IRIS cases occurred when HAART was initiated during the continuation phase of TB treatment. Thus, considering the remarkable survival benefit of HAART particularly in TB patients with advanced AIDS,4 we propose that the decision to delay HAART should mainly be based on the likelihood of overlapping toxicities and high pill burden other than the anticipation for IRIS, pending systematic observations from large prospective studies. Acknowledgements: This work was supported supported by a grant from the National Institutes of Health-Forgaty International Center (FIC) to TB-HIV Clinical Operational and Health Services Research (COHRE) project based at the Joint Clinical Research Center (JCRC), Kampala, Uganda. We thank Prof. Nelson K. Sewankambo, Prof. Elly Katabira, Prof. Peter Mugyenyi and Prof. Allan Ronald for their input; Regina Namirembe and Nelson Kakande of the COHRE secretariat at JCRC for their logistical support and Shuyi Wang for graphics and manuscript preparation. REFERENCES
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08040t1.jpg] [hs08040f1.jpg] [hs08040t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}