 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, Suppl, 2008, pp. S14-S20 Resilience among first responders Luca Pietrantoni and Gabriele Prati Department of Science of Education, University of Bologna (Italy). Code Number: hs08059 Abstract Background. Emergency rescue personnel can be considered a ``high risk'' occupational group in that they could experience a
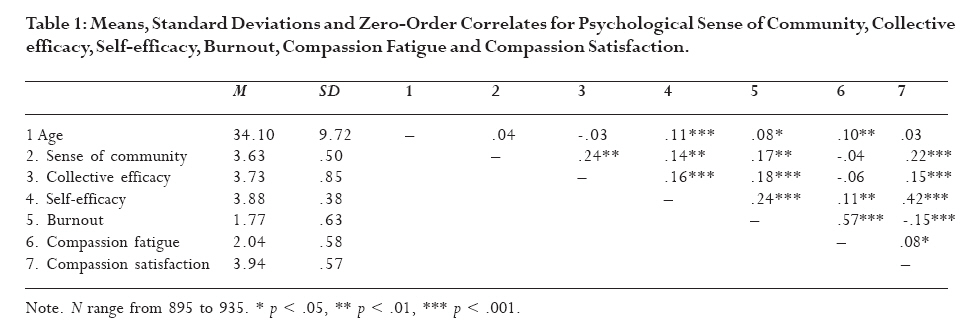
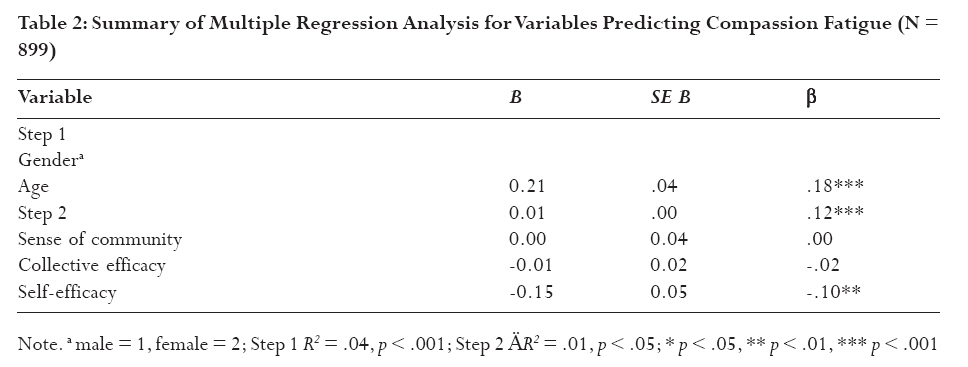
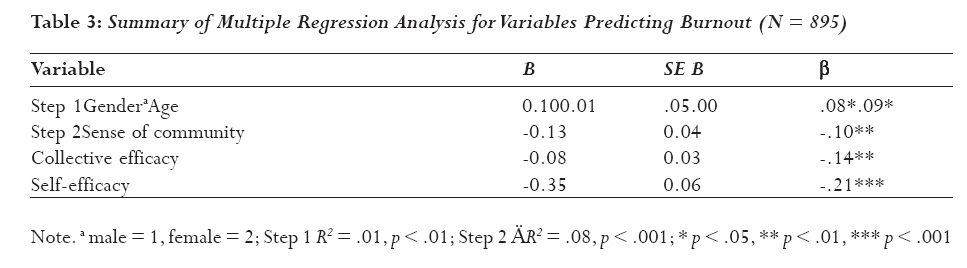
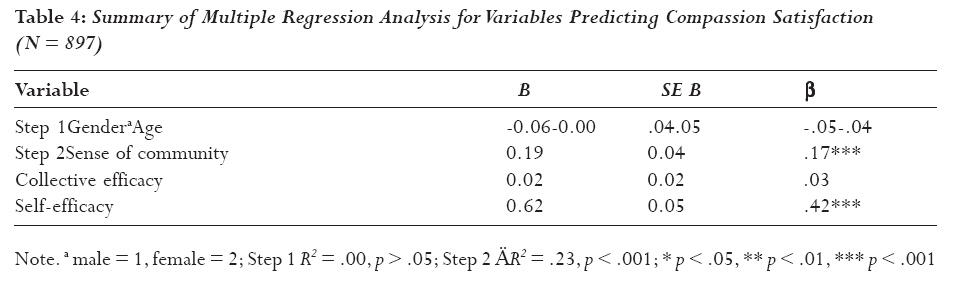
broad range of health and mental health consequences as a result of work-related exposures to critical incidents. Introduction There is considerable evidence on psychopathologic effects of trauma victims. In the last decades there has been a paradigm shift from pathogenesis (etiology of disease) to salutogenesis (origins of health) in the conceptualization of functioning following trauma1. The resilience literature best represents this paradigm shift. Traditionally resilience literature focused on childhood development and on adolescence development. However in the last years the resilience studies has considered the adulthood, mainly in the face of loss or potential trauma. Bonanno2 defined resilience as the "ability of adults in otherwise normal circumstances who are exposed to an isolated and potentially highly disruptive event, such as the death of a close relation or a violent or life-threatening situation, to maintain relatively stable, healthy levels of psychological and physical functioning". On the other hand Almedom and Glandon3 cast doubt upon the equivalence of absence of symptoms of post-traumatic stress disorder with evidence of resilience and proposed that sense of coherence construct "may give a fuller understanding of the complexity of resilience, a dynamic steady state that cannot be measured in isolation from its context of generalized resistance resources, including social support". During the International Resilience Workshop - Talloires 2007, resilience was examined using a holistic approach that embrace both a pathogenic and a salutogenic (health-centered) perspective as two ends of a continuum. The resilience research suggests two key points. First resilience had recently been recognized as a common human response to potentially traumatic events4. Second there are multiple resources, both at the individual and at the environmental level, which could foster adaptation in face of challenge5. More recently, the concept of resilience has been applied to first responders: people whose job entails being the first on the scene of an emergency, such as firefighters, paramedics or police officers. First responders are exposed to potentially traumatic events as part of their duty such as accidents involving children, mass incidents, major fires, road traffic accidents, burns patients, violent incidents, and murder scenes. These events are named critical incidents in that may be any event that has a stressful impact sufficient enough to overwhelm an individual's sense of control, connection and meaning in his/her life. Evidences showed that proximity, duration, and intensity of exposure are the most significant predictors of first responders' physical and mental health symptoms6. The literature focused on negative outcomes such as traumatic stress symptoms7,8,9, secondary traumatic stress or compassion fatigue10,11 and burnout12,13. Finally, research findings showed that critical incident exposure and rates of general psychopathology were higher among first responders in South Africa compared to the Sweden and the United States14. In this research area the resilience concept has been useful for three reasons. First, exposure to critical incidents, involving death or life threatening injury, is potentially an integral part of the job for emergency services personnel. First responders can be considered a ``high risk'' occupational group in that they could experience a broad range of health and mental health consequences as a result of work-related exposures to critical incidents6. Thus, it is appropriate to investigate resilience in this population. Second, traumatic stress, compassion fatigue and burnout are not the only possible emergency work-related outcomes. For example, research findings evidenced that emergency ambulance personnel reported positive post-trauma changes (posttraumatic growth) as the result of the experience of occupational trauma15. Stamm16 introduced the concept of Compassion satisfaction, defined as the benefits that individuals derive from working with traumatized or suffering persons. These benefits include positive feelings about helping others, finding meaning in one's effort and challenges, fulfilling one's potential, contributing to the work setting and even to the greater good of society, and the overall pleasure derived from being able to do one's work well. Thus, the psychological consequences of emergency work are not only negative but even positive. This is a very important point in the resilience literature since resilience is more than absence of negative mental health3 and encompasses positive aspects and consequences of potentially traumatic events17. In fact, resilience could be considered "multifaceted construct are drawn from both the salutogenic and pathogenic camps as well as the interface between the two"3. The third reason is related to the identification of the personal and environmental resources that promote positive adaptation in face of critical incidents. Scientific research has focused increasing attention on predictors of potential negative consequence of emergency work resulting from exposures to critical incidents6. However, much of the attention on predictors of psychological consequences of critical incidents has been focused mostly on risk factors such as degree of exposure, peritraumatic distress, peritraumatic dissociation, presence of subsequent stressful life events, identification with the victim and hostility7,18,19,20,21. By contrast, the resilience field address the role of protective factors in predicting positive adaptation in a risk population such as first responders. Research findings evidenced that resilience factors are located on individual and contextual resources5. Among individual factors, previous researches showed that self-efficacy is an important factor in reducing levels of distress22,23 and it is associated with lower levels of traumatic stress symptoms and depression in firefighters20,24,25. Cognitive mastery of an event has been found as frequently used by first reponders23. Efficacy beliefs pertain to the individual beliefs in one's own capability to exercise some measure of control over in one's own functioning and environmental events26. Efficacy beliefs are not only related to the individual level but even at the collective level. Collective efficacy refers to what people choose to do as a group, the effort they put into it and the perception of the group's ability to accomplish its major tasks26. Emergency rescue work, owing to its characteristics, requires working collaboratively and in a coordinated way as a group: no first responder can be effective working alone without making reference to an organization. As a consequence, the expectation of success influences the outcome of the performance, as it shapes the way group members react to critical incidents. In this perspective, perceived collective efficacy predicts job satisfaction and well being27. Besides organizational level, we want to point out that first responders' occupation is aimed at protecting the local area, at alleviating suffering (and saving lives) of individuals and groups, which may belong to their own community. Thus, first responders' sense of community, which includes, according to McMillan and Chavis's model28, dimensions like feeling of belonging and emotional connection with the community, perceived influence over it and perceived opportunities for satisfying one's needs through such belonging, may be particularly important for rescue personnel, and may constitute a protective factor. The construct of sense of community has been investigated in this population (in particular, fire fighters)29. In their study sense of community was related to low level of distress and high level of satisfaction. However, in such research, the construct was examined at the organizational level as the perception of belonging to a community of co-workers. This study aims at investigating first responders' resilience factors. We therefore expect that self-efficacy, collective efficacy and sense of community could be related to less negative outcomes and to more positive outcomes both related to rescue work. Departing from previous research on resilience, in the assessment of health outcome a decision was taken to focus not only on posttraumatic symptoms and on negative outcomes in a wider sense but to introduce an additional assessment of positive consequences of rescue work. Finally, given that the notions of sense of community and collective efficacy are widely discussed in the literature on mental health and social capital and/or social support, and there is evidence to show gender and age differentials, we assess the effect of age and gender. Methods Procedure The present study employed a survey methodology, using a questionnaire. The instrument consisted an on-line questionnaire. To collect the data, the on-line questionnaire was posted on the webpage of the Emergency Psychology Group of the Faculty of Psychology of the University of Bologna (http://emergenze.psice.unibo.it/ricerca.soccorritori.html ). Included was also a general introduction on the purpose of the research and a consent form to be signed as a precondition to proceed with the completion of the questionnaire. In order to obtain a wide representation of the different typologies of emergency work personnel in the Italian context, prior to the beginning of the study, which was conducted in Spring 2007, an e-mail message was sent to the webmasters of the principal Italian organizations of first responders (Fire fighters, Civil Protection, Emergency Intervention Services, Red Cross), at a national, regional and local levels. The mail included a presentation of the study and a request for collaboration by linking the questionnaire web page to their official web site to encourage their members to fill it. We considered the questionnaires completed within five months from the posting of the questionnaire. Instrument The questionnaire included the following areas: Demographics: included were questions on gender, age and length of service. Work related health outcomes were assessed by the ProQOL R-IV (Professional Quality of Life Scale. Compassion Satisfaction and Fatigue Subscales - Revision IV), including 30 items corresponding to three scales: Compassion Satisfaction Scale, Burnout Scale and Trauma/Compassion Fatigue Scale16. Participants were asked to specify how often, during the last month, they had experienced a series of emotional states. Responses were given on a five-point Likert scale, ranging from "never" (value 1) to "very often" (value 5). The ProQOL was subjected to Factor Analysis procedures. A preliminary inspection of the descriptive statistics leads to discard seven items owing to unsatisfactory psychometric properties or cultural inappropriateness for the Italian context. Factor analysis (method Principal axis factoring, Promax rotation, kappa = 4) was conducted on the remaining items. Visual inspection of the scree plot, ease of interpretation, and theory indicated that the three-factor solution was the best fit. The first factor ("Compassion Satisfaction") includes the items from the Compassion Satisfaction Scale and two items from the Burnout Scale (Variance explained = 22.18%) (± =. 86); the second factor ("Compassion fatigue") includes six items of the Trauma/Compassion Fatigue scale and two items from the Burnout scale (Variance explained = 11.39%) (± = . 80) and the last one ("Burnout") includes four items from the Burnout scale and two items from the Trauma/Compassion Fatigue Scale showing higher loadings on this factor than on the original scale (Variance explained = 5.35%) (± = . 77). Subscale mean scores were calculated by averaging across the specific items included into the three factors (see Table 1). Sense of Community was assessed by the "Italian Sense of Community Scale"30. Response alternatives were on a five point Likert scale from "strongly agree" (value 5) to "strongly disagree" (value 1). An overall score of Sense of Community was created, after reversing the negatively worded items, so that higher scores indicated higher Sense of Community. Cronbach's alpha is .81. Collective Efficacy was measured by the "Perceived Collective Efficacy for members of volunteering associations"31, including five items. The instrument measures the extent to which members perceive their association or organization capable to face different situations and critical events occurring during their typical everyday activity. Response alternatives are provided on a five-point Likert scale from "completely agree" (value 5) to "completely disagree" (value 1). An overall score was calculated in such a way that higher scores correspond to higher Collective Self-Efficacy. Cronbach's alpha was .85. Self-efficacy was assessed by the "Perceived Personal Efficacy for members of volunteering associations" 31. The instrument includes 18 items, assessing the extent to which members of associations feel capable to face the challenges arising from their activity. Response alternatives are provided on a five-point Likert scale from "never" (value 1) to "very often" (value 5). An overall score was calculated so that higher scores correspond to higher personal Self-efficacy. Cronbach's alpha was .78. Participants The final sample included 961 first responders, 71.9% male and 28.1% female. Age ranges from 18 to 66 years (M = 34.10, SD = 9.72). They include fire fighters, Civil Protection volunteers, different categories of emergency medical service personnel (medical first respondents, medical technicians, paramedics, nurses, ambulance personnel, ambulance drivers). Length of service ranged from 0 to 36 years (M = 9.36; SD = 7.40). Results Men tend to show higher scores on sense of community [men M = 3.66, DS = 0.50; women M = 3.56, DS = 0.49; t(933) = 2.75, p < .01]. There are no gender differences on collective efficacy [men M = 3.72, DS = 0.87; women M = 3.74, DS = 0.81; t(915) = -0.24, p > .05] and self-efficacy [men M = 3.89, DS = 0.39; women M = 3.86, DS = 0.37; t(928) = -1.04, p > .05]. Table 1 summarizes mean values and standard deviations for each variable and reports correlation coefficients. On average, our sample reported mean scores above the mid-range of the scale for the variables sense of community, collective efficacy, self-efficacy and compassion satisfaction. The mean scores for burnout and compassion fatigue were below the mid-range of the scale. Age is significantly related to self efficacy, burnout and compassion fatigue but not to sense of community, collective efficacy and compassion satisfaction. All the other correlations are statistically significant with the exception of the relation of compassion fatigue to sense of community and collective efficacy. The magnitude of the correlation coefficients is large for the relations between burnout and compassion fatigue and selfefficacy and compassion satisfaction. In order to assess the predictive role of sense of community, collective efficacy and self-efficacy on the three dimensions of work related health outcomes controlling for age and gender, three hierarchical multiple regression analyses were performed. According to Cohen32, f2 effect sizes of 0.02, 0.15, and 0.35 are considered small, medium, and large, respectively. Table 2 shows the results of multiple regression analysis on compassion fatigue. The effect size for the second step multiple regression is small (f2 = .01). Selfefficacy is the only significant predictor variable. Female sex and higher age predict compassion fatigue. Table 3 presents the results of multiple regression analysis on burnout. The effect size for the second step multiple regression is between medium and small (f2 = 09). All the variables significantly predicted burnout scores. Female sex and higher age predict burnout. Table 4 shows the results of multiple regression analysis on compassion satisfaction. The effect size for the second step multiple regression could be considered quite large (f2 = .28). Collective efficacy is the only non-significant predictor variable. Gender and age do not predict compassion satisfaction. Discussion The present study addressed the protective role of sense of community, collective efficacy and self-efficacy on rescue work. The literature has focused extensively on the risk factors for traumatic stress symptoms following exposure to critical incidents. According to Almedom and Glandon3 resilience following traumatic events is more than the absence of traumatic stress symptoms. This study investigated the protective factors of a more holistic measure of rescue work related health outcomes ranging from negative to positive indicators. Results showed that first responders experience a good level of satisfaction and low level of burnout and compassion fatigue as results of their job. Thus, this study showed that most of first responders are not affected by traumatic stress or burnout syndrome despite their exposure to critical incidents. It is likely that first responders could rely on personal and social resources in order to cope with critical incident stress. This study showed that personal and social resources could protect first responders' health. Furthermore we discovered that personal and social resources have a different impact on different work related health outcomes. Overall, results of the study are consistent with our hypotheses, and with previous findings in the literature. More importantly, they provide additional information on aspects that have been insufficiently investigated, such as the role of sense of community and of collective efficacy. First responders' feeling of belonging to the community where they live and work is an important contributor to satisfaction and reduces burnout outcomes. This finding adds to previous research showing the important role of sense of community referred to the "community" of co-workers29. The importance of organizational factors, as measured by collective self-efficacy as a group, is in line with these results. However, collective efficacy does not predict compassion satisfaction. We underline that compassion satisfaction and collective efficacy are significantly related but this relation is not anymore significant when controlling for sense of community and self-efficacy. It is likely that collective efficacy could be more important for collective satisfaction than for personal satisfaction. The role of collective efficacy remains to be fully clarified by future studies. Furthermore, either sense of community and collective efficacy are not related to compassion fatigue. Our interpretation is that organizational and community level variables could be considered as a distal variable that relates the more proximal determinants, such as self-efficacy, of compassion fatigue. The small effect size in predicting compassion fatigue indicates that there are other protective factors, such as hardiness, self-enhancement, coping strategies, social support and social network2,5, that could explain more variability. Compassion satisfaction (including positive feelings about helping activity), is strongly influenced by sense of community and self-efficacy. In this study, efficacy beliefs pertain to the individual beliefs in one's own capability to exercise some measure of control in one's own job while sense of community involve the ties that link rescue worker to the place where they live and work. A perception of confidence in their job-performance abilities and a feeling of belongingness and attachment to a place could be beneficial in first responders in that they give a sense of control and of meaning in their job. Control and meaning are similar, respectively, to Manageability and Meaningfulness, two components of Sense of coherence1, a construct used to assess resilience in Eritrea33. The finding concerning the protective role of self efficacy in rescue work confirms the results of previous studies20,22,24,25. Women tend to score lower on sense of community. The difference is minimal albeit statistically significant. Older first responders are different in terms of self efficacy beliefs: it is likely that efficacy is related to work experience. Female gender and higher age are significant predictors of burnout and compassion fatigue. The flinging of gender is in line with the literature on reactions to potentially traumatic events4. Higher age is related to higher burnout and compassion fatigue probably because it is a proxy of critical incident exposure. Some limitations of the study should be acknowledged. First, the cross-sectional methodology employed in this study precludes any inference of causality. Second, in this study we did not employ qualitative methodology. According to Almedom and Glandon3 resilience is a multidimensional construct that requires a combination of both qualitative and quantitative techniques to be examined satisfactorily. The results of this study outline the need of interventions aimed at the promotion of resilience factors rather than the treatment of negative health symptoms. The research field on the efficacy and effectiveness of interventions for psychological distress and post-traumatic stress disorder in emergency service personnel is still a controversial issue34. There is a need to take into account less formal strategies such as peer support or health promoting or preventing measures during the training programmes and throughout the course the professional life. In addition, our study reveals the need for increasing first responders' psychosocial competences (e.g., communication skills, decision making skills, team working, leadership competences, coordination, crowd management skills), besides technical skills. Such competences affect first responders' efficacy beliefs and, according to our results, might constitute important protective factors for their work related health outcomes. On this point, a model of non technical skills for members of at risk professions that is currently employed in training courses for emergency workers is NOTECHS model35 including cognitive, behavioural and interpersonal/group skills that all emergency workers should have, in order to enhance the efficacy of rescue interventions, and by reflection, their resilience. Given that prevalence of exposure and rates of mental health problems are higher in African first responders in comparison to European colleagues14, we hypothesize that interventions aimed at promoting sense of community and self-efficacy beliefs may be more relevant to African countries. To conclude, the results of this paper evidence the protective role of self-efficacy, collective efficacy and sense of community in emergency rescue work. First responders face, as part of their job, critical incidents that pose a threat to their mental health. However the results evidenced low scores of burnout and compassion fatigue and high scores of compassion satisfaction. We suppose that the presence of resilience factors may compensate for the risks that exist in emergency rescue work. We discovered that efficacy beliefs and sense of community have an influence on work related health outcomes, especially compassion satisfaction. References
© Copyright 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08059t4.jpg] [hs08059t1.jpg] [hs08059t3.jpg] [hs08059t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}