 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 1, March, 2009, pp. 2-12 The dilemma of safe sex and having children: challenges facing HIV sero-discordant couples in Uganda Jolly Beyeza-Kashesya1, 2, Frank Kaharuza1, Florence Mirembe1, Stella Neema3, Anna Mia Ekstrom2 and Asli Kulane2 1Department of Obstetrics/Gynaecology, Makerere University, Kampala Uganda, 2Department of Public Health Sciences,
Karolinska Institutet, Stockholm, Sweden, 3Makerere University Institute of Social Research, Kampala Uganda Code Number: hs09002 Abstract Background: Sixty percent of new HIV infections in Uganda occur in stable relationships between HIV discordant couples.
Given the importance of fertility in Uganda, we hypothesized that unsafe sexual practices may be used to found a family/replace a
dead child. Thus, we explored sexual practices to understand to what extent these are influenced by the desire to have children and
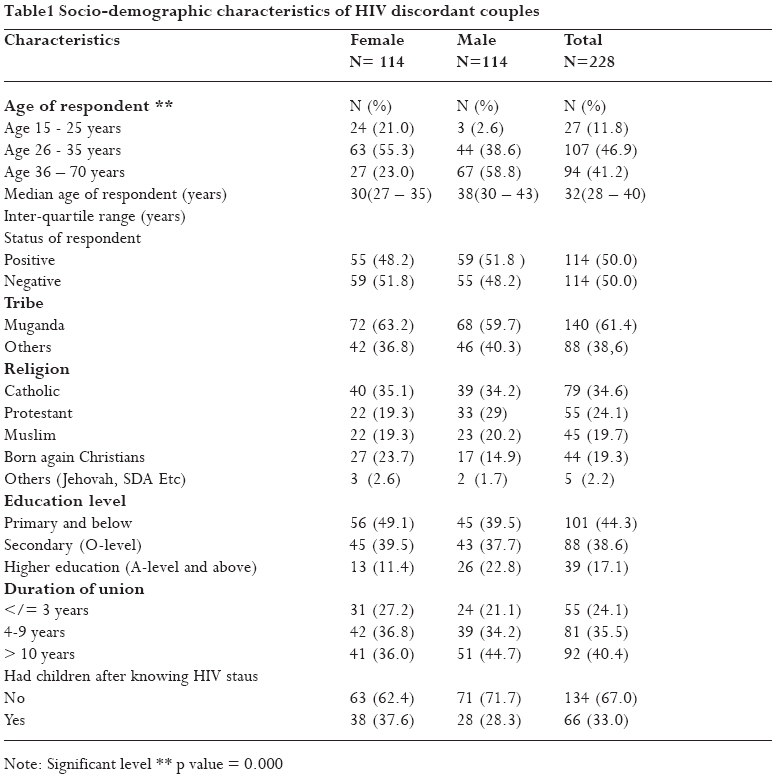
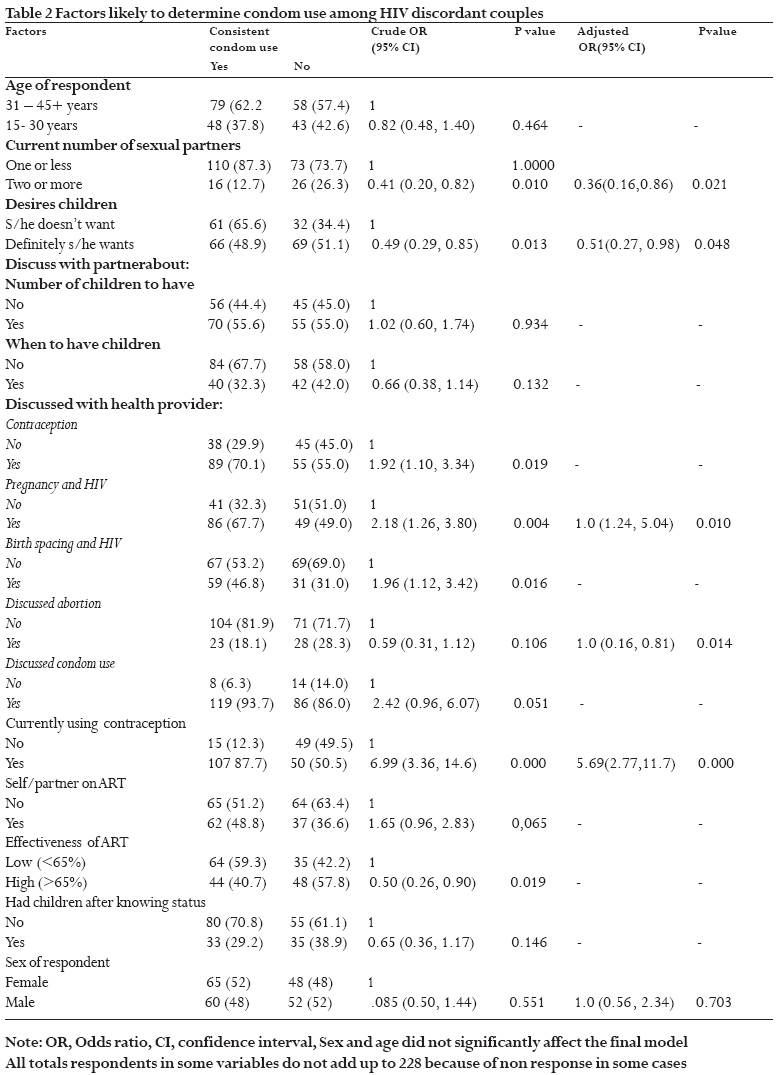
the implications for HIV transmission among discordant couples. Key words: HIV Sero-discordance, condom use, desire for children Background Although Uganda is considered a success story in reducing HIV infection, the HIV prevalence remains unacceptably high and seems to be stagnating or even gathering momentum for an upward trend1 In Uganda, 60% of all new HIV infections occur in HIV sero-discordant couples2 and over 30% of married HIV-positive people have a negative spouse3. The desire for children among HIV infected people is high, especially in the young age group4, and HIV discordance creates a serious dilemma for fertility decision-making in couples. Stigma, discrimination, and non-disclosure fuel HIV transmission between partners5 but also limits pregnant women's access to prevention of mother-to child transmission (PMTCT) services. HIV is also associated with an increased risk of both maternal and child deaths 6 Favorable trends in incidence in several countries are believed to be due to behavior change and prevention programs7-9, but these must be based on knowledge of cultural norms, traditions and sexual and reproductive health practices2 that likely differ between countries10. We hypothesised that discordant couples trying to found a family or replace/have another child may shun condom use and other HIV prevention strategies. This study explores sexual practices of HIV sero-discordant couples and describes to what extent the desire to have children influences these sexual practices, in order to understand the implications for HIV transmission among discordant partners in Uganda. Our study is based on the socio-ecological model which recognizes the intertwined relationship existing between an individual and their environment. The model recognizes that whereas individuals are responsible for instituting and maintaining the lifestyle changes necessary to reduce risk and improve health, individual behavior is influenced by factors at individual, interpersonal, organizational, community, and public policy levels.11-13 Methods Study Setting Kampala, the capital city of Uganda is surrounded by Wakiso district and located in the central part of the country. The urban and peri-urban multi-cultural, multi-ethnic and diverse socio-economic groupings of Kampala's estimated 1.2 million inhabitants increases to two million people during the day. Wakiso is more rural and homogenous with about one million predominantly one ethnic group (77% baganda) (14). Kampala and Wakiso districts were purposefully selected from the 76 districts because they represent both large urban, peri-urban and rural populations; and have a high HIV prevalence of 3% among young people and 6-10% among adults1 Study participants We recruited study participants from four HIV treatment units in Kampala; The AIDS Support Organization (TASO)- Mulago, Infectious disease clinic-Mulago hospital (ISS clinic), Joint Clinical Research Centre (JCRC) and AIDS information centre (AIC) where couples are given quarterly educative workshops on HIV sero-discordance. The total population of discordant couples registered with TASO, JCRC, ISS clinic and AIC were respectively (113+50+35+150) = 348 couples as of June 2007. After taking care of client double or triple registration at the four study sites, we identified 150 couples that could meet our inclusion criteria of attending care at one of the four HIV care units; who had known their HIV status for more than six months, were not involved in any behavioural studies that may affect fertility decisions and with at least one person in the dyad below 40 years. The upper age limit was chosen because most Ugandan women will have completed childbearing by then.15 From June to December 2007, we consecutively recruited all HIV sero-discordant couples meeting the inclusion criteria until a total of 114 couples were recruited. We obtained informed consent to participate in the study. Between June and August 2007, a sub-set of 15 couples considered to be key knowledgeable respondents, were purposively selected from the quantitative study population to participate in in-depth interviews. The purpose of the study was repeatedly explained to them and a new informed consent was obtained before interview. Data Collection We used a structured questionnaire with both open and close ended questions to collect quantitative data on baseline characteristics (age, gender, education, occupation, religion, and number of living children), sexual and contraceptive behaviour, condom use in the last 12 months, any antiretroviral treatment (ART), knowledge of effectiveness of PMTCT and ART use, the role of stigma and significant others (family, friends and health workers) and whether their knowledge or significant others influenced their fertility decisions and condom use The in-depth interviews were conducted by the principal investigator (JB) with the 30 individuals making up 15 couples. Privacy was observed in all interview sessions that were held in English or Luganda (the local language mostly spoken) and audio tape-recorded. We used an unstructured interview guide with open-ended questions, which was back translated (16) to ensure consistency of meaning. We explored sexual practices of HIV sero-discordant couples; the influence of the desire to have children on sexual practices; the effect of the social networks and health systems; and the implications on HIV transmission among discordant couples. The study was approved by the Faculty of Medicine Research and Ethics Committee, National Council of Science and Technology (NCST), and the Karolinska Institutet, Sweden. Data analysis All quantitative data were entered using Epi Info version 3.4. Analyses were done using STATA version 10. We tested the association between the study variables: socio-demographic characteristics, desire to have children, perception that partner desires children, discussion with spouse and health workers about pregnancy, contraception and, number of children desired, use of ART and using knowledge about PMTCT to decide about childbearing, influence of others, disclosure to relatives, and the main study outcome, defined as consistent condom use. Following univariate and bivariate analysis, multivariate analysis was performed to adjust for confounding. We calculated odds ratios (OR) and 95% confidence intervals (CI) associated with consistent condom use. Only variables with a p-value < 0.20 in the bivariate analysis were included in a forward stepwise multiple logistic regression model and kept in the final model only if significantly associated with the outcome. All p-values were two-tailed at a significance level of 5%. The in-depth tape recorded interview data were transcribed by research assistants fluent in Luganda and translated to English. Reduction of data was done to remove vague, unclear or meaningless phrases and sentences. Using a thematic approach,17 categories within the texts were identified and grouped together to form the emerging themes. A random selection of the transcribed data was given to a qualitative research specialist from Makerere Institute of Social Research (SN) who independently analyzed the data, identified categories and themes. This analysis was compared with that done by the first author (JBK) to check for consistency and consensus on data interpretation. To improve validity and reliability of coding, frequent consultations with all authors was done. All authors reviewed the analysis with a "fresh eye". We used NVIVO 2 computer software package to assist in organizing the data. Lastly, the text was reviewed to identify quotes for illuminating the themes. Results The median age of the participants was 32 years (inter-quartile range 28-40 years), the women being on average 8 years younger than the men (median age 30 years vs 38 years respectively). Slightly more couples (52%) than had the man as the positive partner. A majority (86%) described their relationship as officially monogamous and the median duration of the union was 7 years (inter-quartile range 4 to 14 years). Most respondents were of low socio-economic status with 83% having secondary school education or less. A total of 212 (93%) participants had children and the median number of living children was 3 (inter-quartile range 1 to 5). More women than men (38% of the women and 29% of the men) had had children after knowing they were HIV positive. (Table 1) Fifty six percent (56%) of respondents used condoms consistently. Consistent condom use was less likely to occur among respondents who desired to have children. (Adjusted OR 0.51 (95%CI; 0.27, 0.98). In addition, having multiple sexual partners, and not having had discussions with health personnel about unwanted pregnancy and abortion, was also associated with inconsistent condom use, while respondents who were using contraception and had discussed pregnancy and HIV with health staff were more likely to use condoms consistently. The belief that ART gives high chances of an HIV negative child was associated with inconsistent condom use but not significantly so in multivariate analysis. (Table 2) Two broader themes emerged from the in-depth interviews and the qualitative analyses: Sexual practices for HIV prevention, and desire for children with the dilemma of condom use. Five types of sexual practices emerged under the first theme: 1) abstinence, 2) consistent condom use, 3) practicing unsafe sex, 4) alternative non-penetrative sexual practices and 5) seeking for HIV concordant partners, Five reasons for wanting a child despite HIV sero-discordance also emerged: 1) ensuring linage and posterity, 2) Concurrent relationships for childbearing, 3) pressure from relatives to reproduce, 4) securing the relationship through children, and 5) availability of antiretroviral therapy. In summary, the four major challenges that HIV sero-discordant couples struggle with include the fear of transmitting HIV infection to partner and child, the negative (more often the females) partner's lack of negotiating power for safer sex, failure of health systems to offer safe methods of reproduction, and whether to search for alternative sero-concordant partners, or concurrent partnerships. Sexual Practices for HIV Prevention The issue of preventing HIV transmission to negative partner was discussed in all the interviews and consistent condom use appeared to be a major struggle. Most respondents viewed prevention of HIV transmission as the most important thing in any discordant relationship and particularly challenging if the couple wanted children. To become pregnant, they must choose between risking HIV infection transmission or fulfilling their desire for children and most respondents therefore hesitated to go ahead with child bearing as illustrated below: "What is holding us is her status. We still fear transmission. I was only given one advice; to protect myself with condoms" (38 year-old negative male) "He brought the idea of another child; I brought the issue of HIV transmission. So we need advice. At first he would refuse condoms, I would refuse sex until he accepted condoms" (30 year-old negative female) Consistent condom use Almost all respondents suggested using condom as the best alternative available for protecting the negative partner. Most respondents reported commitment to use of condoms in the couple dyad. "We have been using condoms all the time" (24 year-old positive woman) "I make sure I put it on him myself." (24 year-old negative woman) However, some respondents said that there is a tendency to exaggerate the use of condoms to health personnel and that the actual frequency of safer sex was much less than that reported. "In our meetings and other fora, we tell health workers that we use condoms. But at home the story is different. Some men have totally failed to use condoms". (30 year-old positive female "Sex in discordant couples is interesting. It makes one laugh. Some discordant couples claim in public to be having sex, when at home they are abstaining. Others claim to use condoms when they have never touched it. …. We even lie that we are using condoms. `Do you use condoms, we say yes; has the condom ever burst? We say no; Have you ever removed the condom (had sex without condom)? We say no'; but when they examine us, they find some of us/our women pregnant." (37 year-old positive male) Practicing unsafe sex Failure to use condoms by discordant couples was discussed by many respondents, and in almost all interviews, lack of pleasure and sexual dysfunction emerged as the main reasons. Many felt forced to use them to protect their primary partners while they did not feel they had to use condoms outside marriage with other concurrent or temporary sexual partners. "I feel tired of condoms with my wife so when I go out for sex, I don't use them" (31 year- old positive male) Other reasons for non use included; relying on God's protection, myths about transmission like having strong blood and not believing the condom is sufficient to protect them as illustrated below: "You know how we do these things (sex). Do you also look for condom for the hands? You know the hands are involved in sex. They touch the fluids…. Some of us, the nature of our work, (manual) we get bruises in the hands. Are we going to put on gloves also?" (43 year- old negative male) Another important issue raised by some members was that health workers were explaining HIV discordance to be due to blood incompatibility and this was leading people to practice unsafe sex. "Doctor told my husband that my blood and his are incompatible. That's why we are discordant…. With my husband, condom use is irregular because he refuses. The doctor told him: "first show her love and when she wants then she won't get infected. If you force her, then you infect her" 23 year-negative female. Couple interaction and negotiation for condom use came out as a strong determinant for condom use and how sexual relations are managed. In most cases the man was the final decision maker and the woman had to obey. "My husband stopped me sleeping with him live [having sex without a condom]; that we should either abstain or use condoms. But later he chose to abstain. It is now three years" (23 year-old negative female) However, some men insisted that in issues of sex, women could have more decision-making power if they so wanted. "Every creature has its own power. So women have power over men when in love [in bed]. Even the toughest and most feared man can become stupid like a goat being taken for slaughter. Actually the goat struggles. He becomes like a sheep being taken for slaughter." (28 year-old positive male) Men's fear of condom-associated impotence was raised as one major reason for unsafe sex that could be driving the HIV epidemic. Most responded that if a man fears he may lose his erection, he will feel forced to rescue the situation by not using or removing the condom or else he will lose his status as a man. AM. If you lose an erection, can you perform? ... And at that point, you would rather die than lose face in front of a woman. That is why even the negative man can sleep with a positive woman live [without condom]. JBK. So in that case what do you do? AM. You take off the condom of course. (37 year-old positive male) Alternative non-penetrative sexual practices and abstinence To avoid infecting the partner, respondents used several alternatives of sexual fulfillment. Members who were abstaining sexually satisfy themselves with other sex objects simulating dildos or other non penetrative sexual practices. Those having sexual relations reported using other body parts like rubbing the penis in the palm of the hand, the navel, or underneath the partner's breast. A few others reported they were advised by peers to avoid things like romancing, deep kissing, touching themselves in private parts and touching the condom fluids. Having quick sex and not using force was said to be safe because it avoids friction. "Also if a man takes a long time without sex, then he will take a short time on sex and this is quite safe…… he won't take long and friction and bruising is less" (32 year-old negative female) Seeking for HIV concordant partners for sexual pleasure Some respondents admitted to not using condoms mainly because they wanted to enjoy sex and in almost all interviews, lack of pleasure emerged as one of the main reasons why people do not like condoms. Since many feel forced to use condoms to protect their primary partner, they seek other partners outside marriage to avoid using condoms. I have a sex partner outside marriage. Though I have never told him my status, it seems he is also positive but we both fear telling one another. ….My husband is always away and when he comes we use a condom. But my man friend outside marriage does not want to use condoms. (39 year-old positive female) Desire for Pregnancy with the Dilemma of Condom Use Respondents pointed out that practicing safer sex was hindered by the desire to have children. Many reported that HIV infected people have learned how to go around their status. Some respondents revealed that many discordant couples who had no children together separated to try new relationships in search for children. Those who remained together said that it is the children that bond the relationship. Some respondents expected their partners to leave after discordant test results. Some started doing all sorts of things to get children; like piercing condoms or even deceiving about own HIV status. Respondents voiced a need to urgently find ways of helping those who want children through medical research like they have done with antiretroviral therapy. "One time I told her I wanted to marry but it brought quarrels. She started demanding for more children... She started piercing condoms and when I discovered it she complained she wanted children". (43 year-old negative male) Ensuring lineage continuity and posterity The prestige of having own children, place in society, and the stigma of infertility all seem to drive many HIV infected people to want children. Many agreed that one's respect in society arises from having children. Many respondents held the view that many positive people avoided condom use or looked for negative partners to leave negative children behind to propagate the lineage. "One is respected to be a man if he left a child behind" (27 year-old negative male). "Introducing a condom is difficult because he wants children He has no children and yet he looks after mine like they are his. I look like a thief." (41 year- old positive female) Concurrent relationships for childbearing Both men and women with and without HIV were straying for concurrent relationships and in most cases, the negative younger men reported trying to look for negative partners to get more children. "I am the first born in our house. I can't stay with one child and I can't look after two wives. But we decided not to get more children with her. So I will look for a way of getting my three children. So I will get another wife." (29 year old negative male) One respondent who was contemplating other means of getting children talked of the frustration of having to deal with a husband who is positive and does not want children and would not even discuss the issue: "He doesn't want to talk about it at all... We used to talk about it. Even the child we have together, we agreed that we get it even though we had known our status. That he is positive and I am negative. But now each time I bring the issue up, he keeps quiet…… I have tried talking to him but he won't listen. Some people get children when their husbands don't want to have children. How do you think they get them?" (34 year-old negative female) Influence of significant others on couples' fertility decisions Culture and community interests emerged as very important in shaping fertility decisions of discordant couples. The expectations of society put pressure on individuals and often led them to behave in a certain way. One respondent recounted a story of an old woman going to funeral rites of women who died unmarried but had children to hear if the children left behind were her grand children because her late son did not leave a child at home. Significant others and health workers appeared to influence this group of discordant couples albeit in opposite directions; with relatives encouraging respondents to have children. "I have only one child who is also HIV positive. I talked with my uncle and he supported the idea of getting another child. So I remarried my current wife who is negative so that I get a negative child." (29 year-old positive male) "My mother told me to produce till my eggs are finished. That for her she got few children so I should not kill mine with contraception. Now I am told to use protector [condom] always." (24 year-old negative female) But health workers were reported as not supporting child bearing for HIV infected people. Indeed, the majority confirmed that they do not consult health workers because health workers do not want them to give birth. "Counselors would not be happy if my wife got pregnant. You would have broken the rules. They tell you to always put on the condom; how do you produce?" (38 year-old negative male) "Counselor, are you planning to give us programs to help us get children? …many want but they do not talk about it. They know you cannot help them so why talk. That is why you see many pregnant." (34 year-old negative female) However, all participants acknowledged that health workers could play an important role in helping discordant couples get children safely without infecting their partners but many expressed disappointment that health workers were not helping them enough or were not committed or had no way to assist them to get babies. One respondent has been referred for invitro fertilization (IVF), but the rest were just told to use condoms all the time. "I talked to counselors about getting pregnant but they have no way to assist us. They referred us to an expensive place for such a procedure". (29 year-old negative female) Securing the relationship through children Discussions on why people still have unsafe sex with their partners when they know they are discordant revealed that major factors are at play that override the fear of HIV transmission. Due to gender inequality and lack of communication between couples, there is fear of a "loose" partnership and would rather strengthen it with a child as illustrated below: "It's difficult to discuss children now. May be he will get them from out. I see he has his women there… we are like strangers to each other in the home" (27 year-old positive female) ".. Some negative partners force positive ones to have children. Like the child we have, I was forced by my wife who is negative. She was not threatened by my positive status, she insisted we get the one child we have together; though she has five others from two other men." (37 year-old positive male) "I knew she would leave me. We had no child together. So what would stop her from going?" (37 year-old positive male) The influence of Anti retroviral therapy (ART) on hope for children Having access to ART led to mixed responses. Most respondents said ART has helped people to live longer and healthier lives. Most of them saw it as a golden chance to get negative children but they still did not believe it reduced their own risk of being infected or the risk of infecting their partner. "It is positive women who benefit from ARVs to get negative babies. There are no ARVs to stop men from infecting women" (34 year-old negative female) "But it is him who is positive not me? Is there Nevirapine for men not to give us HIV? That is what I am waiting for. Otherwise, no more children." (30 year-old negative female) "Since I started my ARVs, my health has improved and I would get children if I had a man but he refused. Most of my friends have got pregnant again. And why not..? I see I am healthier than those other negative women of his…. but my husband refused and said I want to kill him (27 year-old positive female) Nonetheless, others chose not to have any more children but focussed on strategies for surviving longer to plan for their families instead. Others reasoned that since ART is for life, then most likely infectivity is also life long necessitating life long safe sex. "I no longer want to produce because I will be risking my life to death .....My lifespan will shorten." (28 year-old positive female) They tell us you take the drugs for life, which means no cure. So you should use condom for life.(37 year-old positive male) Discussion HIV sero-discordant couples were grappling with the dilemma of choosing between child bearing and HIV transmission to/from the partner. Only 56% stated they were consistently using condoms. Respondents with definite plans to have children were less likely to use condoms. Studies have reported variable desire for children in HIV positive people18-20 though they did not relate it to HIV infection risk reduction. Other studies show inconsistent commitment to condom use21, 22 even within discordant couples23. This study shows that negotiation for condom use and childbearing issues are closely interlinked and still a major hurdle in the daily lives of discordant couples. In addition, participants confessed that actual condom use is much less than what they normally report. This is supported by studies which found discrepant results of reported condom use and the findings of spermatozoa and Prostatic Specific Antigen in the vagina24, 25. The moral imperative may be to conform to the norms or risk being categorised as abnormal among one's social network. To avoid HIV infection transmission, some HIV infected/affected people, satisfy their sexual desires through alternative forms of sexual practices which do not allow pregnancy to occur. Those who perceive that they are at risk of HIV infection and are committed to condom use must trade the risk HIV transmission, or look for a sero-concordant partner, to get children. This study is among the first to report desire for children as the reason to look for another partner in HIV sero- discordant people. Studies from Africa suggest concurrent partnerships as a cultural norm26, 27 and the desire to have children will be regarded as a reason for HIV affected people to have concurrent partnerships. Nonetheless, this study finds that having multiple sexual partners was independently associated with not using condoms. Gender problems were prominent in this study with women struggling to negotiate for child bearing and condom use. Some despaired or devised other means like piercing condoms to get pregnant, but others vowed to dress their partners with condoms or have no sex if the man refused it. The struggle of getting children or refusing to have sex is mirrored in Kandyoti's work which shows that women, when faced with concrete constraints, make different strategies to maximize security and optimize life options with active or passive resistance28. Interestingly, no one was contemplating separation because of these hurdles. Whereas studies show men as the main decision makers in sexual and reproductive issues because of their differential decision making power within couple dyad29, 30, we found that some men believe women had power over men in sexual matters. Nevertheless, gender stereotypes, position of women in society, relationship power and internalised oppression hinders some women from taking charge 29, 31-33 even in situations where men believe women should. For example, when the condom leads to sexual dysfunction as reported in this study, the threat to his male ego makes him vulnerable and HIV transmission becomes secondary because he culturally must prove his manhood. Yet as the decision maker, his decision is often final. Decisions taken during these vulnerable situations could as well be seen as the driving force of the HIV epidemic. The findings of this study show that significant people in the lives of respondents play a big role in fertility decision making and position couples in a dilemma. Two groups emerged: The relatives who used traditional norms to encourage procreation; and the health workers who used medical knowledge to dissuade clients from childbearing. Uganda is a patrilineal society and its culture has several beliefs. One of them is: a man is considered to be man if he produces a child, especially a male to ensure lineage continuity. The prestige of having children, the position it puts one in society, and pressure from relatives may force HIV infected/affected people into childbearing. However, 86% of respondents thought their relatives would not want them pregnant if the relatives knew they (couple) had HIV. This may explain the dilemma of disclosure of HIV status. One third (34%) of respondents had not disclosed their sero status to their relatives. Another reason for bowing to pressure to have children in the absence of disclosure of their status was, culturally they had no other reason not to be having children, so they did not want to be considered culturally inappropriate or to be labeled infertile". This is consistent with studies which show that child bearing is a socio-cultural practice involving the person and a concern to other members of the person's social environment34. Similarly, women will be insecure in that family if they do not "give the man children" making procreation a power issue tilting in favor of the man. On the other hand, the respondents believed so much in the health workers and most of those who reported child wanted-ness also reported waiting for health workers to assist them. This gives health workers an untapped and great opportunity, and a unique position to support HIV positive clients to make responsive fertility decisions which would reduce HIV transmission. Study findings show that respondents who discussed with health workers about pregnancy and HIV were three times more likely to use condoms consistently. Nevertheless study findings reveal frustration of clients when some health workers avoid the question of child bearing. Other studies report similar findings of how health workers show negative attitude, lack of support and at most offer non prescriptive guidelines on reproductive choices for HIV infected/affected people. 35-38 Similarly, reproductive health policies in HIV/AIDS era are lagging behind the clients' needs. In Uganda, there is no policy for assisted reproduction for HIV affected people and the policy of prevention of mother to child transmission is not addressing discordant couple.39 It is recommended that sero-discordant couples who desire to have children should undergo assisted fertility treatment such as sperm washing, intra uterine insemination and in-vitro fertilization, to avoid HIV transmission to their partners 40, 41. However, only two private centers in Uganda are performing assisted fertility treatment and this is too expensive for the great majority in need. The average cost for one fertility treatment cycle is $ 5000. [Compare with an average salary of a school teacher of $ 200 per month]. Nonetheless, whereas infertility care is not a national priority, other options like reducing viral load by ART treatment before attempting conception, timed intercourse, and insemination to the positive females is not widely advised to HIV affected clients. This study also showed lack of adequate knowledge of ART and fertility. Whereas some saw it as a lease to life and a chance to get negative children, others especially the negative partners were skeptical and felt that they are still at risk of acquiring infection particularly if the man was positive. ART reduces the likelihood of HIV transmission to the partner; and health workers should be discussing its limitations and benefits with HIV infected people who desire to have children. In this study, respondents who believed ART increases chances of getting a negative child were not using condoms. ART has only been available for five years and this may explain the lack of knowledge in both clients and health workers. An unexpected finding was that HIV negative partners had a fatalistic attitude and were ready to risk acquiring HIV infection at the expense of getting children. This implies that the desire for children supersedes the perception of the likelihood of HIV transmission; or the perception of the risk of transmission is blurred by myths, misconceptions and lack of accurate knowledge about HIV-discordance hence doubts about the need for risk reduction3. Factors that might affect the risk of HIV transmission including for example male circumcision, ART use, viral load and other sexually transmitted diseases 42, 43 may be taken into account by the individual health worker when estimating the risk of infection but it is very dissatisfying indeed that some health workers make obviously erroneous statements regarding incompatible blood etc . This coupled with other myths and misconceptions gives the person a false sense of security and leads to laxity in preventive measures as they struggle with the option of not using the condom to have children. The findings of this study show enormous implications regarding sexual practices and child wanted-ness; and reveal that HIV infection has changed the context of sexuality and fertility decision making among sero-discordant couples. As the socio-ecological model, our study shows that an individual's behaviour and decisions are influenced by one's environment with a varied direction of effect. It is therefore unrealistic to expect individuals to change behavior or make responsive decisions when the constraints at in their environment are insurmountable. We need to study in depth to understand the issues surrounding safe sex, child wantedness and strategies needed to assist couples have children with minimal risk of HIV transmission to the negative partner. Specific programs modified to the needs of discordant couples and targeting health systems, families, communities and the society, should be developed and implemented. Health workers should be empowered with knowledge about sexuality and fertility control so that they assist their clients in fertility decision making in the era of ART. Competing interests None declared. The views expressed here are those of the authors and do not necessarily represent their institutions of affiliation. Authors' contributions JBK and FMM conceived the idea, all authors participated in the design of the study, JBK did data collection, and all did data analysis, and read and approved the manuscript. Acknowledgements SIDA-SAREC through Makerere University-University-Karolinska Institute Research Collaboration for funding this study, the faculty of medicine research and ethics committee, TASO, ISS-Clinic, JCRC, AIC for the support and accepting to utilize their premises, HIV sero-discordant couples who accepted to participate in the study, the research assistants Ms Atwine Patience and Mr. Namanya Hilary who participated in data collection. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09002t2.jpg] [hs09002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}