 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 1, March, 2009, pp. 19-25 Potential risk of HIV transmission in barbering practice among professional barbers in Ibadan, Nigeria Oyedunni S. Arulogun and Moses O. Adesoro Department of Health Promotion and Education, College of Medicine, University of Ibadan, Ibadan, Nigeria Code Number: hs09004 Abstract Background: There is a growing concern that barbering procedures could create opportunities for HIV transmission. However,
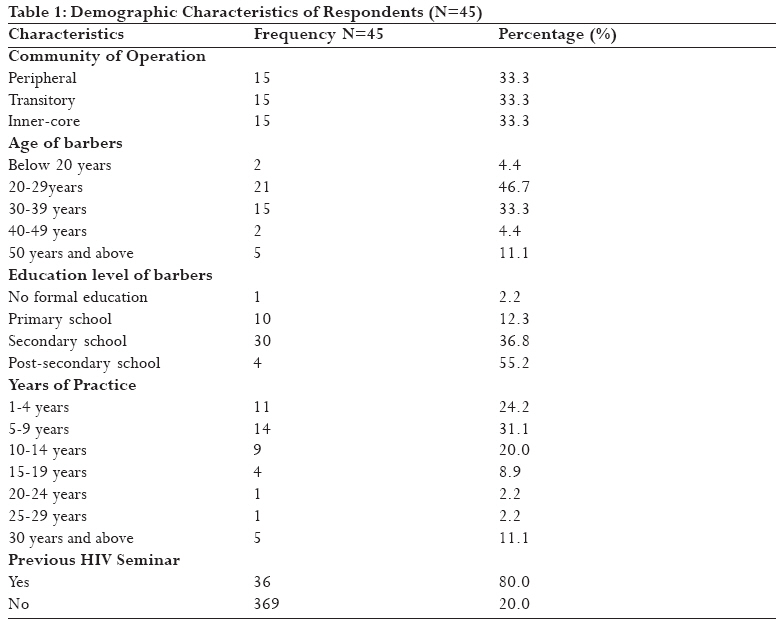
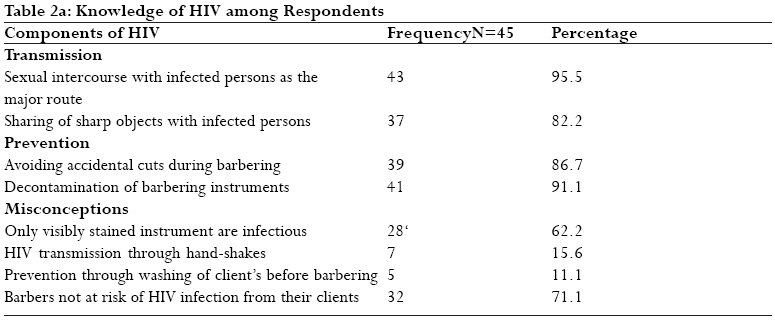
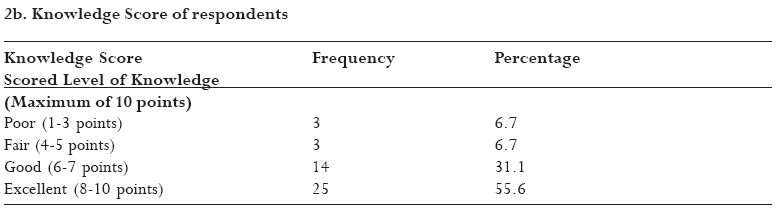
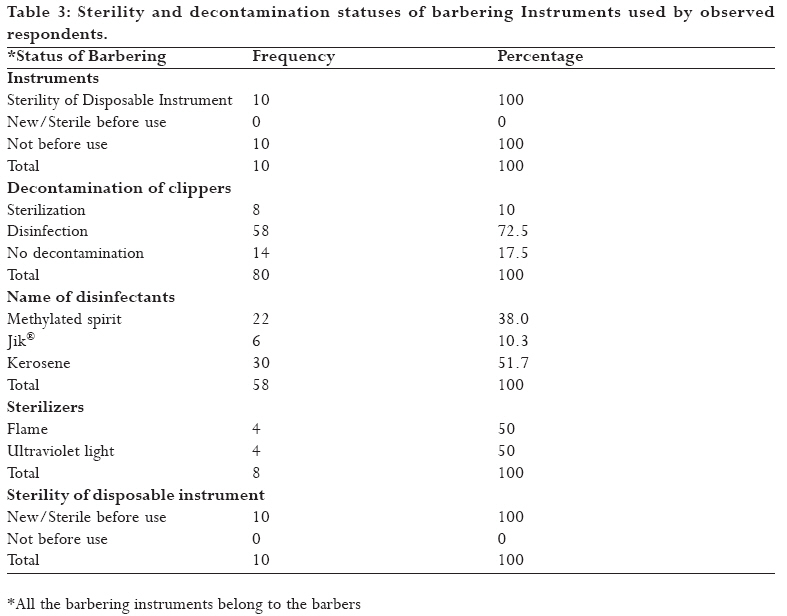
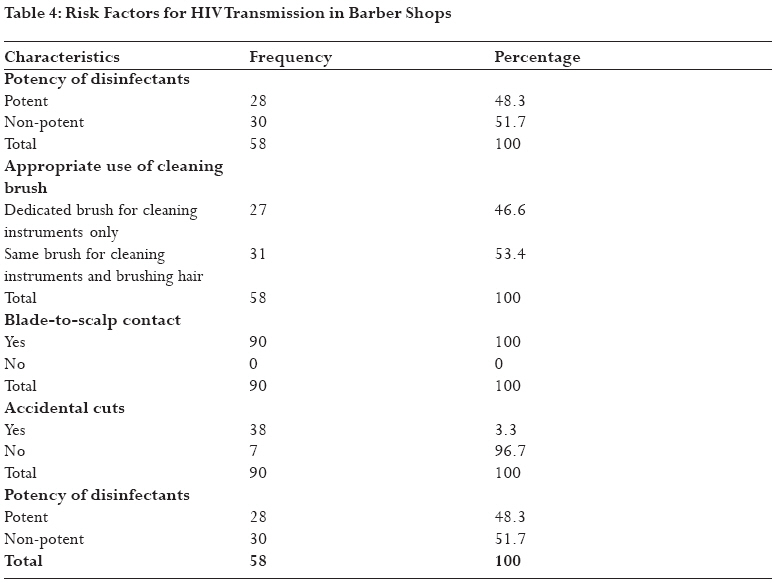
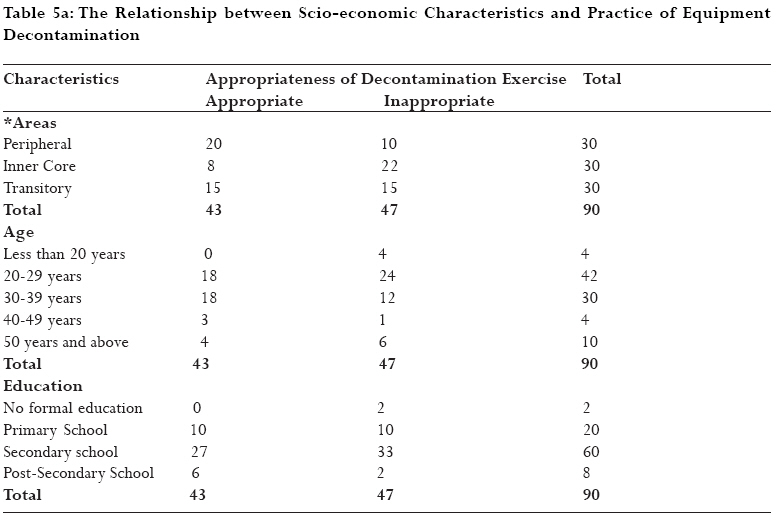
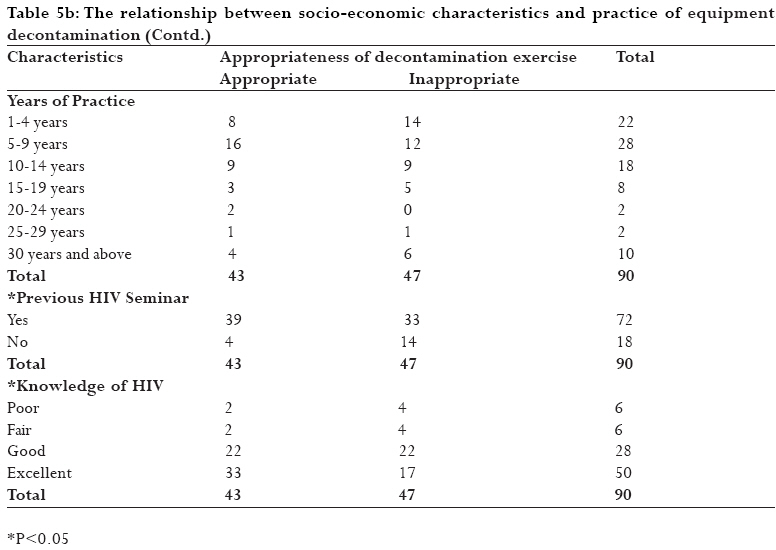
little is known about Nigerian barbers' practices relating to the prevention of HIV. Introduction HIV/AIDS still remains a major public health problem all over the world, particularly in Nigeria where it has caused incalculable human suffering, social and cultural disruption and huge economical loss. There were about 220,000 deaths from AIDS and 930,000 AIDS orphans living in Nigeria in 2005 alone.1. Nigeria is expected to spend $260-$390/person as budgetary allocation to HIV/AIDS control yearly2, definitely at the expense of other developmental projects. Though the country's HIV prevalence rate has dropped from 5.8% in 2001 to 4.4% in the last sentinel survey carried out in 2005, some States and sites still have explosive prevalence rates. For example, Benue State and Iquita-oron in Akwa-Ibom state recorded 10% and 14.7% prevalence rates respectivel.3 Prevention is the only viable way to control HIV spread, as there is no cure for the infection presently. In Nigeria, efforts have focused mainly on prevention of HIV through sex, blood transfusion and mother-to-child transmission. This must have been informed by the fact that more than ninety percent of HIV/AIDS transmissions occur through the combination of these routes.4 However, HIV transmission through sharing of non-sterile sharp instruments such as those used for barbering, circumcision, facial scarification, incision, tattooing, ear perforation, bloodletting, injections and acupuncture have always been vaguely classified as `others' and given less attention in the campaign against the spread of HIV. Barbers are cosmetic workers that undertake skin-piercing practices involving re-useable sharp instruments, which present risks for transmission of HIV and other blood-borne pathogens from one client to the other. Though barbers do not carry out procedures that deliberately penetrate the skin, the procedures can inadvertently damage the skin through abrasion or minor accidental cuts.5 A simple nick caused by clipper or razor blade is enough for infection to occur. 6 Due to the lipid envelope that protects HIV from dehydration, the virus can survive on the surfaces of barbering instruments for a period long enough for transmission to occur, particularly in commercial barber shops. 7 Specific HIV-risks of barbering procedures relating to HIV transmission have been documented in Nigeria and other African and Asian countries. 7,8,9,10,11 These authors reported incidences of accidental cuts on scalps and poor hygiene practices, including low disinfection rates of re-useable instruments. However no study seems to have documented the extent and effectiveness of hygiene practices of the barbers. Proper, effective and consistent decontamination of barbering instruments is important in preventing HIV transmission in barber shops. Surgically, barbering instruments are semi-critical instruments that come into contact with damaged non-intact skin and require at least intermediate-level disinfection to make them safe.12 Methods and agents that have been designed to inactivate other viruses such as hepatitis B are also effective for HIV. These agents include alcohol (ethanol, isopropyl), chlorine (Sodium hypochlorate), phenolic compounds, quaternary ammonium compounds, iodine and iodophores. HIV on barbering instruments can also be inactivated by using sterilizing agents such as flame, dry heat, cream and ultra-violet light.13 HIV infected persons despite being asymptomatic, are infective at all stages of infection. Therefore, when dealing with all clients, barbering instruments must always be disinfected or sterilized to minimize the risk of HIV transmission. The concept of universal precaution considers all blood and body fluids to be potentially infectious and all invasive instruments to be potentially contaminated if already used.14 The responsibility to keep instruments free of infective agents lies on the barbers. The prediction that Nigeria will have 10-15million HIV/AIDS cases by the year 201015 may be fulfilled if barbering and other traditional skin-piercing procedures are not given better attention than they are given presently. This study, therefore, was aimed at assessing the professional practices of barbers relating to HIV transmission. Methods The study was a descriptive survey carried out among commercial barbers in Ibadan Southwest Local Government Area (LGA), one of the five LGAs that make up Ibadan Metropolis, southwestern Nigeria. The site was chosen because of its categorization into inner core, transitory and peripheral communities, which represent various socio-economic status of Nigeria communities. The site is located within the rain forest belt of western Nigeria, about 150km from Lagos and 659km from Abuja, the Nigeria Federal capital city. Three communities were randomly selected from the stratified communities and fifteen barber shops were systematically selected from each of them using a sampling interval of two. Trained research assistants, with the authors supervising, collected data by direct observation using the pre-tested and validated checklist. Prior to this, advocacy visits were made to the executive members of Barbers' Union to intimate them with the purpose of the study and seek for their support. Verbal informed consents of the barbers' union at both the state and zonal levels as well as that of the individual participating barbers were secured before the observation exercise. The shops were visited between 4pm and 6pm on weekdays and between 12noon and 6pm on Saturdays. These periods were the busy periods when barbering sessions could be witnessed. In each shop, two barbering sessions, with at least one session involving the use of reusable instrument, were observed. For effectiveness, only one session was observed wherever more than one session were going on simultaneously and the first session to start in the presence of the observer was taken. The pre-tested observation checklist used for data collection was designed to record the instruments used; type of decontamination; description of equipment decontamination procedures; names and certification of germicidal potency of decontaminant in terms of composition, concentration and expiration. Other behaviours observed included incidences of zero-cut hairstyles and accidental cuts as well as actions taken on client and instrument on such occasions. With the exception of the verification of decontaminants, other observations were done unobtrusively. Data generated were processed and analyzed using the SPSS (version 12.0) to generate frequencies, descriptive statistics and Chi square tests. Results Demographic Characteristics of Respondents The ninety barbering sessions observed were carried out by 45 barbers. Table 1 shows the demographic and professional characteristics of the barbers, which were all males. The mean age was 36(10.2) years. There was preponderance (30 or 66.7%) of respondents that had secondary school education. The mode of learning of the art of barbering in the area is through apprenticeship spanning 2.0±0.8 years. All the barbers were aware of HIV/AIDS and they had a mean knowledge score of 7.2(±2.2) out of a maximum score of 10. Thirty-seven (84.1%) knew that HIV could be transmitted by sharing non-sterile sharp instruments. For the prevention of HIV in barber shops, avoiding accidental cuts and equipment decontamination were mentioned by 39 (86.7%) and 41 (93.2%) of the respondents respectively. Twenty-eight (62.2%) did not know barbers were at risk of HIV infection from their clients (Tables 2a and 2b). Out of the 90 barbering sessions observed, razor blades were used in 10 (11.1%), manual clippers in 8 (8.9%) and electric clippers used in 72 (80%) of the sessions. Table 3 shows the sterility and decontamination statuses of these barbering instruments. All the razor blades used as the main instruments were used as new and disposed thereafter. The clippers were sterilized in 8 (10%) and disinfected in 58 (72.5%) of the sessions while no decontamination was carried out in 14 (17.5%) of the sessions. Out of the 58 sessions that involved disinfections, 22 (38%) used Methylated spirit, 30 (51.7%) used Kerosene and 6 (10.3%) used Jik®. Hand-held flame and Ultra-violet light sterilizer were used each in 50% of the session for the sterilization. The sterilizers were found to be functional and operated according to specifications (Table 3). The risk factors that encouraged HIV transmission in the observed sessions included inappropriate disinfections, which involved the use of disinfectants that could not inactivate HIV and using same brush for cleaning instrument and brushing hair by 30 (51.7%) and 31 (53.4%) respectively. Others were blade-to-scalp contact and accidental cuts observed in all (100%) and 3 (3.3%) of the sessions respectively. In addition, no first-aid action was taken on the victims and the instruments involved in the accidental cuts (Table 4). The appropriateness of the decontamination processes was cross-tabulated with the status of their location, age, education, years of professional practice, experience of previous HIV training and knowledge of HIV. Chi-square statistic was used to test for significance at 95% confidence interval (p<0.05). The location, previous HIV training and knowledge of HIV were found to influence the decontamination of barbering equipment (Tables 5a and 5b). Those in more enlightened communities, beneficiaries of training on HIV and good knowledge of HIV are more likely to practice appropriate decontamination procedure. Discussion This study shows that the frequency and quality of instrument decontamination practices of the respondents in relation to HIV prevention is not satisfactory. Though majority of the respondents appeared to observe decontamination either as disinfection or sterilization, more than half of the disinfections were inappropriately done. For example, kerosene, which cannot inactivate HIV, was used in majority of the disinfections and brushes used in cleaning instruments were also used to brush hair in the same barbering procedure, with the possibility of recontamination. A list of standard disinfectants recommended for use against HIV in hospital and personal care settings excluded kerosene. 12 In addition, studies on germicidal activities of kerosene showed that it could only decontaminate fungi, particularly the Candida genus, it has no inhibiting effects on bacteria and viruses, HIV inclusive. 16 The Authors specifically underscored the use of kerosene as disinfectant on barbering instruments. This implies that the seemingly high disinfection rate among the respondents may only amount to a false sense of security to the clients and general public. This finding is similar to some previous studies on barbers' practices. 10,11 However the finding differs from a study that reported a high sterilization rate among barbers in some parts of Oyo state, Nigeria.7 The study, probably, was not critical of the decontamination procedures. The socio-economic status of the barbers' location seems to have effect on the decontamination practice. Barbers in the high-class Peripheral areas were more likely to practice appropriate equipment decontamination than those from lower-class Inner-core areas as predicted by a previous study.5 Inappropriate practices may be due to lack of practical knowledge about decontamination and potency of disinfectants. The infrequent rates may be attributable to the asymptomatic nature of sero-positive individuals. Health and personal care workers are known to adhere strictly to decontamination guidelines for invasive instruments when used on clients known to be HIV-positive and may not follow the rules rigorously when dealing with instruments used on "routine" clients.17 However the principle of `Universal precautions' considers all blood and body fluids to be potentially infectious and all invasive instruments to be potentially contaminated. 14 Another possible reason for the poor HIV-prevention practice may be the lack of strict control measures and monitoring by relevant bodies. Unlike in developed countries where activities of barbers are regulated through a comprehensive training, licensing and monitoring programmes13, Nigerian Government has not given any noticeable attention to barbers and their activities. Skin damage is the prerequisite for inoculation of the scalp with HIV to occur. It allows for the penetration of the skin by barbering instruments and exposes the circulatory system to infection. Skin damage occurs during barbering either as an accidental cut or abrasion as a result of blade-to-skin contact, or both. Blade-to-scalp contact often occur during hair shaping, shaving and zero-hair cutting involving non-use of detachable plastic comb [18]. In this study, all the sessions involved procedures like hair-shaping, hair-shaving and zero-cuts. All these procedures encouraged blade-to-skin contact and consequently, skin abrasion and cuts. Minor cuts during barbering seem to have become a common accident as it has variously been reported in previous studies. 7, 8 It may be as a result of improper handling of the instruments. Apart from aiding infection, improper handling of barbering instruments has also been linked to the high and increasing prevalence of Acne Keloidalis Nuchae (AKN) among the patrons of barber shops in Nigeria. 19 The non-use of detachable plastic combs on clippers during barbering may be attributed to the prevailing zero-cut hairstyles in the population. Barbering is a tool for manifesting fashion. 20 This unavoidably leads to skin abrasions and accidental cuts, if proper care is not taken. Conclusion This study has revealed that barbering procedures in Nigeria, particularly in the study area, present the risk for HIV transmission through the use of non-potent disinfectants and improper handling of sharp instruments. The same invasive instruments were used on asymptomatic sero-positive and uninfected individuals. In addition, there were blade-to-scalp contacts in all the sessions. Therefore, barbers could serve as a potential core group for indirect transmission of HIV in the general population. This should be of great concern and calls for prompt and target-group oriented interventions. To effectively control HIV/AIDS in Nigeria, a comprehensive approach has to be adopted with the involvement of all relevant sectors and groups. Barbers should not be left out. It is therefore recommended that enough attention should be given to hygiene practices in barbershops through routine supervision and monitoring by agencies of the government. In addition, practical-oriented training should be organized for the barbers on equipment decontamination with emphasis on the use of correct procedure and potent decontaminant. All these can be organized through the barbers' union using peer education' approach. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09004t4.jpg] [hs09004t2b.jpg] [hs09004t5b.jpg] [hs09004t2a.jpg] [hs09004t1.jpg] [hs09004t5a.jpg] [hs09004t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}