 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 2, June, 2009, pp. 82-91 Correlates of misperceptions in HIV knowledge and attitude towards People Living With HIV/AIDS (PLWHAs) among in-school and out-of-school adolescents in Ghana. Anthony M. Sallar Ohio University, School of Public Health Sciences and Professions, Grover Center E335, Athens, OH 45701 Code Number: hs09016 Abstract Background: A quarter century into the HIV pandemic, knowledge about sexual transmission and sharing of needles remain
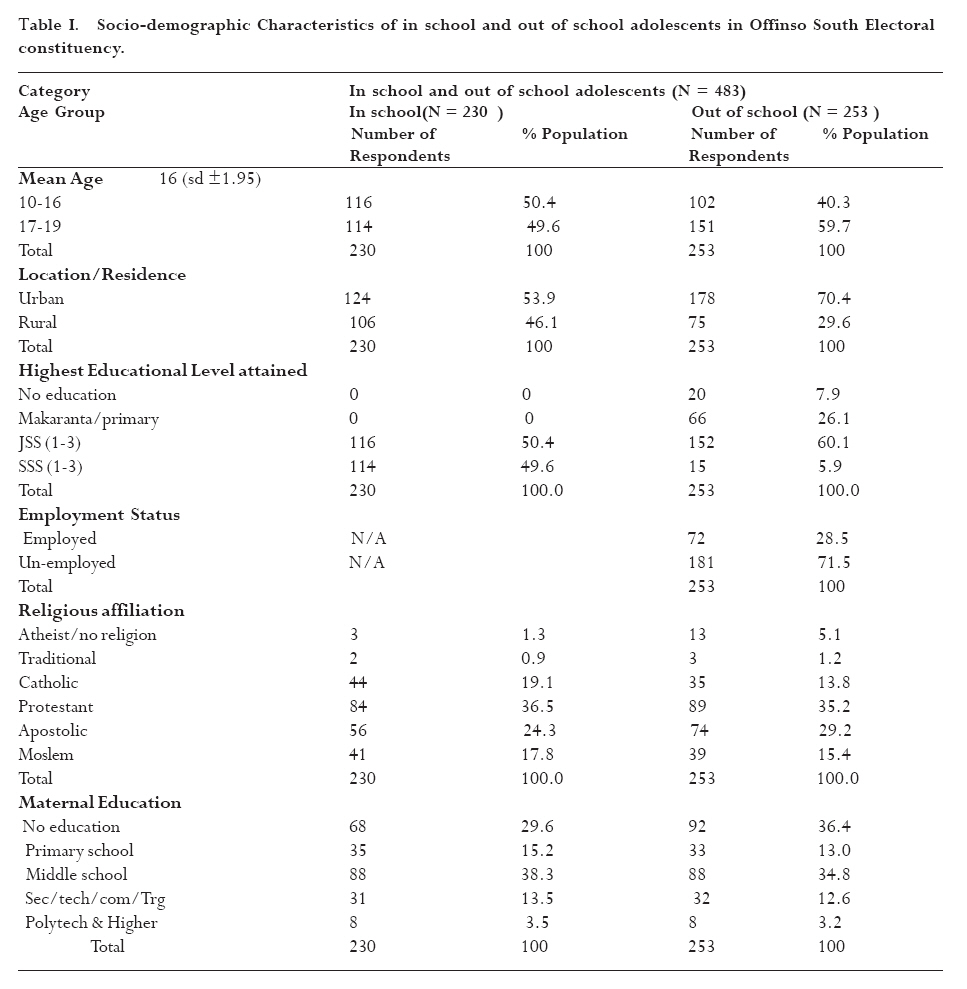
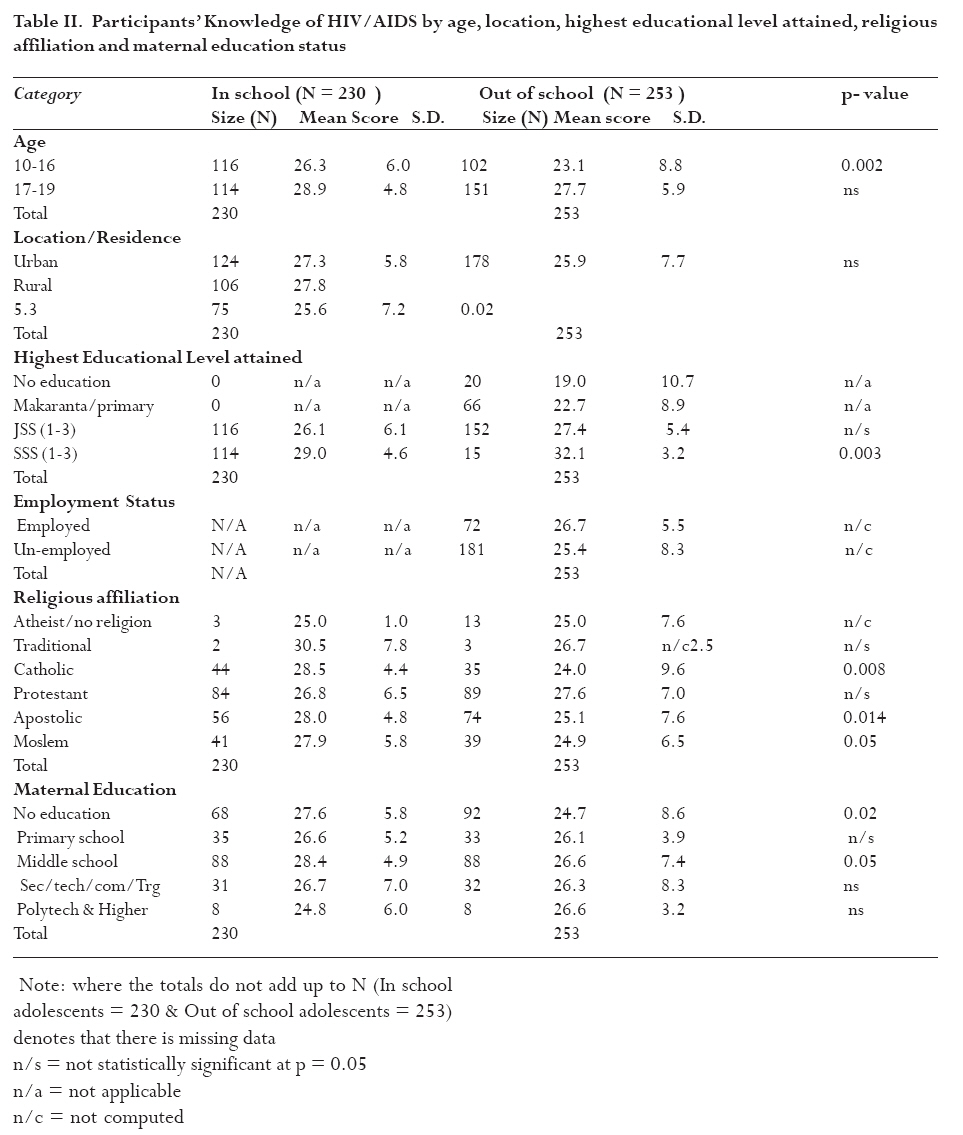
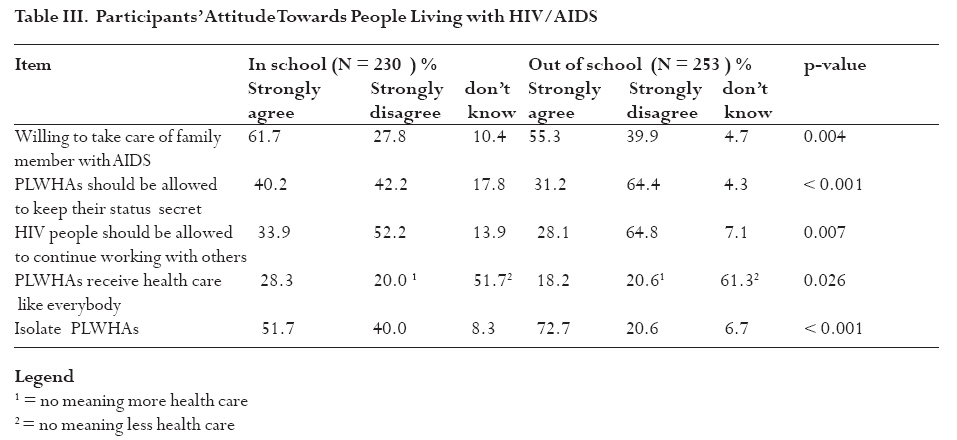
high just as misperceptions relating to casual contact. Introduction Since its inception in the early 1980s, HIV continues to have a tremendous effect in the world. Nowhere is this felt more than in sub Saharan Africa where the devastating tremendous impact has not only been on morbidity and mortality, but also on family structure, social organizations, and economics. The first case of AIDS was reported in Ghana in March 1986 with 43 cases1. The Ghana Ministry of Health reported that HIV prevalence has continued to increase and by 2005 there were 58,000 cumulative confirmed cases with adult prevalence estimated at 2.3%2. By 2006, approximately 320,000 people were estimated to have the virus with only 7% of HIV-infected women and men receiving antiretroviral therapy3. It has been demonstrated that increased knowledge about AIDS is not a predictor for behavioural change4, 5, 6, 7 although knowledge about the disease is a prerequisite for change8. However, knowledge of HIV and other STIs have been lacking among adolescents in Ghana and elsewhere. According to UNAIDS, only 44% of men and 38% of women aged 15 to 24 in Ghana correctly identify ways to prevent HIV3. In spite of the above, of those aged 15-24 years, 3.9% of men and 7.4% of women had sexual intercourse and the percentage of young people aged 15 24 years who used condom the last time they had sex with a casual partner was 52.0% (men) and 33.0% (female)3. This has implications for propagation of HIV because almost 41.3% of Ghana's population of 22 million is aged 15 years or less. The study was conducted among unmarried in-school and out-of -school adolescents living in the Ashanti region of Ghana. Ghana has 10 administrative regions and using the 2000 census data, the Ashanti Region ranks the highest in Ghana in terms of AIDS cases with the rate of 27.9/1,000 people.. The primary objective of the study was to assess HIV knowledge and misperceptions that may act as barriers in HIV prevention, and adolescent attitude towards People Living with AIDS (PLWHAs). Discrimination against PLWHA impacts on testing since individuals may be overly concerned about who will see their test results and what can happen to them especially when there is no universal ARV treatment. Negative attitude towards PLWHAs can be manifested in different forms including stigma and disagreement regarding location of a residential care in the neighborhood [9] or discrimination at the work place. This study does not limit itself to high school or college students but also includes out-of-school adolescents because of many reasons. 1) Survey research regarding AIDS in the young adult population in sub-Saharan Africa has been conducted with those in primary school10, 11 in secondary school12-17 and those in college18, 19, 20, 4, 21. There are very limited studies in the sub continent as well as in Ghana concerning out of school adolescents 22, 23 except street children24, 25 and adolescents gathered at truck stops26. Adolescents connect with other adolescents (students or non-students), parents, and others. School is only one of the settings in which they congregate, so restricting studies to adolescents who are in school ignores issues and problems pertinent to the out-of school adolescents. 2) Furthermore, in developing countries, there are lower school attendance and higher illiteracy rates than in developed countries. Because of the above reasons, restricting research to adolescents who are only in school may not provide enough evidence regarding the dynamics at play and may provide biased results that cannot be generalized to the adolescent population at large in Ghana. It was hypothesized that 1) HIV knowledge will be lower for out-of-school adolescents compared to those who are in school 2) Those who scored higher on misperceptions on HIV knowledge are more likely to have negative attitude towards PLWHAs 3) Out of school adolescents are more likely to have negative attitude toward PLWHAs compared to their counterparts who are in school. Methods The study was a cross-sectional survey of unmarried in-school and out-of-school adolescents aged 10-19 years residing in Offinso South electoral constituency of the Ashanti region of Ghana. Those aged 10-11 years were included in the sample because there were some in the junior secondary schools. They however formed only 1.2% of the study sample. In-school adolescents were defined as those who were enrolled in secondary school at the time of the study and out-of-school adolescents were those who had never been to school, had only an elementary school education and had not continued, or had dropped out of secondary school. The survey instrument was organized to elicit information on the following issues: 1) General demographic information (age, gender, residency, education, religion, parental education, and occupation); 2) Knowledge of HIV/AIDS; and 3) Attitude toward PLWHAs. The AIDS knowledge module consisted of 42 items divided into three sections (transmission, prevention, and risk reduction). The questions had possible choices of "True, False, and Don't Know". The "Don't Know" as an option was included to reduce the probability of guessing, as guessing causes some variation in performance from item to item, which tends to lower the test reliability27. Respondents were asked questions whether HIV could be transmitted via sexual intercourse, sharing needles or sharps, blood transfusion, vertical transmission, mosquito/insect bites, shaking hands or hugging HIV+ person. Attitude toward PLWHAs was assessed with five key questions on a five point Likert Scale, ranging from 1 (Strongly Disagree/Very Unlikely) to 5 (Strongly Agree/Most Likely). The survey instrument was pilot tested in a district with demographic and cultural characteristics similar to the research site. Initially the English version of the questionnaire was pre-tested on 20 students, then on additional 15, then another 10. The reason for this approach was that it made each testing unique and resulted in three episodes of testing rather than a single test on 45 students. The questionnaire administered to out-of-school adolescents was translated from English into the local language (Twi) and then translated back into English by different people in order to determine whether the translations were consistent and to ensure that the meaning of all survey items had been preserved. The translation was done to remove bias by ensuring that the research assistants did not give different interpretations of the questions as well as the answers when administering to out-of school adolescents. The translated questionnaires were again pilot tested on 20 out-of-school adolescents (10 boys and 10 girls) by four interviewers in areas where the survey instrument was not going to be administered. One month after pre-testing in schools, the translated versions were pre-tested on 15 (30%) of the same students in one-on-one interviews in order to determine whether significant differences would be found between self-administration in English and one-on-one administration in the local dialect. No major differences were observed between responses given by the students on key variables such as ever having had sex, condom use and number of sexual partners as they all yielded reliability coefficients of 0.85 or higher between the two versions. The internal consistency reliability coefficients for HIV knowledge and attitude towards condoms components of the instrument, respectively, yielded Cronbach's alphas of 0.92 and 0.94, and were high enough to meet the study criteria. In-school adolescents were divided into junior secondary (JSS) and senior secondary (SSS). A listing of all schools and enrollment in the constituency was obtained from the Statistical Division of the District Headquarters of the Ministry of Education. The schools were then selected to ensure the representation of rural and urban schools on the 60%-40% distribution respectively. Samples from each school were proportionally weighted to represent the total student population in the study area. In each school, the enrolment register per class, which has the list of all students in alphabetical order, was used to select study subjects by using a random number table28. Since there was no list available for selecting out-of-school participants, they were selected from a random sample of households in each ward of the district utilizing neighborhood demarcations. None of the youth live in "informal" accommodation, makeshift housing, or group type of homes since there are no street kids or homelessness in the study area. Where a selected household had two out-of-school adolescents, only one was chosen by a toss of a coin. If the residence had more than two out-of-school adolescents, the choice was made by throwing a die. No teachers or parents were present during administration of the questionnaire. There was no problem obtaining informed consent from parents since the traditional authorities, health administrators, and politicians were aware of the study and had informed the citizenry about the need to participate. The questionnaire was administered in order to ensure confidentiality, anonymity and privacy. Each participant was assured of confidentiality and anonymity. They were informed that participation was entirely voluntary, they were at liberty to opt out of the study at any time, and refusal to take part or complete the questionnaire would not jeopardize the participant's schooling or continued stay in the community. Data analysis The data were entered in a Spreadsheet and later exported to SPSS version 13 for analysis [29]. Descriptive statistics were used to describe demographic characteristics and knowledge of HIV. In testing the hypotheses, data were analyzed by contingency table analysis except for t tests as appropriate for continuous data. Chi Square (X2) tests were used for differences in proportions and for categorical variables. The Fisher's exact test was used when frequencies were less than five. All statistical tests were two-tailed and alpha = 0.05 or less was considered significant. In computing total knowledge score, all correct responses were scored as one (1) and incorrect and "don't know" responses were scored as zero. Scores were computed by summing up all correct responses to generate an overall score for each study participant. The scores were categorized into three segments: those scoring 50% or less were classified as having "low" HIV/AIDS knowledge, those scoring 51% to 74% were classified as "intermediate" or "medium" knowledge, and those scoring 75% or more were deemed to have "high" knowledge. To identify specific gaps in knowledge, an analysis was undertaken on each question to find out those questions which were consistently answered correctly and/or incorrectly. Attitudinal items on PLWHAs to which the subjects responded utilized a five point Likert Scale, ranging from 1 (Strongly Disagree/Very Unlikely) to 5 (Strongly Agree/Most Likely) with the midpoints representing ambivalent responses. Thus, the score of "1" represents low tolerance or unfavorable attitude while a score of `5" indicates a high tolerance or favorable attitudes/feelings towards PLWHAs. During the analysis phase the scores were collapsed into 3 categories (for example, "strongly agree" and "agree" as one category, strongly disagree and disagree as another category). Chi-square analysis was used to examine the relationship between AIDS knowledge (relating to misperceptions involving transmissions through casual contact) and each of the 5 questions assessing negative attitude toward PLWHAs. ResultsSocio-demographic information Overall, 488 participants, aged 10-19, were interviewed. Five participants were excluded from analysis because they had exceeded the age limit. All the in-school adolescents who were sampled agreed to participate. Three of the out-of-school adolescents refused to participate because of prior commitments. This yielded an overall response rate of 99.4%. There were 262 males (54.2%) and 221 females (45.8%), with one hundred and eighty one (37.5%) residing in rural and 302 (62.5%) residing in urban areas. Of the study's 483 participants, 230 (47.6%) were currently in school and 253 (52.4%) were not in school. Of those not in school, 28.5% were currently employed or learning a trade and 71.1% were unemployed and not learning a trade. The mean age of the respondents was 16.6 years (s.d. ± 1.95). Those classified as young adolescents (10-16 years) constituted 45.1% and those considered old adolescents (17-19 years) were 54.9% of the study population. Demographic characteristics of the study participants classified between in-school and out of school adolescents are presented in Table 1. HIV/AIDS Knowledge and Understanding Overall, 94% of the study's participants had heard about AIDS, but only 65.8% about HIV. The difference between hearing about AIDS and HIV may be due to the fact that in Ghana, AIDS is used rather than HIV to describe the infection as well as disease. Of the 42 questions which addressed HIV knowledge, the scores ranged from 0 to 38 (mean score = 26.64; sd: ± 6.74; median score = 28) with only 6 participants scoring 37 and above. About 17.5% (n = 85) obtained scores which could be classified as having low knowledge (0% to 50%) while 59% (n = 285) scored between 51% and 74% (classified as having medium knowledge); and 23.4% (n = 113) can be deemed to have high knowledge. The main sources of information for acquiring HIV knowledge in this population were the radio (86.1%), television (84.9 %), doctors/healthcare workers (81.6%), schools (77.8%), friends/acquaintances (72.3%), community agencies (70.2%), family members such as aunts, cousins, and other relatives (67.3%), books (63.1%), and newspapers/magazines (55.0%). About one out of every ten (12.4%) participants indicated that they heard somebody could cure AIDS. Of these (n = 60), 42.4% indicated medical doctors, 35.6% indicated herbalists/traditional healers, 16.9% mentioned spiritualists/Osofos (a local name for priests of charismatic churches) and 5.1% stated mallams (spiritualists of the Moslem faith) could cure AIDS. Furthermore, 29% of the respondents expressed their belief in fate as the ultimate determining factor in whether or not one contracts HIV/AIDS. In addition, 43.7% of the respondents believed that no matter what some people do, they would never get sick. Greater than majority (80%) of the participants knew that HIV could be transmitted via semen, vaginal fluids, and blood and that a healthy person who has HIV can pass the virus to others unless protective barriers are used (72.2%). However, only 72.2% indicated that breast milk from a mother could infect an infant with 11.4% stating they "don't know". Sexual abstinence was mentioned by 78.1% as a means of preventing AIDS. Other means mentioned were: the use of condoms during sex (72.7%), fidelity to the same partner (72.5%), not sharing needles (76.4%), reduction in the number of sexual partners (56.7%), while one in four (25.3%) incorrectly indicated that oral contraceptive use could serve as a protection against HIV. To determine whether participants who recognised the fatality of AIDS had translated this knowledge in behavioural change, the following question was asked: "Since you first heard about AIDS, have you done anything to avoid catching the virus yourself or to prevent someone else from getting it from you?" Almost three out of every four participants (72.2%) responded in the affirmative, with 20.1% indicating that the changes started within the last 12 months, while 79.7% indicated that they had started the changes more than a year ago. To identify specific gaps in knowledge, an analysis was undertaken on each question to find out those questions which were consistently answered correctly and/or incorrectly. The analysis demonstrates that there were misperceptions as shown by the responses. "You can tell by looking at a person that he or she has HIV or AIDS" elicited a combined "true" and "don't know" responses up to 55.6%. Similarly, participants inaccurately were of the view that "Birth control pills protect women from contracting HIV infection" with 25.3% reporting it as true, and 18.8% indicating they "don't know". Similarly 20.9% indicated that "People can protect themselves from HIV/AIDS by using contraceptive foam or jelly" with 22.2% indicating they "don't know". Also, almost 2 out of 5 participants (38.9%) indicated that "Kissing/contact with saliva is a way of contracting HIV" with 17.6% indicating they "don't know". More than one half (56.5%) of the respondents believed that "A person can get HIV by donating blood" with 10.4% indicating they "don't know" Table 2 shows differences between in-school and out- of -school adolescents' knowledge of HIV/AIDS and related socio-demographic factors by age, location, highest educational level attained, employment status, religious affiliation and maternal education. Statistical significant differences were observed as in-school adolescents were more likely to have a higher knowledge compared to out-of-school adolescents (p = 0.004) across all categories except the variable, "highest educational level attained". No statistical significant difference was observed at the junior secondary school level (p > 0.05) but at the senior secondary level, it was significant (p = 0.003) as out-of-school adolescents were more likely to have a higher score than in school adolescents (32.1 vs. 29.0). Association between misperception about HIV knowledge and attitude towards People Living With HIV/AIDS (PLWHAs) The study participants were not sympathetic towards PLWHAs. In the univariate analysis, about 3 of 5 respondents (58.4%) indicated they were willing to take care of a family member with AIDS. The majority of the respondents (53.8%) were of the view that people with HIV should not keep their status secret and others should be informed with 10.8% stating they had no opinion. Furthermore, only 23.0% expressed the view that PLWHAs should receive health care like everybody else, 20.3% indicated it should be more, and 56.7% stated that PLWHAs should receive less health care. Less than 1 out of 3 respondents (30.8%) indicated that PLWHAs could continue working with others on their jobs, 10.4% had no opinion and 58.8% were of the view that they should be dismissed from their jobs. Additionally, 62.7% would want PLWAs to be isolated but 29.8% were against isolation while 7.5% had no opinion. Table 3 shows respondents' answers to five questions that sought to tap attitude towards PLWHAs between those in school and those who were not. When chi-square analysis was used to examine the relationship between misperceptions involving transmissions through casual contact and each of the 5 questions assessing negative attitude toward PLWHAs, there were statistically significant associations between scoring high on misperceptions (hugging, shaking hands, toilet seats etc) and having negative attitude towards PLWHAs (0.001 < p < 0.009) on all questions. Compared to their counterparts in school, out -of -school adolescents were less likely to be willing to take care of relatives who have HIV/AIDS (27.8% vs. 39.9%, p = 0.004); less likely to allow PLWHA to conceal their status (64.4% vs. 42.2%, p < 0.001); less likely to allow PLWHAs to keep working with others (64.8% vs. 52.2%, p = 0.007); and more likely to let PLWHAs have less health care (61.3% vs. 51.7%, p = 0.026) and more likely to indicate that PLWHAs should be isolated from those who are not infected (72.7% vs. 51.7, p < 0.001). Some of those who indicated that PLWHAs should receive less health care, argued that PLWHAs would eventually die, so it did not make economic sense to waste scarce resources caring for them and that "They should be kept isolated so that they stop spreading the disease." AIDS was viewed as a major problem in Ghana by 82.0% of the respondents. Respondents specified that they had heard on the radio, TV, and in the print media that half of Ghana's population was dying from AIDS and that a minimum of 600,000 to 9.5 million of adults in a population of 20 million were living with HIV. The respondents viewed HIV/AIDS as a public health menace because of the following additional reasons: AIDS was killing students who were deemed future leaders of the country, many others in the commercial towns; trepidation and apprehension that those infected were knowingly and unknowingly spreading it to the unsuspecting public; concern that government was spending limited and scarce resources not only on educating people about AIDS, but also caring for PLWHAs who would eventually die despite the care they receive; and that scarce resources spent on PLWHAs could be used in development. In addition, PLWHAs were considered burdens on relatives, who care for them, and take care of their orphaned children when they eventually die. Adolescents were also concerned that the long incubation period for HIV made it possible for anyone infected to spread it to many partners he or she sleeps with, whether or not condoms were used. The result, they believed, is that AIDS puts the whole country at risk, not only the sexually active, but also those who have not engaged in sexual intercourse but intend to marry in the future. Women were mostly blamed for the propagation of AIDS in Ghana. The reasons cited for the propagation of AIDS could be categorized into three dimensions: economics; morality; and education even though these three issues were not mutually exclusive. Participants stated that because the rate of unemployment was very high, parents have shirked their responsibility in caring for their children who end up fending for themselves. Thus, in the absence of job opportunities in Ghana, women and girls prostitute themselves at home and abroad (Ivory Coast, Togo, Nigeria and in Europe, notably Holland, Germany and France). They contended that these commercial sex workers (CSWs) become infected and pass the infection to their unsuspecting sexual partners in Ghana. Those respondents who had moral concerns stated that there were too many fornicators, promiscuous, and sex-crazed boys and girls who indulge in indiscriminate sex, especially those between ages 16 to 19 in Ghana. Whether people get the infection through promiscuity or sex for money, the respondents contended that once infected, some of them do not want to die alone and deliberately engage in unprotected sex to infect unsuspecting partners, since they believed somebody had also infected them. Finally, participants believed that lack of basic education had made it difficult for the uneducated to get AIDS prevention messages, since most of the messages are written in English and hence the uneducated cannot take precautions and may be at risk of getting infected. Discussion According to UNAIDS, only 44% of men and 38% of women aged 15 to 24 correctly identify ways to prevent HIV3 and about 1 out of 5 had what can be classified as having high knowledge. This is consistent with this study in which the adolescents sampled in this population had a mean knowledge score of 26.64; sd: ± 6.74 and a median score of 28. Other researchers have also found low knowledge among adolescent populations studied elsewhere. For example, Aomreore, Alikor, and Nkanginieme found that 31%, 14.4%, 9.1% and 8% of the students they studied mentioned sexual intercourse, blood transfusion, vertical transmission and intravenous drug use respectively as modes of transmission12. Their study concluded that HIV/AIDS knowledge was poor among these adolescents12. Also, Mbago and Sichona, reported that 73% of the students had poor knowledge of HIV/AIDS and only 48% knew condom use and abstinence as methods of STI prevention11. There were also other gaps in knowledge and misconceptions about infection through casual contact. These knowledge gaps were consistent with other HIV studies carried on in other parts of the world30, 6, 31, 32. In these studies, people believed STIs could be contracted from saliva, toilet seats, donating blood and sharing kitchen utensils. Even though the above mentioned studies were conducted before HIV became a household name, nevertheless later studies, for example the 2007 UNAIDS report cited earlier, continue to show these gaps in knowledge. In this study, two out of every three participants believed that PLWAs should be quarantined and that the government should not spend money to provide health care for them, since they would die anyway. This proportion was far greater than the 29.8% observed in a study conducted among Kenyan secondary school students33. More than two decades into the epidemic in Ghana, it is surprising to have such gaps in knowledge even when there is anti retroviral drugs on limited basis. In addition, a statistically significant result confirmed an association between scoring high in believing that HIV could be contracted through casual contact and having a negative attitude towards PLWHAs. These misperceptions (e.g. contracting AIDS through casual contact) might explain the negative attitude in this population towards PLWHAs. The participants were also of the view that some PLWHAs, and especially commercial sex workers who contracted HIV, were either deliberately or inadvertently infecting the general population. Other researchers also found that respondents incorrectly indicated that one could contract AIDS through casual contact30-32, 34-37. The negative attitudes towards PLWHAs was not surprising, as one could reasonably assume that these misperceptions were in part responsible for the negative attitude towards PLWHAs, especially since respondents were of the view that PLWHAs should be quarantined. This finding is consistent with observations about adolescent respondents in a Nigerian study who stated that they would stop seeing friends and would reject relatives who develop AIDS38. Similar findings were observed in a Hong Kong study in which 42% stated they would not make physical contact with PLWHAs and 35% thought medical staff infected with HIV should be dismissed and 47% agreed there should be legislation barring PLWHA from visiting Hong Kong39. It is likely that today's Ghanaian adolescents may not come into contact with their peers who are dying from AIDS. This is due to the fact that children infected from their mothers hardly ever live to adolescence in the absence of anti-retroviral therapy and adolescents who are infected get into adulthood before AIDS manifests clinically. Hence there is the mistaken belief in the adolescent population that they are not vulnerable to HIV infection. Because AIDS in Ghana in the early days of the epidemic was associated with women who went to Abidjan, the capital of La Cote D'Ivoire, where they engaged in commercial sex, it might be that the sexually active adolescents discount their own risk, because they do not identify themselves with the stereotype they hold of people who contract HIV/AIDS. It is also important to note that even though there were misperceptions and negative attitude towards PLWHAs, the out-of-school adolescents were more likely to have negative attitudes compared to their in school counterparts. These have implications for HIV education and the need to reach this hard to reach group because the negative misperceptions have a bearing on stigma, discrimination and voluntary testing. These can impact on people who are infected to not test and hence unknowingly spreading HIV. Limitations The strengths in this study are manifested in the fact that this survey represents a cross-sectional study of in-school and out-of-school adolescents and was population-based. There is a high response rate (over 99%) with a sample size that is sufficiently large enough to represent junior secondary school and senior secondary school and out-of-school adolescents in the area studied. It may not necessarily, however, be representative of other adolescents in Ghana who may differ by geographic location, (large urban cities or large trading centers), ethnicity, and the economic status of their parents. Still, the adolescents surveyed are resident in a region of high HIV prevalence in Ghana and constitute a critical group to be studied. One drawback in using cross-sectional data such as in this study is that it measures HIV knowledge and attitude toward PLWHAs at only one point in time. This knowledge or attitude (positive or negative) may evolve with changes or exposure to AIDS-related information, and new situations. Thus the variables, which are statistically significant may change if measured at another point in time. Conclusion The results of the study shed light on HIV knowledge among in school and out of school adolescents and their prevailing misperceptions regarding HIV/AIDS and other STIs, and their attitude towards PLWHAs. The information gathered from this study can be used to improve efforts to increase tolerance towards PLWHAs and destroy the myths around contracting HIV through casual contact. With the introduction of HIV drugs in Ghana (limited though the coverage is) and with increased campaign for voluntary testing, the success of these initiatives will hinge on people testing voluntarily. Thus it imperative that the educational messages become correct so that individual and societal obstacles that impede AIDS prevention efforts (stigma and discrimination) become limited. An HIV infected person or an individual who has engaged in high risk behavior may not be willing to know his status especially when there is the tendency of stigma and discrimination. With appropriate education and correct information, the misperceptions may eventually be removed at the individual and societal level. Acknowledgements This study was completed with funding provided by Rockefeller Foundation under the auspices of its African Dissertation Internship Awards and the University of British Columbia Department of Healthcare & Epidemiology. My sincere appreciation to Professors Martin Schechter, Robert Hogg, Samuel Sheps and Mark Tyndall (all of University of British Columbia, Vancouver, Canada), Kofi Awusabo-Asare (University of Cape Coast, Ghana) for their invaluable guidance and Matthew Adeyanju (Ohio University, Athens) for his helpful comments. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09016t1.jpg] [hs09016t2.jpg] [hs09016t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}