 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
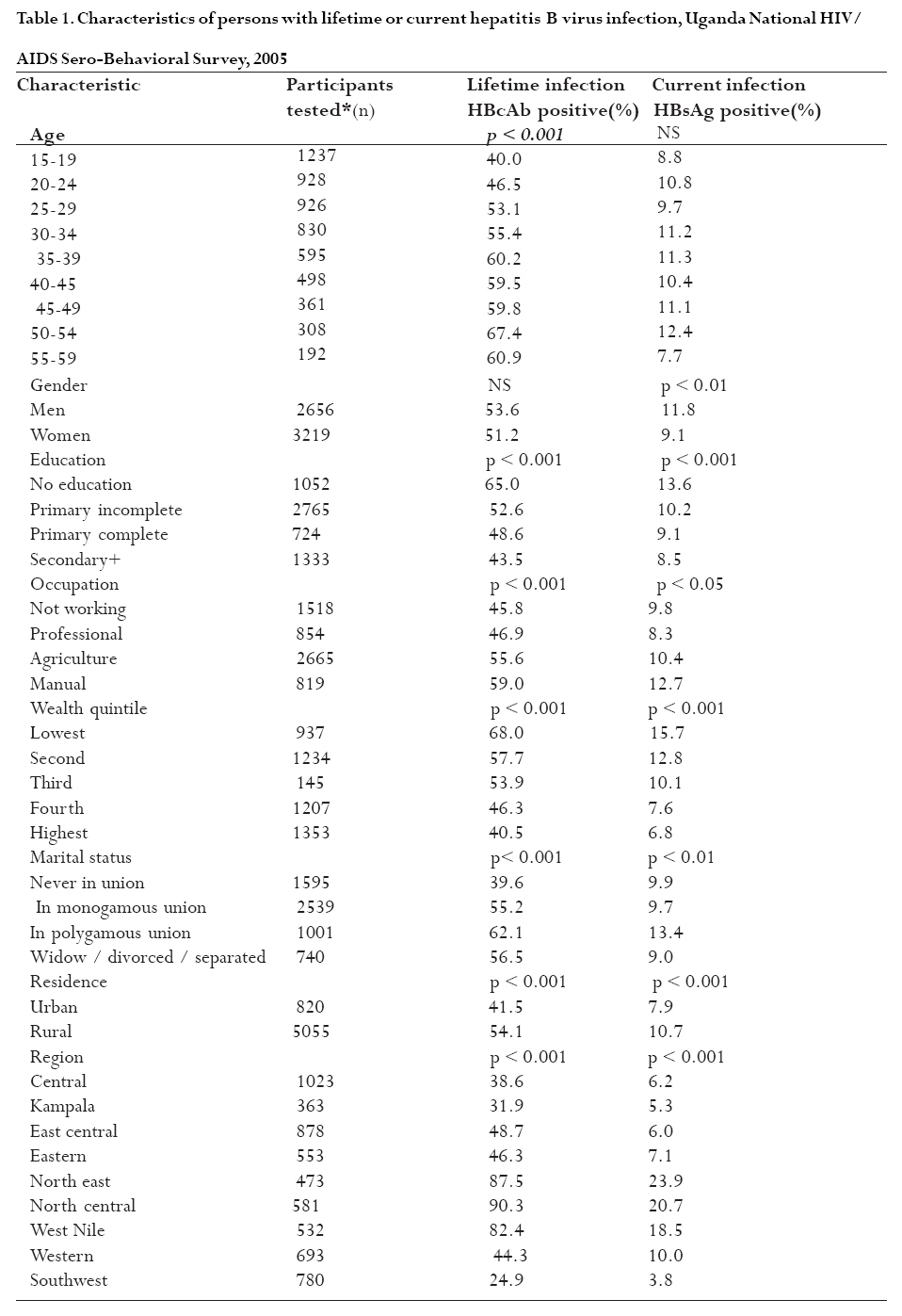
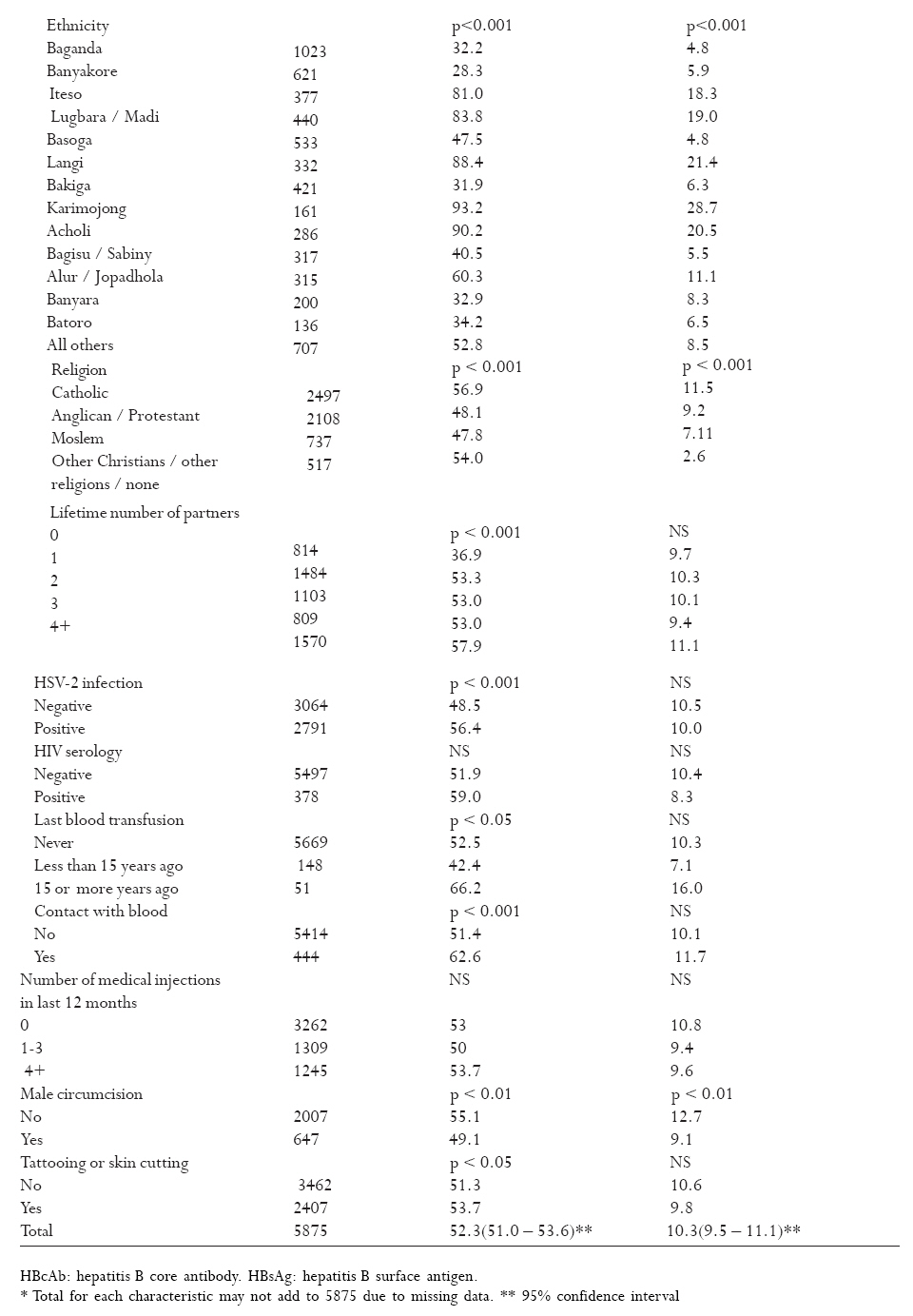
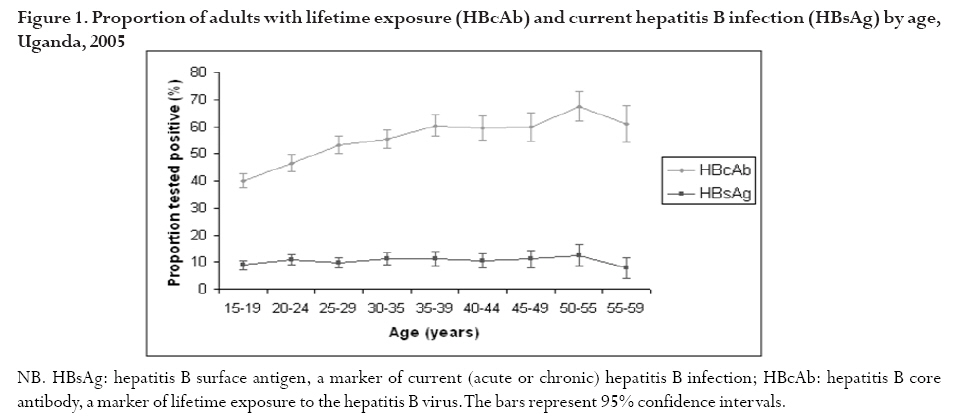
African Health Sciences, Vol. 9, No. 2, June, 2009, pp. 98-108 Hepatitis B infection is highly endemic in Uganda: findings from a national serosurvey Josephine Bwogi1, Fiona Braka2, Issa Makumbi3, Vinod Mishra4, Barnabas Bakamutumaho1, Miriam Nanyunja2, Alex Opio5, Robert Downing6, Benon Biryahwaho7, Rosamund F. Lewis2 1 EPI Laboratory, Uganda Virus Research Institute, P.O. Box 49, Entebbe, Uganda Code Number: hs09018 Abstract Background: Infant immunization against hepatitis B began in Uganda in 2002.
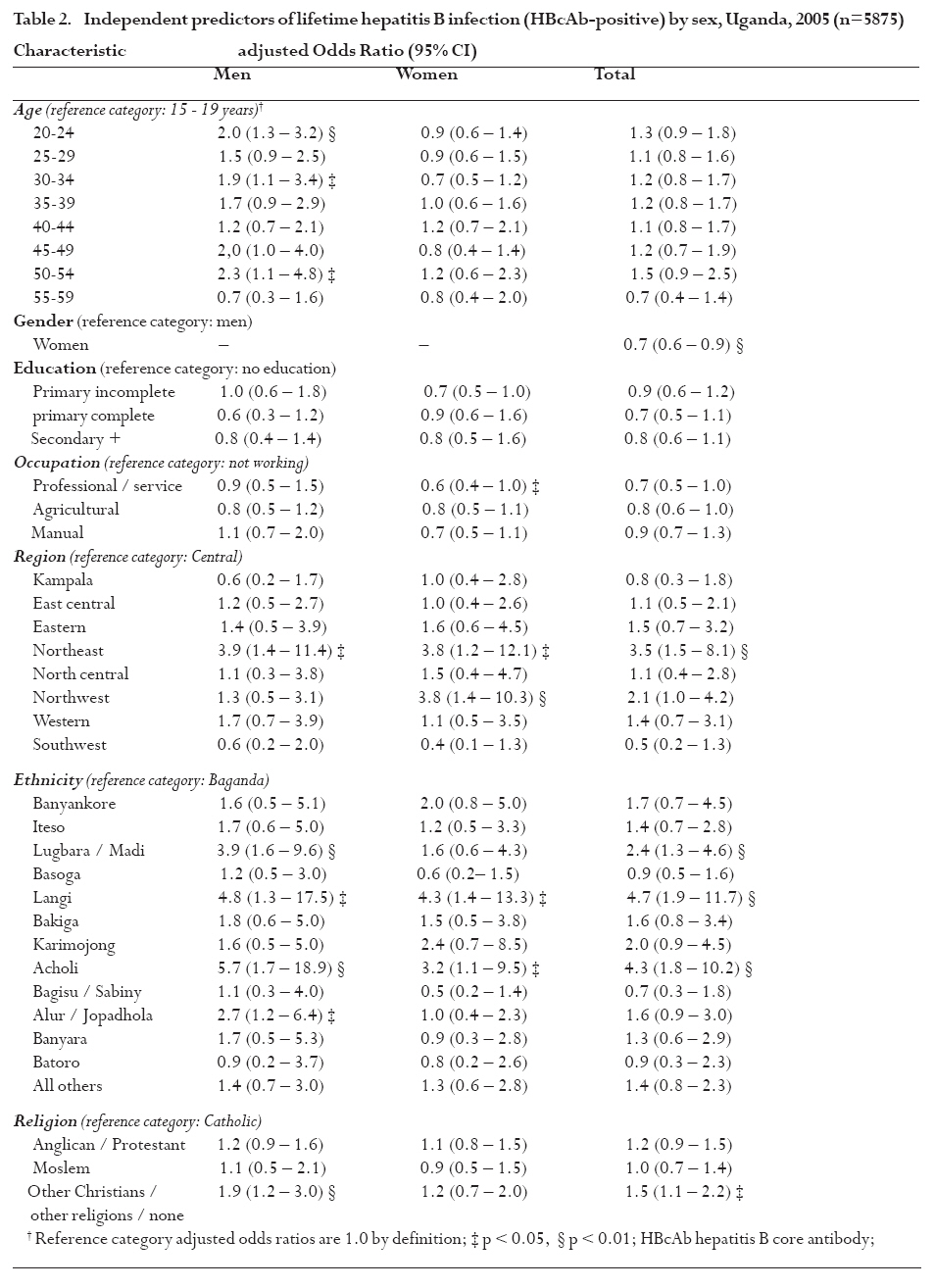
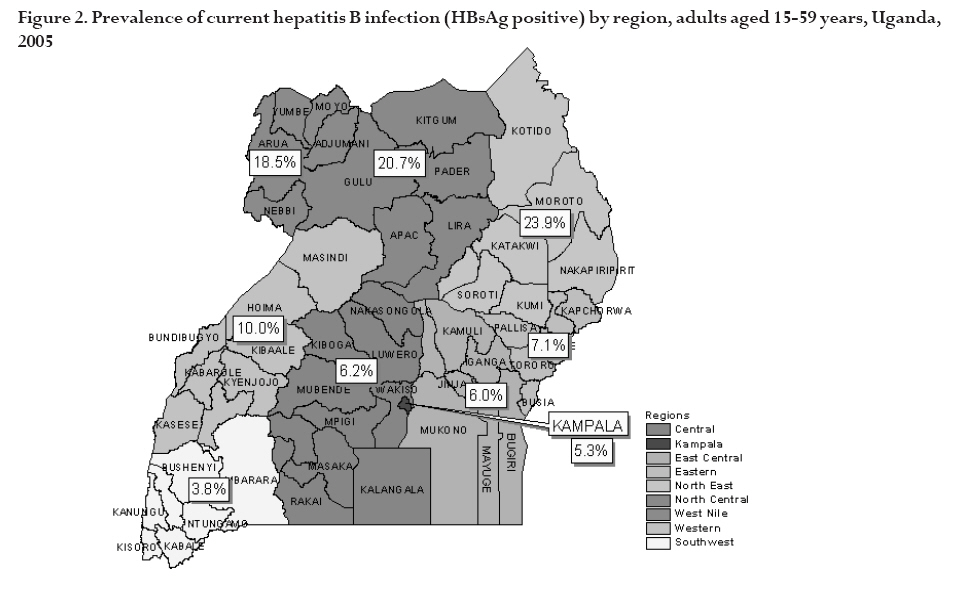
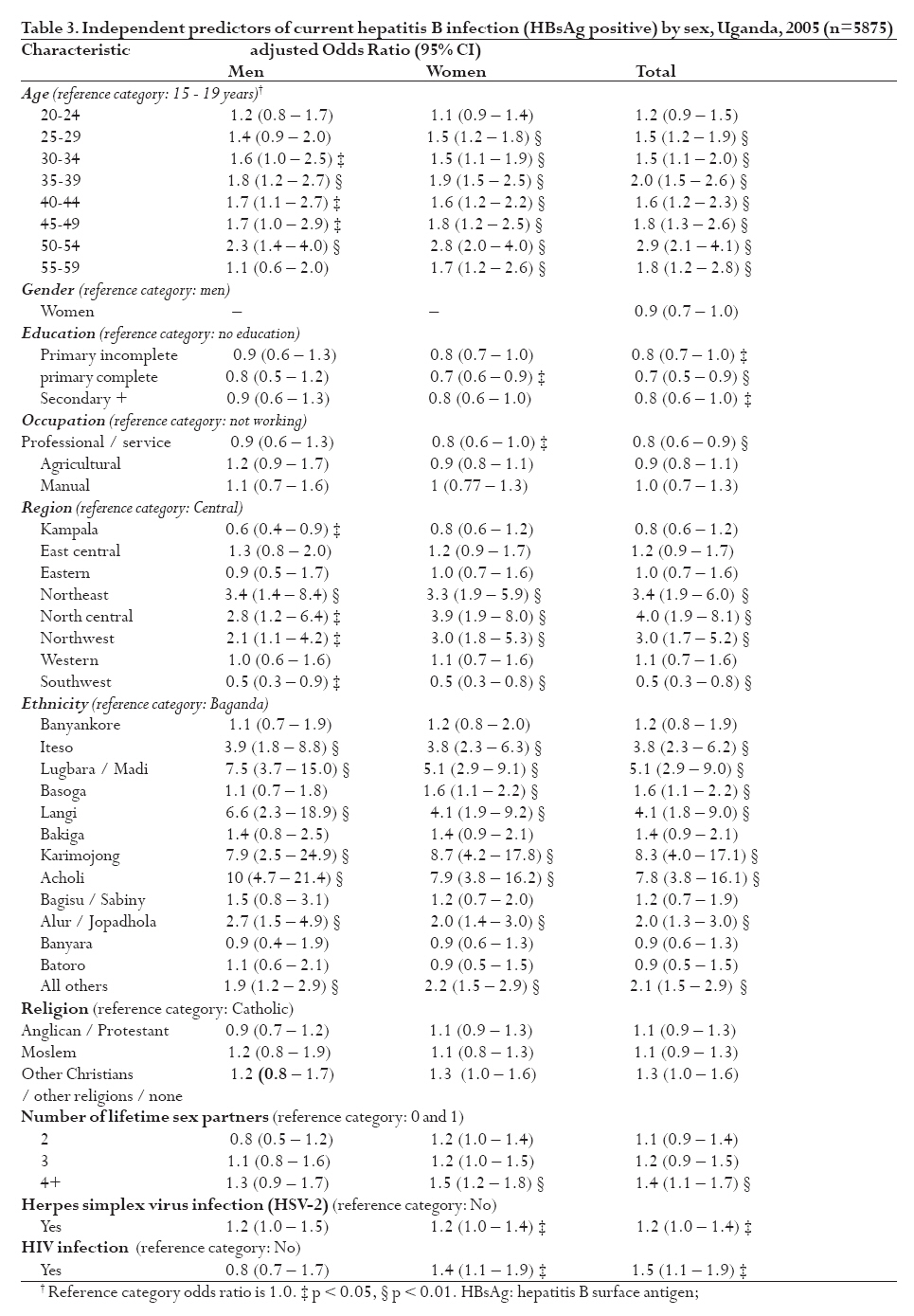
Key words: hepatitis B, HBsAg, HBcAb, Uganda, vaccine, immunization, HIV, coinfection, circumcision, survey Short running title: Hepatitis B is highly endemic in Uganda Introduction More than 2 billion people worldwide are estimated to have had hepatitis B virus (HBV) infection and 350 million chronic carriers of the virus are at high risk of cirrhosis of the liver and primary liver cancer.1-3 HBV accounts for an estimated 500,000-700,000 annual deaths worldwide.1,4 With a safe and effective vaccine available since 1982, much of this infection and death should be preventable.3-5 The public health burden of HBV infection in Uganda is unknown, although the country has long been considered to be among the highly endemic countries of sub-Saharan Africa,4,6 with more than 8% of the population expected to harbour chronic infection. Results from a few Ugandan studies have supported this hypothesis: the prevalence of HBV surface antigen (HBsAg), a marker of chronic HBV infection, ranged from 6 to 15% among blood donors when HBV screening was introduced,7 and in selected populations in Uganda.8,9 In medical students and health workers, the prevalence of HBsAg ranged from 8 to 11%.10-12 These studies found a prevalence of HBV core antibodies (HBcAb) between 60 and 66%, which, in the absence of HBV vaccination programs, suggests that two-thirds of the Ugandan population is infected with HBV during their lifetime.10,12,13 In regions of high endemicity, HBV is mainly contracted at birth or during early childhood.3 The development of chronic infection occurs in approximately 90% of persons infected perinatally, in 30% infected in early childhood and in 6% infected after 5 years of age.4 Persons with chronic HBV infection have a 15-25% risk of dying prematurely in adulthood from HBV related cirrhosis and hepatocellular carcinoma, and acutely infected individuals occasionally succumb to fulminant liver failure.4 Adults acquire HBV through contact with infected blood or body fluids, through unsafe injections, sexually or by other means of horizontal or iatrogenic transmission.3,14-18 In accordance with the WHO-recommended strategy for HBV control,1,4,19 HBV vaccine was introduced in Uganda in 2002 as part of the Expanded Programme on Immunisation (EPI) and is given at 6, 10 and 14 weeks of age.20 To establish the prevalence and distribution of disease, explore risk factors for HBV infection, and provide baseline data for future assessment of the impact of hepatitis B vaccination in Uganda, a national HBV sero-survey was conducted among adults aged 15-59 years and children under five years of age. The findings in adults are presented here. Methods Study design and subjects A hepatitis B sero-survey was incorporated into the 2005 Uganda HIV/AIDS Sero-Behavioural Survey (UHSBS),21 a nationally-representative, population-based cross-sectional survey involving adults 15 to 59 years old and children <5 years old. During the survey, data were collected on demographic, social, and behavioural indicators and blood samples were obtained for testing of HBV, HIV, and herpes simplex virus type 2 (HSV-2) seromarkers. Separate informed consent was provided by respondents for interviews and blood sampling. The survey utilized a two-stage sample design. The first stage involved selecting sample points or clusters from a list of enumeration areas covered in the 2002 Household and Population Census. A total of 417 clusters (74 urban and 343 rural) were selected. The second stage of selection involved systematic sampling of households from the census list of households in each cluster. Twenty-five households were selected from each cluster. The sample was constructed to allow separate estimates for key indicators for nine regions, consisting of Kampala (the capital city) and eight regions created by grouping the (then) 56 districts in Uganda. To allow a sufficient number of cases in each region, the sample was allocated more or less equally across all nine regions. As the sample was not allocated in proportion to the population of each region, the UHSBS sample is not self-weighting at the national level. Consequently, weighting factors were applied to the data to produce nationally-representative results. A total of 10,437 households were selected from the 417 clusters, of which 9,842 were occupied at the time of the survey. Of the occupied households, 9,529 were interviewed, resulting in a household response rate of 97%. In the interviewed households, a total of 11,454 women and 9,905 men aged 15 to 59 years were eligible for individual interviews and blood sample collection. Individual questionnaires were completed for 95% of eligible women and 89% of men; blood specimens were collected for 90% of women and 84% of men. A nationally-representative systematic sub-sample of 1-in-3 participating adults was selected for HBV seromarker testing, maintaining the stratification by region and residence (urban and rural), resulting in a total of 6037 adults surveyed, sufficient to detect a prevalence of HBsAg of 8%, assuming a design effect of 1.5 with 1% precision and a confidence level of 95%. The survey protocol was approved by the Uganda National Council of Science and Technology, the Centers for Disease Control and Prevention (CDC), and by the Institutional Review Boards of the Uganda Virus Research Institute (UVRI) and ORC Macro. Measurements Household and individual questionnaires, administered to adult respondents, were translated into six local languages and pre-tested by trained personnel. Demographic variables assessed included age in five-year groups, gender, marital status, ethnicity, religion, residence (urban, rural) and region of residence (Kampala and eight regional district groupings). Socioeconomic variables assessed included education, occupation (professional or service work, agricultural work, manual labour, not working) and wealth index in quintiles constructed according to ownership of consumer goods. Possible exposure to blood, body fluids or contaminated instruments was assessed through variables for history of blood transfusion (never, in last 15 years, 15 or more years ago), contact with the blood of others, tattooing or skin cutting and medical injections received in the last 12 months. Sexual behavior risk was assessed through number of lifetime sex partners, age at first sex and condom use at last sex in the last 12 months. Men were asked if they were circumcised. Variables were categorized as listed in Table 1a and b. Laboratory methods Venous blood (4.5 ml) was collected from the consenting participants in an EDTA Vacutainer tube. Plasma was transferred to micro-vials, transported to UVRI in liquid nitrogen and stored at -20oC. After thawing, aliquots of 50 µl of plasma were tested in the Expanded Programme on Immunization (EPI) laboratory at UVRI for HBcAb antibodies using a commercial enzyme-linked immunoassay (EIA) (Abbott Murex, Dartford, UK), which has a sensitivity and specificity of 100% (with lower 95% confidence limits of 99.18% for sensitivity and 98.98% for specificity). HBcAb-positive specimens were further tested for HBsAg by EIA (Abbot Murex, Dartford, UK), which has a sensitivity of 100% (95% lower confidence limit 99.92%) and specificity of 99.97% (95% lower confidence limit 99.99%). Evidence of lifetime (past or current) HBV infection was defined by a positive test for HBcAb, indicating previous exposure to the hepatitis B virus. Evidence of current HBV infection was defined by a positive test for HBsAg, which could be due to a chronic carrier state or acute infection. Any specimen negative for HBcAb was assumed, for the purpose of this analysis, to be negative for HBsAg. For quality control, 5% of HBcAb-positive and 5% of HBcAb-negative specimens were randomly selected and retested by the CDC-Uganda laboratory using the same kits. Likewise, 5% of HBsAg positive and 5% of HBsAg negative specimens (randomly selected) were retested in the CDC lab. A discordance of less than 10% between the quality control lab and the original test results from the EPI laboratory was deemed acceptable. Testing for other biomarkers, including HIV and HSV-2, was conducted using standard testing and quality-control procedures.22 The laboratory test results for individuals were anonymously linked to individual and household questionnaire information through their unique identifiers. Details of these procedures are provided elsewhere.22 Data analysis To establish the prevalence of current and lifetime hepatitis B infection in the sample population, we determined the proportion of tested specimens positive for HBsAg and HBcAb, respectively. To estimate the number of adult Ugandans with current hepatitis B infection in 2005, the year of the survey, we extrapolated the proportion with a positive HBsAg test to the general adult population aged 15 years and older. We used the estimated Ugandan population for 2005 of 26.8 million persons, as projected from the national census of 2002, multiplied by the population distribution of 50.7% for this age group23 and by the proportion positive for HBsAg. The proportion of respondents with lifetime or current HBV infection was then determined for each demographic category and other predictors in a bivariate analysis. Differences between categories were assessed by Pearson chi-square tests. All variables of theoretical importance (based on the known epidemiology of HBV infection and hypothesized modes of transmission), or of statistical significance in the bivariate analysis, were considered for inclusion in a multivariate logistic regression model. Variables retained in the final model included age, education, occupation, ethnicity, religion, wealth, residence (urban/rural), region of residence, number of lifetime sex partners, contact with blood, blood transfusion, tattooing, number of medical injections, male circumcision, and sero-status for HSV-2 and HIV. All analyses accounted for the survey sampling design and were carried out using STATA version 8. ResultsParticipant characteristics and hepatitis B prevalence Of the 18,525 participants aged 15-59 years recruited in the UHSBS from whom blood was collected, 6037 were systematically selected for HBV tests. Of those selected, 5875 (97.3%) had an adequate blood specimen and were tested for HBcAb antibodies, and thus had full results in the database. Quality control for HBV tests showed 3% discordance for HBcAb-positive, no discordance for HBcAb-negative results, 9% discordance for HBsAg-positive and 6% for HBsAg-negative specimens between the EPI and CDC labs respectively. Further analysis proceeded with the original test results. Comparison of the HBV sub-sample with the main survey sample showed that the two were similar for all main demographic and socioeconomic characteristics. Of those tested, 3072 (52.3%, 95% CI: 51.0 - 53.6) were HBcAb positive; 1424 (53.6%) of the tested men and 1648 (51.2%) of the tested women. Six hundred and six (10.3%, 95% CI: 9.5 - 11.1) were HBsAg-positive, 313 (11.8%) men and 293 (9.1%) women (Table 1a and b). By the age of 15-19 years, 40.0% (95% CI: 37.2 - 42.7) of the population had been infected with HBV (Figure 1). The proportion with lifetime HBV infection increased with age, but declined slightly after the age of 50-54 years (Figure 1). The proportion of adults with current HBV infection remains more or less constant across all adult age groups (Figure 1). The projected Ugandan population aged 15 years or older in 2005 was 13.6 million persons. Therefore, approximately 1.4 million (95% CI: 1.3 - 1.5 million) adults were actively infected with hepatitis B virus at the time of the survey. Risk factors for lifetime HBV infection In unadjusted analysis, the prevalence of lifetime HBV was significantly associated with age, education, occupation, wealth, marital status, religion, ethnicity, residence (urban/rural), region of residence, number of lifetime sex partners, HSV-2 infection, lack of male circumcision, history of blood transfusion, contact with blood, and tattooing or skin cutting (Table 1a and b). Lifetime HBV exposure (HBcAb positive) was much higher in the north central, northeastern and northwestern regions than in other regions, and higher in rural than urban areas. The prevalence of lifetime HBV exposure increased with number of lifetime sex partners, but decreased with higher education and wealth. History of blood transfusion more than 15 years previously, contact with blood and tattooing or skin cutting, and evidence of Herpes simplex virus type 2 (HSV-2) infection were each associated with a higher prevalence of lifetime HBV exposure. Circumcised men were less likely to have had HBV than uncircumcised men (Table 1a and b). After controlling for confounding, the factors found to be independent predictors of lifetime HBV infection were male gender, being of Acholi or Langi ethnicity, and Lugbara/Madi or Alur/Jopadhola ethnicity in men, religion (other than Catholic, Anglican or Moslem) for men, residence in the northeastern region for men and women and in the northwestern region for women. Being in a professional or service occupation was associated with lower risk of lifetime HBV infection in women compared to other occupational categories (Table 2). Risk factors for current HBV infection In bi-variate analysis, the prevalence of current HBV infection (HBsAg positive) was associated with gender, education, occupation, wealth, marital status, religion, ethnicity, urban/rural residence, region of residence and male circumcision (Table 1a and b). Prevalence of current HBV infection was higher in men than women and much higher in the northeast, north central region and northwest (18.5 - 23.9%) than in other regions, with the lowest in the southwest (3.8%) (Figure 2). The Karimojong, Langi and Acholi ethnic groups had the highest prevalence of current HBV infection, as high as 28.7% compared to 4.8% in the Baganda, and those with little or no education had a higher prevalence than the more educated. The likelihood of being infected also declines with increasing wealth, with 15.7% infected in the lowest wealth quintile compared to 6.8% in the highest quintile. Those with manual and agricultural occupations had a higher prevalence of current HBV infection than the professional or service occupations, or those who were not working (Table 1a and b). Independent predictors of current HBV infection were age greater than 24 years, lower educational status, ethnic group (Iteso, Lugbara/Madi, Langi, Alur/Japadhola, Karimojong and Acholi, and also Basoga for women), region of residence (higher in the northeastern, north central, and northwestern regions and lower in the southwestern region and Kampala region for men), number of life-time sex partners, and for women, having HSV 2 or HIV infection. Women in a professional or service occupation were at lower risk (Table 3). Discussion In this first reported national hepatitis B serosurvey, we confirm that HBV infection is highly endemic in Uganda. With one in ten adults carrying hepatitis B surface antigen, we estimate that 1.4 million adult Ugandans were living with active disease in 2005, and probably a similar number of children, compared to the 900,000 Ugandans living with HIV/AIDS.21 The prevalence of HBV infection observed in this study is generally within the expected range for highly endemic countries in sub-Saharan Africa4,24 and consistent with smaller studies among medical students, inpatients, and health workers in Uganda.10,12,13 Nonetheless, the prevalence of 28.7% active infection in the Karamojong is among the highest reported in any population. 4 Regional variations in current and past HBV infection were observed, the northern regions having almost double the national prevalence with a six-fold difference between northeast and southwest, similar to earlier observations among blood donors.7 The ethnic groups that traditionally reside in the northern and eastern regions of the country were more affected, particularly the Karamojong, Acholi and Langi tribes, as found previously,8,13 although ethnicity and residence appeared nonetheless to be independent risk factors. Early sexual debut is more predominant in the eastern and east central regions21 and cultural practices such as traditional tattooing or skin cutting have been observed particularly among women in the eastern, east central, northeastern and northwestern regions. However, in the presence of other prominant risk factors, we were unable to demonstrate the independent contribution of traditional practices to the high prevalence of HBV infection in those areas. We also found that HBV infection occurs more frequently in rural areas and risk rises with poverty and lack of education, as do other forms of ill health.25,26 Socio-economic conditions among the poor and less educated, especially in the rural areas, may contribute to HBV exposure. By the age of 15-19 years, 40% of youth in Uganda have already been exposed to the hepatitis B virus, confirming that HBV infection occurs primarily in childhood. Poverty-related factors such as overcrowding (typical in camps for internally displaced persons in northern Uganda and in kraals of northeastern Uganda) and close contact among children could contribute to higher risk among the rural poor. 27 This study finds that Ugandan adults continue to be exposed to HBV. In the multivariate analysis with potential confounders controlled, the number of lifetime sex partners and presence of HSV-2 or HIV infection appear as risk factors for chronic HBV infection, probably due to common modes of transmission.8,13,28 Thus, the stable prevalence of chronic infection in adulthood suggests that new infections are acquired at a rate equivalent to the loss of HBsAg of 1% per year among carriers,4 plus mortality from the disease and associated complications. Chronic infection is also slightly more common in men than in women, a pattern observed in other sub-Saharan African countries.24,28 In view of recent studies confirming that male circumcision offers some protection against HIV,30-32 our finding of fewer HBV infections among circumcised men suggests this practice may also protect against HBV. Aggressive HIV prevention strategies over the past 20 years have promoted sexual behaviour change. Nonetheless, 14% of youth reported having had sex by the age of 15 years and the national survey revealed a secular trend of fewer adults engaging in safer sex in the 12 months preceding the survey.21 Sexual transmission of HBV may again become more common after the age of 15.33 Rising exposure to blood transfusions with age could also contribute to HBV infection21 although pre-collection screening of potential donors appears to have improved, with a decline in HBsAg from 6.8% in 1998 to 4.0% in 2005.34,35 Hepatitis B testing is not presently part of routine care for HIV infected patients in Uganda. However, HIV infection may cause reactivation of `silent' chronic HBV or renewed susceptibility to HBV infection due to immuno-suppression,36 and HIV-infected individuals subsequently infected with HBV are more likely to become chronic carriers.28 Reactivation of HBV infection may also occur when HIV patients begin anti-retroviral therapy,28,37,38 and there is frequent co-infection of HIV and tuberculosis with potential for hepatotoxicity of tuberculosis treatment. These findings have implications for prevention and care of both hepatitis B and HIV/AIDS in sub-Saharan Africa.39 Therefore, the value and role of routine hepatitis B testing for HIV-infected patients should be further explored. HBV testing could be considered for patients about to begin anti-retroviral therapy. The validity of our findings is supported by the high response rates and large sample size of this nationally representative survey, and high sensitivity and specificity of EIA test kits used in the study. However, prevalence of infection has most likely been underestimated for several reasons. The study design does not account for earlier HBV-related deaths among chronic carriers, spontaneous resolution of previous infections, latent infections seronegative for HBsAg, or acute infections present in the window period before the appearance of hepatitis B core antibodies. Occult HBV infection was also not identified since PCR tests were not carried out. The study was not designed to explore the clinical features of hepatitis, such as fatigue, jaundice, hepatic failure or other complications. The discordance of hepatitis B tests between the EPI laboratory and the CDC Reference laboratory suggests that some misclassification of infection status may have occurred. Any association between HBV infection and tattooing or injections may be underestimated due to the short recall period. Finally, the cross-sectional design precluded ascertaining the chronology of putative risk factors and infection in adults. These findings describe the national epidemiology of hepatitis B infection in Uganda for the first time and highlight the extremely high burden of disease in the country, underscoring the critical need for preventive measures. Immunization remains the most effective method of prevention and control of HBV infection available.4,5 The infant hepatitis B immunization programme should be strongly supported and sustained. The Ministry of Health should also consider vaccination for school-aged children and high-risk groups such as health workers, and use of universal precautions by health workers should be reinforced.10-12,40 The pattern of perinatal and childhood hepatitis B transmission and potential benefit of a birth dose of hepatitis B vaccine should be determined.4 Public information programs can raise awareness of this devastating illness and available prevention strategies, including immunization for children and adults, as well as prevention of sexual transmission. Finally, it would be useful to explore further the relationship between HIV, HBV and circumcision, as well as the role of HBV testing and vaccination for persons with HIV. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09018f1.jpg] [hs09018f2.jpg] [hs09018t1b.jpg] [hs09018t3.jpg] [hs09018t2.jpg] [hs09018t1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}