 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
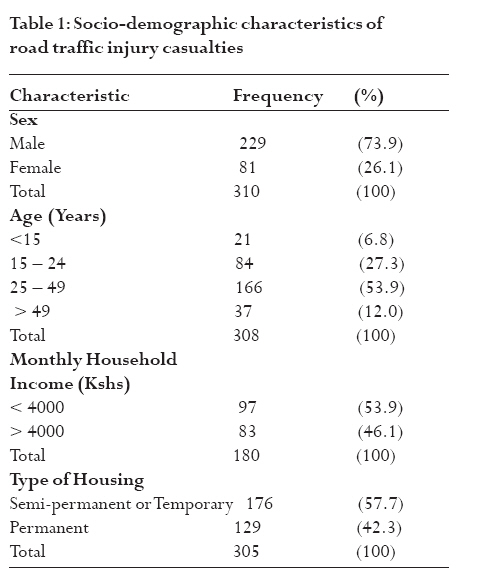
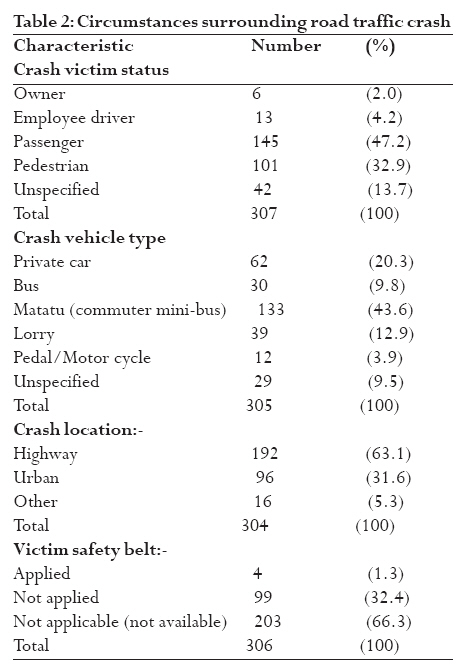
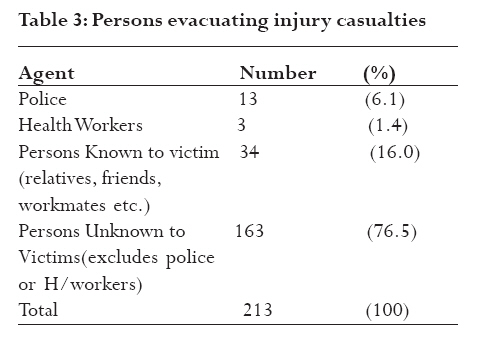
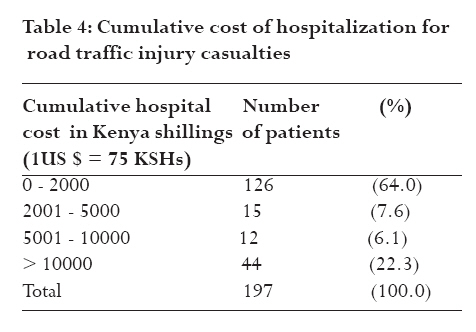
African Health Sciences, Vol. 9, No. 2, June, 2009, pp. 118-124 Severe road traffic injuries in Kenya, quality of care and access Macharia WM1, Njeru EK1, Muli-Musiime F2 and Nantulya V 2 . 1 Nairobi Clinical Epidemiology Unit, University of Nairobi, 2 AMREF, Nairobi. Code Number: hs09020 Abstract Background: Road traffic injuries (RTI) are on increase in developing countries. Health care facilities are
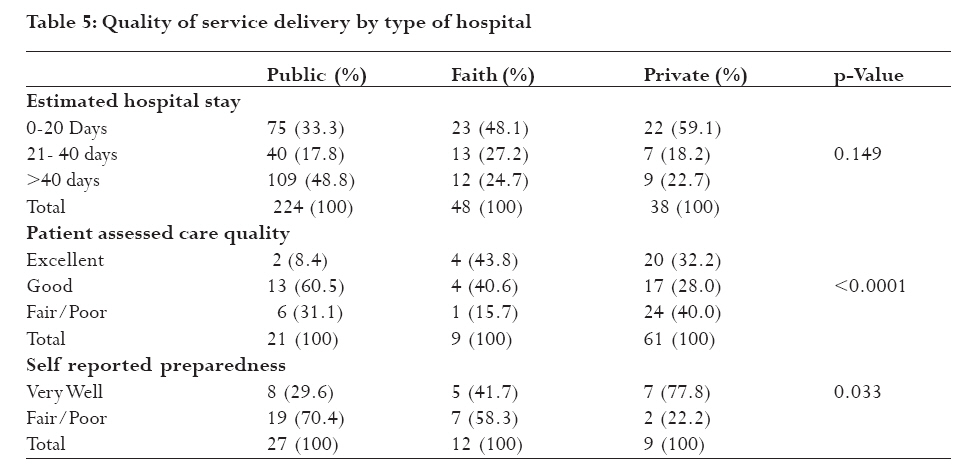
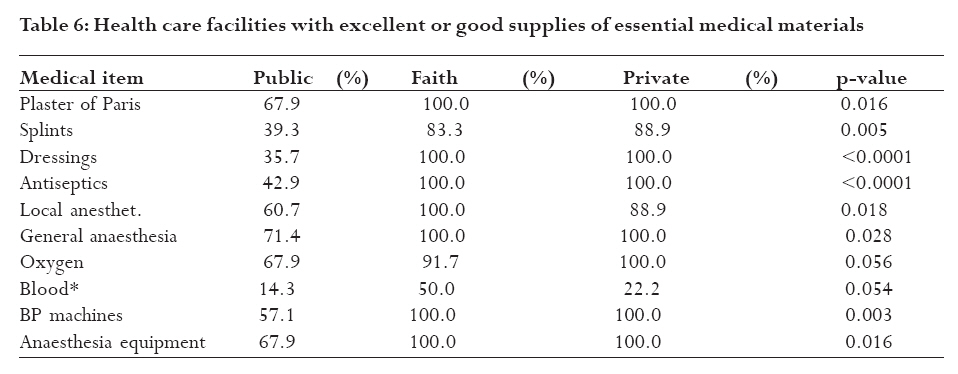
poorly equipped to provide the needed services. Introduction Road traffic Injury (RTI) is a rapidly growing, yet preventable, public health problem worldwide (1-4) that is projected to become the third leading cause of morbidity and mortality by the year 20205. Road crashes have enormous impact on national economies and represent a major human tragedy. In 1985 alone, motor vehicle crashes cost United States more than 75 billion US dollars6. It has been estimated that there are over 1.18 million road traffic injury related deaths annually world wide, with 74% occurring in developing countries 1, 7. The young and socio-economically disadvantaged tend to experience disproportionately higher RTI fatality rates8, 9. In East Africa, road traffic crashes are among the top causes of death from injuries. Fatality from RTI in Kenya is estimated to have increased by 578% between 1962 and 1992, rising from 7.3 to 8.6 per 100,000 population. Most of the road traffic crashes occurred on major rural roads and were associated with higher case fatality rate than those occurring in urban areas10, 11. Reports of fatal crashes on roads in Kenya have continued to feature prominently in the local dailies and electronic media in the form of news flashes and editorials. Despite the public health importance of RTI, there is little, if any, published information on how RTI casualties are handled at the crash scenes, evacuated to health facilities or received and managed at the facilities. This survey was motivated by the need to map out the magnitude of road traffic injuries in Kenya in order to provide baseline data to policy makers and other stake-holders who may wish to undertake interventions to improve road safety in the country. The aim of this study was therefore, to determine access and quality of health care for road traffic injury (RTI) casualties in Kenya. We also undertook to find out the extent to which health care facilities in Kenya were prepared to manage RTI emergencies. Since the time when this study was conducted, there have not been any targeted efforts to address this concern in the country. While availability of medical supplies may have some how improved as an indirect result of rising economic growth realized over the last few years, access to care and quality of services are unlikely to have changed much. Methods A national road traffic injuries survey was carried out between August 1997 and August 1998 as a collaborative effort between an institution of higher learning (University of Nairobi) and a service oriented non-governmental organization (African Medical and Research Foundation, AMREF). The study was part of a larger enquiry into the social determinants of health inequities associated with road traffic injuries undertaken under the auspices of the Global Health Equity Initiative of the Rockefeller Foundation (11). Severe road traffic injury was defined as that which resulted in hospital admission in contrast to lethal and minor injuries resulting in death and outpatient care respectively. Outcome of severe injuries included death, disability and complete recovery. A sample size of 50 hospitals was considered adequate apriori for this survey in view of available resources. To include as many road traffic injury casualties as possible, all the major private and faith-based hospitals in the country were deliberately included in the survey. Kenyatta National Referral and Teaching Hospital and all provincial hospitals were also included as they have a large burden of severe road injuries that they cater for. Facilities in the North-eastern Province were not eligible in consideration of the low vehicular traffic and poor road infrastructure. A list of all district and sub-district government hospitals in the country, excluding North-eastern Province, was obtained from the Ministry of Health. After categorizing the hospitals by province and in alphabetical order, four hospitals were chosen per province using systematic sampling technique. Authority to carry out the national survey was obtained from the Director of Medical services who issued an introductory letter to the hospital chief executives to provide necessary cooperation. Despite prior visits having been made by the principal investigators to introduce the study, interviewers were required to carry with them copies of the letter to every hospital they visited. Casualty department patient attendance registers were examined to identify road traffic injury patients and admitting wards. All road traffic injury casualties in the wards during the visit were eligible for inclusion. Records of those treated and discharged were not included in the study. Interviews were conducted with the patient or a close relative conversant with crash circumstances if the former was indisposed. A structured questionnaire was used to obtain information on sex, age, educational and socio-economic status, type of care provided at the site, how evacuated from the crash site, waiting time at health care facility, hospital costs and ability to pay, among other details. Type of housing, employment, level of formal education, and household income were used as surrogates for socio-economic status. Information on availability of medical supplies at the facility, state of institutional preparedness for injury emergency care, anticipated duration of hospital stay and expected treatment outcome were provided by hospital administrators and most senior primary clinicians (nurses, clinical officers or doctors) attending to the patients. Validation of responses on availability of essential medical supplies for trauma care was done through inspection and recording by the research assistants of what was available at the time of the visit. Information of current hospitalization cost on day of the survey was obtained from the accounts departments of the respective hospitals. This was an underestimate as the patients were still in hospital. Data analysis: Data was displayed in tables and analyzed using univariate and bivariate techniques. P-values were computed for categorical variables using Chi square test and Fisher's Exact test depending on the size of the data set. Independent student t-test was used for continuous variables. A p-value of less or equal to 0.05 was considered to constitute a statistically significant difference. Sub-analysis by ownership of health facility (Public, private and faith-based) was conducted for various outcome variables. Ethical clearance for the national survey was obtained from the Office of the President, as required by the Kenyan law. Individual patients or relatives also gave free and informed consent before participating in the interview. Authority to visit health facilities for the study was obtained from the Director of Medical Services and respective institution administrators. Results Of 53 hospitals identified for inclusion in the study, five rural public hospitals were not accessible for data collection due to logistic reasons. Analyzable data were obtained from nine private, 12 mission and 27 public hospitals. Three hundred and ten road traffic injury casualties admitted in the hospitals, or their next of kin, participated in a face-face interview. Majority of the injured were treated at public health facilities (72.3%), with 15.6% and 12.2% of the casualties receiving care at faith-based and private hospitals, respectively. Permission to carry out the survey was granted by all the hospitals and no patient or relative declined to be interviewed though there were situations when some required information was not obtained for various reasons. Respondents were the injury casualties in all but a few cases which were not sub-analyzed. Table 1 and 2 show baseline characteristics of those interviewed, and the alleged circumstances surrounding the crash as judged by the interviewees. Most of the casualties were passengers (47.2%) or pedestrians (32.9%). Majority of passengers (70.2%) were traveling in buses, and mini- and midi- buses known locally as "matatus" (15.7%). Of those interviewed, 79.7% were admitted in hospitals based in rural areas. Highways, outside urban areas were the scene of crashes involving 63.1% of those interviewed. In terms of days of the week, Fridays and Saturdays accounted for 30.5% of all the casualties. Baseline characteristics of injury casualties Severely injured casualties were nearly three times more likely to be male than female (males 73.9% Vs females 26.1%). The peak age of casualties was 15-49 years (81.2%) with only 12.0% being above the age of 49 years at time of crash. Use of safety belts at the time of motor vehicle crash was reported by only 4/306 (1.3%), while 66.3% were in vehicles without safety belts; mainly public service vehicles (Table 2). About half (51.9%) of those admitted with injuries reported their vehicle to have been over speeding at the time of crashing. The driver was suspected to have been under the influence of alcohol by 10.3% of the respondents. Almost two thirds (60.0%) of the casualties had primary level or no education at all which was consistent with predominance of a low socio-economic status. About 87.6% of 266 casualties admitted in hospitals did not have any form of health or accident insurance cover. Further, half (53.9%) of the households from which casualties hailed, had monthly incomes of less than 50 US dollars with only 21% reporting income above 130 US dollars. Only 16.0% of people injured reported having received any form of first aid at the crash site. Table 3 shows the persons responsible for transportation of the injured to hospitals. Out of those who received first aid at the crash site, 74.0% received from members of the public, other motorists or the less injured casualties. Ambulance personnel and police officers played a relatively bigger role for casualties evacuated to Kenyatta National Hospital. Most (76.5%) of the injured persons were transported to hospital by unknown persons and 16.0% by persons who were previously known to them. Police officers and health workers assisted 6.1% and 1.4% respectively at the crash site. Interval between occurrence of the crash and arrival at hospital ranged between < 5 minutes 10 hours, with a mode of 30 minutes. About half (51.9%) arrived within thirty minutes and 71.8% within an hour of crash occurrence. Seven (14.6%) of 48 health facilities demanded cash deposits or letters of guarantee of payment before providing treatment to road traffic injury patients. Deposits varied between US $ 6.7-667 and greatly varied from one health facility to another. While most seriously ill patients who could not afford to pay were granted waivers in public and some faith-based hospitals, private facilities always demanded signing of binding agreements and securities. Table 4 shows the cost accumulated by the time of interview. Out of 197 of the respondents, 44 (22.3%) owed the hospitals more than of US $ 133. However, only 19.7% of all those interviewed were in a position to pay the bills while 58.7% indicated that they would approach relatives and friends for financial assistance. Health institution services Information on outpatient hospital care was available on 91 patients (21 treated at public sector hospitals, and 61 and nine, at private and faith-based hospitals, respectively). Overall, 66.2% of casualties were attended within one hour of the crash. Relatively more delay in service delivery was experienced in public and faith-based hospitals compared to private hospitals where, respectively, 44.7, 44.4 and 4.8 percent of patients attended waited for more than one hour for services. Over half of all the respondents (59.2%) rated the quality of services as "Fair-Poor". Quality of care in faith-based hospitals was rated higher than that of the other providers (Table 5). Approximately 40.8% of all the health facilities visited rated themselves as being well prepared to handle road traffic crash emergencies. Self report by the hospital personnel on level of preparedness to handle trauma emergencies is shown in Table 5. The reported poor state of preparedness by public hospitals was supported by observation that many essential supplies were in short supply (Table 6) unlike in mission and private hospitals. Overall, as shown in Table 5, there was statistically no difference in anticipated duration of hospitalization (p=0.149) though there was a tendency for longer stay in public hospitals compared to private ones. Almost two thirds (61.3%) of those admitted for inpatient care were expected to stay in hospital for three weeks or more with 9.0% expected to stay more than three months. The longest anticipated duration of stay was in public hospitals where 51.9% expected to be in hospital for more than one month. On the other extreme, the projected duration of stay in private hospitals for half of the admissions was less than 10 days. In-patient treatment outcome The prognosis for injury outcomes for inpatients was assessed by the attending teams of nurses and doctors. Overall, complete recovery from severe injuries was projected to be low irrespective of the health facility in which a patient was being treated. Occurrence of disability ranged from impaired use of a body part to being completely bedridden due to quadriplegia. Though not severe for most, permanent disability was estimated by primary clinicians in 42/58 (72.4%) patients admitted into public health facilities compared to 13/14 (92.8%) and 13/15 (86.7%) admitted into mission and private hospitals respectively. There was a tendency towards transfer of long stay patients from private to public hospitals due to financial constraints. Study limitation There were two key limitations to this study. It was carried out between 1998 and 1999 and the situation may have changed substantially following political regime changes in Kenya and the recent political skirmishes. The findings of this study, never-the-less provide important baseline data needed in assessment of effectiveness of interventions in RTI prevention and management. There have however not been any targeted interventions on RTI evacuations, onsite first-aid nor service quality improvement. Any improvements that may have taken place would be attributable to incidental occurrences from a more positive political and economic environment over the last few years. Also, although a large number of health facilities was included, lack of random selection reduced the generalizability of the findings. It should be noted that the methodology used in this study did not offer all hospitals in the country an equal opportunity of being selected. Our approach however ensured that a large population of RTI patients was interviewed since selection criteria favoured larger institutions known to admit the bulk of RTI casualties in the country. Further, exclusion of North-eastern Province was not likely to have substantially affected the findings of this survey. The region is largely inaccessible, has very few hospitals, low road traffic and poor road infrastructure. As such the number of RTI casualties normally admitted for RTI treatment within the province is relatively small. Discussion Both the burden and case-fatality rate of RTI has been on the increase over the last four decades8 resulting in heavy socio-economic loss to the country. A national survey undertaken concurrently with this study found a total of 63,725 road traffic crashes between 1992 and 1996 in Kenya giving an average of 12,745 crashes per year (Macharia WM, Njeru EK, Musiime F and Omurwa T, unpublished observations). Most crashes with fatalities or severe injury occurred on major highways outside the urban centres; a finding which was also reported in a review by Odero in 199510. About 15% of the crashes were considered "fatal" in that at least one death occurred in the crash and 33% "severe" since at least one casualty required immediate hospitalisation. As found in this survey and others, young adults are at the highest risk of severe RTI. Among deaths from post traumatic causes in an accidents and emergency department of a university hospital in Nigeria, 57.8% followed road traffic crashes12. Almost half (47.2%) of the casualties interviewed were passengers. Crash vehicles in which 53.4% of those injured were travelling were identified as buses or commuter mini-buses (matatus). The observed over representation of males in road traffic crashes in this study may be attributable to a higher proportion of males travelling on the roads more often than females at any given time. It is also quite evident from this study that most of the persons involved in serious road traffic crashes were from low socio-economic background and hence the not surprising finding that 87.6% had no medical or accident insurance cover of any form. Public service vehicle passengers and pedestrians are also more likely to be the less well-to-do in society unlike private motor vehicle owners. Globally, poor population groups tend to bear a disproportionately higher burden of road traffic injury morbidity and mortality as reported by Nantulya and Reich9. While private and faith-based hospitals demanded high deposits before admission, public hospitals accepted non-monetary deposits more readily and hence the higher number (72.3%) of casualties in public hospitals. Heavy work load, unavailability of essential trauma management resources and low staff morale in public institutions may explain the observed longer waiting time in their outpatient departments as compared to faith-based and private hospitals. Trained health workers and police played a negligible role in provision of first aid and evacuation of severe accident casualties. Evacuation to hospitals too, was largely undertaken by either members of the general public, or other motorists who happened to be on crash site at the time. Only a small proportion (16.0%) of the casualties reported having received any form of pre-hospital treatment at all. First aid was nearly always given by non-medical persons, and only rarely by police or medically trained persons. In a similar study by Andrews et al (13), but which was confined to the city of Kampala, 80% of RTI casualties did not receive any pre-hospital treatment. Of the other 20%, the authors did not indicate what proportion actually received medical assistance at the scene of injury since care given at "other hospitals and health centres" was categorized under "pre-hospital treatment" too. This was contrary to what would be expected in a well functioning health care system. In more industrialized countries like United Kingdom, emergency medical services include provision of care by physicians at the crash scene14. Approximately 72% of patients in this survey arrived at health care facilities within an hour of crash occurrence and about two-thirds (66.2%) were attended to by medical personnel within one hour following injury. Considering that most crashes occurred outside urban centres, compared to other similar settings in the region, time taken to transport casualties to hospital (range 5-600 minutes) was relatively shorter for the majority of casualties. In the Kampala survey13, for example, the average time from injury to treatment for those without prior pre-hospital treatment was 155 minutes with a range between 15-1440 minutes. Waiting time in emergency departments may be attributable to many factors and may stretch up to three hours before completion of all necessary procedures, even in developed countries14. This study found that 51.9% and 71.8% of RTI patients were attended to within 30-60 minutes of arrival at the facility. Relatively more delay in service delivery was experienced in public hospitals. Lambe et al15 reported a mean waiting time of 56 minutes (95% CI=52-61) in an emergency department in California, USA, and recommended review of staffing arrangements to improve performance. Review of emergency department administration has been demonstrated to improve efficiency in care delivery16. A waiting time of 30 minutes for a general outpatient clinic was considered reasonable by Huang but should be even shorter for emergency visits17,18. Overall, most patients rated quality of care in this study as "good excellent" in faith-based and private hospitals. Adverse working conditions may have been responsible for the relatively longer delays observed in the public hospitals. Access to health care in many developing countries has progressively deteriorated with the introduction of health sector reforms19. Given that the vast majority of populations in the developing world are too poor to afford medical insurance as observed in this study, more equitable health care financing systems for medical emergencies, at the least, need to be sought 19,20. Ensuring that emergency medical supplies for trauma management are available in all major health facilities and those along major highways could go along way in curbing severe consequences of RTI. Prompt management of the RTI casualties would be expected to result in less fatality, disability and shorter hospital stay which would then translate into substantial economic savings. Conclusions Young persons from poor backgrounds constituted majority of casualties from road traffic crashes. Evacuation from crash sites was predominantly by other road users or members of the general public who provide little or no first aid. Public motor vehicle passengers and pedestrians were at an increased risk for severe road traffic injuries and are often admitted to public hospitals. Public hospitals being more financially accessible than mission and private hospitals handled a disproportionately higher RTI casualty load despite being more poorly equipped to handle such emergencies. Interventions to improve public transport safety and improvement of emergency health care access for the poor should be a priority for national road safety initiatives. It is further recommended that first aid training be undertaken for motorists and the general public. Public health facilities, especially those situated near major highways, should be preferentially supplied with medical supplies and other resources necessary for handling of RTI. Since the time when this study was conducted there have not been any targeted efforts to address this concern in the country. While availability of medical supplies may have some how improved as an indirect result of rising economic growth realized over the last six years, access to care and quality of services are unlikely to have changed much. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09020t5.jpg] [hs09020t3.jpg] [hs09020t2.jpg] [hs09020t1.jpg] [hs09020t6.jpg] [hs09020t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}