 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, Special Issue 1, Aug, 2009, pp. S2-S7 Psychological distress and adherence to highly active anti-retroviral therapy (HAART) in Uganda: A pilot study. Etheldreda Nakimuli-Mpungu, Brian Mutamba, Makanga Othengo, Seggane Musisi Makerere Univerity College of Health Sciences, School of Medicine, Department of Psychiatry, P. O. Box
7072 Kampala, Uganda An oral presentation of this paper was made at the 11th Annual International Meeting of the Institute of Human Virology. Fogarty Scholarship Luncheon, September 11-13,2008 Harborplace Renaissance Hotel, Baltimore, Maryland. Fogarty AIDS International Training program (AITRP) provided support to attend the meeting. The Fulbright Science and Technology Award provided support to carry out the study. Code Number: hs09023 Abstract Background: Mental health related risk factors for non-adherence to highly active anti-retroviral therapy (HAART) have not
been investigated in Uganda and yet adherence is critical to the success of the current scale up in the provision of HAART to HIV
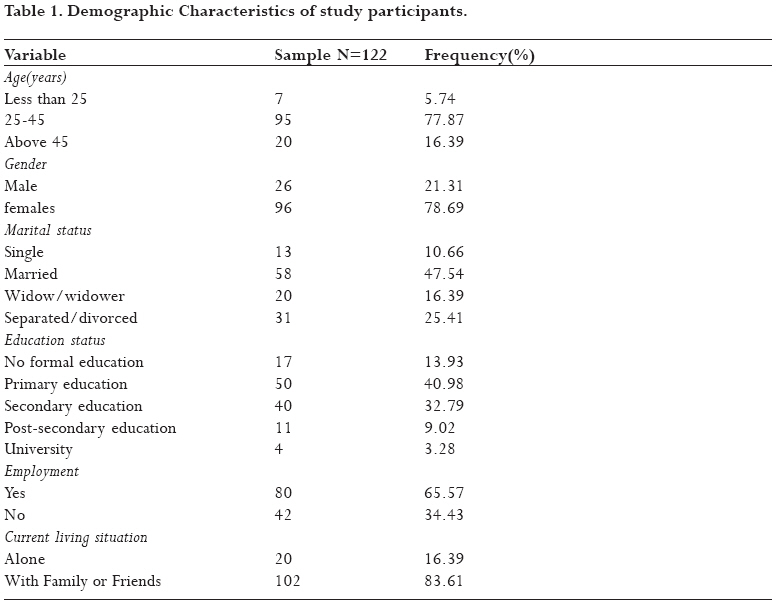
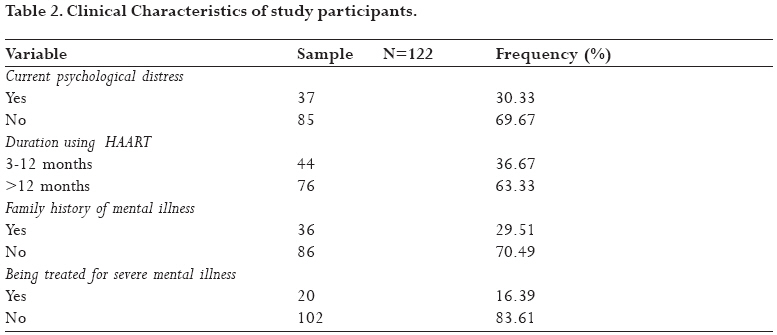
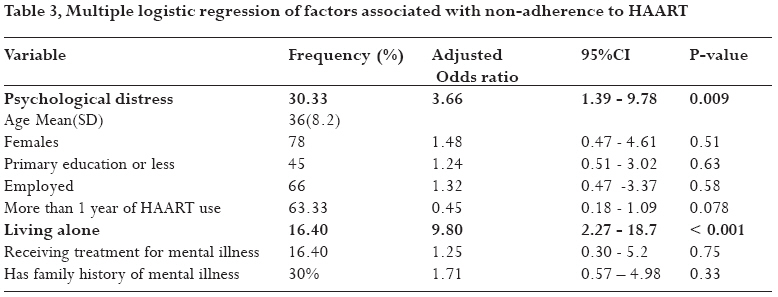
positive individuals in rural areas of Uganda. African Health Sciences 2009; 9(S2): 2-7 Introduction:Sub-Saharan African countries are home to more than 60% of all people living with HIVestimated at some 22 million.1 Uganda is one of those countries that have successfully applied various HIV prevention efforts which have dramatically decreased the HIV prevalence rate from 20% in 1992 to a current rate of 7% among adults aged 15-49 years. 1 As we continue to fight the epidemic, emphasis is towards increasing access to highly active antiretroviral therapy (HAART) which has been shown to effectively reduce morbidity and mortality due to AIDS2,3 Presently, activities to scale up provision of HAART are taking place country wide with support from Ministry of Health working with various Non governmental organizations, the World Health Organization (WHO); the Global Fund to Fight AIDS, Tuberculosis, and Malaria; and the (U.S.) President's Emergency Plan for AIDS( PEPFAR).4 The benefits of these efforts critically depend on patients achieving and maintaining high levels of adherence. Sub-optimal adherence is highly associated with incomplete suppression of viral replication, declining CD4 cell counts and clinical progression to AIDS5,6. Therefore HAART programs that are being set up in the country may have to take a holistic approach in addressing all potential barriers to adherence to these medications. The few studies that have investigated adherence to HAART in Uganda have not quite assessed mental health issues as possible risk factors for non-adherence. For example, the most recent publication7 reports that patients were screened for depression and alcohol use but they do not report what proportion of patients screened positive for depressive symptoms, what proportion had alcohol use problems but they reported that these mental health problems were not associated with non-adherence. It is clear such findings should be taken with a pinch of salt. In fact mental health screening is not integrated into the majority, if any, of the numerous HIV /HAART programs that are being set up. It is common practice that patients will only have their mental health needs addressed if they have overt symptoms or when they have already received a diagnosis of a severe mental illness. If mental health needs of HIV positive patients are ignored, this may subsequently have a negative impact on the HAART programs. Previous studies have shown that people with HIV infection often suffer from depression and anxiety symptoms which may or may not meet criteria for clinical disorders as they adjust to the diagnosis, adapt to life with a chronic disease and anticipate and receive news of death of friends and family8,9,10. Given that access to mental health services are limited and mental health care is not integrate into HIV treatment in most health care facilities, mental health issues affecting adherence remain poorly understood. We have previously described the clinical presentation of HIV positive individuals with overt and severe HIV related psychiatric syndromes such as HIV-related mania11,12 HIV dementia13 and HIV depression14 at Mulago and Butabika Hospitals. This pilot study was initiated to assess the likely success and feasibility of a much larger study investigating the prevalence of covert mental health problems such as psychological distress among HIV positive individuals in rural populations using HAART and whether these problems are associated with non- adherence to HAART. Given that the HIV positive status has been associated with an increased risk of mental health problems and the fact that HIV positive individuals are not routinely offered mental health screening, we hypothesized that our study sample may have substantial psychological distress and that this may be associated with non-adherence to HAART. The goal of the study is to provide information that can be used in designing HAART programs which at least offer mental health screening with counseling geared at providing stress management skills. Methods Over a one month period, we performed a cross-sectional study of HIV positive adult individuals aged 18 years and above, who were using HAART and received HIV care every Wednesday at the HIV clinic located in the Butabika Hospital Outpatient center. Butabika Hospital is the national referral mental and teaching hospital. Its outpatient center houses the mental health clinic and general medical clinics which offer general medical services to the community. Among the medical clinics, is the HIV clinic which was established in 2005 by the Ministry of Health and provides free anti retroviral drugs. Presently there are approximately 800 HIV positive patients registered with the clinic and 500 patients are using HAART .All patients who came to the clinic during the study period were approached by research assistants who asked them whether they were using HAART. If an individual was using HAART, the research assistants went on to explain study procedures and invited the person to participate in the study. To control for confounding by HAART regimen, only individuals using a combination of neverapine, lamivudine and stavudine were invited to participate in the study. All individuals who were approached gave informed consent and none refused to participate. Instruments The Self Report Questionnaire (SRQ-20) was used to screen for psychological distress during the previous month. The SRQ20 was developed by the World Health Organization to screen for common mental disorders (depression and anxiety) in primary health care. 15 The questionnaire is not a substitute for, or equivalent to, a clinical diagnosis. An endorsement of 6 or more symptoms on this questionnaire indicates the presence of a probable mental disorder and thus would require further evaluation. This instrument has been validated in Uganda and a cut off point between 5 and 6 yielded high sensitivity (80%) and a reasonably good specificity (74%) in detecting psychiatric co-morbidity among general hospital outpatients. The Negative predictive value was 53% and the Positive predictive value was 87%.16 In this study, Individuals who endorsed 6 or more symptoms were classified as having psychological distress. Measurements All individuals were assessed by a standardized socio-demographic questionnaire. The main explanatory variables was psychological distress, other explanatory variables were age, gender, education status(primary level and below versus secondary level and above), marital status(single versus others, married versus others widowed versus others separated/divorced versus others), employment status(employed versus unemployed) family history of mental illness, history of having a severe mental illness, living situation(living alone versus living with family / friends) duration of using HAART (less than or equal to 1year versus greater than 1year) Adherence to HAART was assessed by using the missed-dose method which is simple and straightforward. Participants were asked to report the number of missed doses within a specified time period. Adherence is usually calculated as a percent discrepancy score, which is the number of doses the patient had reportedly consumed, divided by the number they should have consumed during a specified time interval. Adherence "scores" were converted to a dichotomous variable (e.g., adherent/non-adherent) to simplify their interpretation. When converting discrepancy scores, many researchers have used either 80% or 90% as the cut off point to distinguish between adherence and non-adherence.17,18 In this study, we used 90% as the cut off point. The outcome measure examined in this study was rates of non-adherence in the previous one month. Statistical Analysis Statistical analysis was performed by using Stata 10.0 (Stata Corp., College Station, Texas). Frequencies of clinical and demographic variables were computed, and bivariate analyses were conducted to identify demographic and clinical variables that were significantly correlated with non adherence in order to control for their contribution in multivariate models. For the bivariate analyses, we used chi-square tests or Fisher's exact test for qualitative variables, independent- sample t tests for continuous variables. Variables that had a significant bivariate association with non-adherence were then included in a multivariate logistic regression model. Results Overall, 122 HIV positive individuals using HAART were asked to participate in the study. None declined to participate. The prevalence of non-adherence to HAART since initiation of treatment and in the previous month prior to the study was 30% and 17.2% respectively. 30.3% screened positive for psychological distress. The social demographic characteristics of the study population are shown in Table 1. The mean age of study participants was 36 years (SD= 8.2). The majority of the 122 participants were female, with a male to female ratio of 1:4. Nearly half of the sample had primary level education and below. Table 2 shows the clinical characteristics of the study participants. 20% were receiving treatment for a severe mental illness at the outpatient mental health clinic.30% reported a family history of mental health problems. Table 3 summarizes the results from multivariate analysis. Results from the multiple logistic regression analysis of factors associated with non-adherence since initiation of treatment are similar to results from the multiple logistic regression analysis of factors associated with non-adherence in the previous one month, except that in the latter its only psychological distress that was significantly associated with non-adherence (OR 3.70, p-value 0.028). Having a severe mental illness being treated at the adjacent mental health clinic was not significantly associated with non-adherence. Bivariate analysis showed that only psychological distress and living alone were statistically significantly associated with non-adherence to HAART (x² = 8.31,p-value 0.004 and x²=8.03,p-value = 0.005 respectively). No other demographic or clinical variable was significantly associated with non-adherence to HAART. Gender(x²= 0.52,p-value= 0.47), age was categorized as less than 45years versus more than 45 years(x²=1.77,p-value= 0.18) education status was categorized as primary education or less versus secondary education or more(x²=0.16,p-value 0.68) Marital status was categorized as single versus otherwise(x²=1.99,p-value=0.18),married versus otherwise(x²= 0.58,p-value=0.45 ) widowed versus otherwise(x²= 0.08,p-value=0.77 ) divorced/separated versus otherwise(x²=0.14,p-value = 0.71 )Having a family history of mental illness versus otherwise(x² = 0.86,p-value,0.35). Receiving treatment for a severe mental illness versus otherwise (x²= 0.5,p-value=0.35 ) Using HAART for more than 1 year versus for less than one year (x²=2.24,p-value=0.09) Discussion This pilot study of psychological distress and adherence to HAART had 2 major findings. First, psychological distress (symptoms of anxiety and depression) and living in isolation were significantly associated with non- adherence to HAART among HIV positive individuals attending the HIV clinic situated in the Butabika Hospital Outpatient center,after adjusting for potential confounders. This finding is consistent with findings from prior studies of adherence in HIV positive individuals in developed countries which have linked lack of social support, for example, living in isolation, depressive and anxiety symptoms with poor adherence.19 20 21 Weaver and colleagues22 went further to demonstrate that the relationship between these negative mood symptoms and adherence was mediated by increases in avoidance-oriented coping strategies such as denial and behavioral disengagement. Further more, Murphy and colleagues23 reported that those with greater social support for example having reassurance from family members, those having reliable alliances were more likely to be adherent over the past one month. This suggests that mental health problems may be a key deterrent factor in achieving optimal adherence rates to HAART and ultimately in achieving successful ART programs. It's important to note that adherence rates in this study population are comparable to adherence rates in other HIV treatment programs in Uganda.7 24 This implies that if mental health needs are assessed and appropriate treatments given, then these rates could be even boosted further resulting in less drug resistance, better viral suppression and longer survival. Second, although receiving additional treatment for a severe mental disorder was associated with 25% increase in risk for non-adherence, this was not statistically significant. Possible explanations for this is that these individuals were receiving treatment for their mental illness from the adjacent mental health clinic and therefore their illness was under control and they were able to have good functioning levels. Previous studies have shown that individuals accessing mental health care as well as HIV care in one facility have improved outcomes. 25 26 One of the strengths of this study is the inclusion of HIV positive patients with severe mental illness as the majority of prior studies have excluded these individuals from studies of adherence to HAART. The results show that these individuals can achieve rates of adherence comparable to other individuals without severe mental illness. This further demonstrates the importance of timely and adequate treatment of mental health problems in HIV positive patients regardless of severity so as to prevent further complications. This study has several limitations. First, our data are drawn from a single HIV clinic that treats patients in a city environment; our results therefore may not be applicable to other populations of HIV positive individuals. Second, this being a pilot study, we did not gather information on alcohol or drug use, measures of immune status, other medications or medication side effects, or HIV disease stage, all of which have been reported to be associated with adherence to HAART and therefore should be adjusted for in future studies.27 28 Third, self report is not the most reliable measure of adherence therefore our adherence estimates may be overestimated. However, there is no gold standard for adherence assessment yet and different assessment methods have been used across a range of studies. 28 Lastly, we did not screen participants for HIV dementia which has been found to be prevalent among HIV positive individuals attending HIV urban clinics in Uganda and has been documented as a risk factor for non-adherence. 29 30 Within the context of these limitations, this study provides information that is relevant in implementation of HAART programs in Uganda. Conclusion Replication of the study using a better epidemiological design such as case-control design is of paramount importance as this would provide further evidence for integrating mental health services into existing HAART programs in Uganda. Screening for psychological distress could be integrated with voluntary counseling and testing or on going counseling for HIV infection. In other words, each counseling opportunity could be used as a chance to screen individuals for psychological distress. Individuals identified with high level symptoms initially receive counseling oriented towards psych-education, stress reduction skills and coping skills. Although this may come with additional costs of training HIV care providers in screening and recognizing mental health problems, the benefits of sustaining and maintaining optimal levels of adherence to HAART in such a low resource setting may overshadow those costs. References:
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09023t2.jpg] [hs09023t1.jpg] [hs09023t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}