 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, Special Issue 1, Aug, 2009, pp. S8-S15 Non-adherence to anti-TB drugs among TB/HIV co-infected patients in Mbarara Hospital Uganda: Prevalence and associated factors Monica G Amuha1, Paul Kutyabami 1, Freddy E Kitutu1, Richard Odoi-Adome 1, Joan N Kalyango1,2 1. Department of Pharmacy, Faculty of Medicine, Makerere University Code Number: hs09024 AbstractBackground: Non-adherence to treatment remains a major obstacle to efficient tuberculosis control in developing countries.
The dual infection of Tuberculosis and HIV presents further adherence problems because of high pill burden and adverse effects. This
poses a risk of increased multi-drug resistant TB. However, the prevalence of non-adherence and its associated factors have not been
studied in these patients in Uganda. African Health Sciences 2009; 9(S2): 8-15 Introduction Non-adherence to treatment is a problem in Tuberculosis (TB) management as with other long term illnesses. TB treatment presents particular challenges for adherence because the treatment is long and involves taking a number of medications, side-effects are common and the patient usually feels better long before treatment has been completed1. Non-adherence has been cited as one of the reasons for failure of achievement of the global treatment success rates by Uganda2. In 2005, Uganda attained a treatment success rate of 73%2. Although this was an improvement on the success rates of 68% achieved in 20032, it is still short of the 85% global target for treatment success3. Patients with TB are expected to have adherence levels greater than 90% in order to facilitate cure4. Failure for cure increases the risk of development of drug resistant strains, spread of TB in the community and this in turn increases morbidity and mortality. The burden of TB in Uganda is already very high with the country ranking 15th among the high burden countries 2. Any further increases in the burden of TB would overstretch the health system that is already over laden with TB patients. The problem would be worse with the Multi-Drug (MDR) and Extensively Drug resistance (X-DR) TB cases that are likely to develop with non-adherence and yet are difficult to treat5. The problem of TB is made worse by the concurrent infection with HIV6. It is estimated that 50% of TB patients are co-infected with HIV. Both diseases place a big social, economic and health burden on the country. Patients with HIV and TB are likely to face more challenges because they have to get HIV care in addition to the TB care. This may lead to poorer adherence among these patients and yet because of their immune suppression, are likely to get more severe forms of TB. Studies that have been done elsewhere have found the prevalence of non-adherence of 21.2 32.9% 7, 8. A number of factors associated with non-adherence have been cited in the literature. These include health system, condition related, patient related, socio- economic and therapy related factors9. Many of the studies have been done in patients infected with only TB. We therefore do not know the prevalence and factors associated with non-adherence to TB treatment among TB/HIV co-infected patients in Uganda. The study was thus conducted among patients that were co-infected with TB/HIV to obtain this information in order to provide a basis for possible interventions by the TB program in the management of TB in HIV infected patients.
Methods A cross-sectional study with quantitative and qualitative methods of data collection was carried out among TB/HIV co-infected patients receiving TB treatment at the National Tuberculosis and Leprosy Centre of Mbarara hospital. The center provides in-patient and out-patient TB care and has since September 2007 worked jointly with the Immune Suppressive Syndrome (ISS) clinic for the dual management of TB/HIV co-infection. The total number of TB/HIV co-infected patients registered in 2007 was 235. Consecutive sampling was used to select 140 patients. The inclusion criteria for the study subjects was TB/HIV co-infected patients 18 years and above, receiving TB treatment at Mbarara hospital in the months of January and February 2008 that gave written informed consent to participate in the study. Patients that were too sick and unable to communicate were excluded from the study. The study was approved by the Mbarara University Research Ethics Committee.
Data collection Quantitative data was collected by trained research assistants using a pre-tested, semi-structured questionnaire. The questionnaire was translated to the area's local language (Runyankore) and back translated to English to ensure consistency of meaning. Qualitative data was collected through key informant interviews using a topic guide. The participants included the doctor in charge of the TB ward, one dispenser and a nurse. The participants for qualitative data were selected purposively. Data was collected on patient socio-demographics e.g. sex, age, educational level, marital status, religion; patient factors e.g. level of income, patient beliefs, perception, attitude and knowledge about TB, forgetfulness, family/social support, life style habits, medical expenditure on treatment of TB; program factors e.g. distance to the treatment centre, availability of drugs, waiting time at the centre, and cost of travel to the centre; health service factors e.g. attitude of health workers, attention and support provided to the patients, health information on TB and treatment regimen; drug related factors e.g. adverse drug reactions, type of regimen, number of pills, patient's physical response to treatment and whether patients are on antiretroviral therapy (ART). The outcome variable was non-adherence and this was measured using patients' self reports of how they had been taking their drugs in the five days preceding the interview. Patients were asked to recount if they had been unable to take any of their medications on a day by day basis over the five days and those that reported missing more than 10% (had taken less than 90%) of the prescribed medicines were considered to be non-adherent. Adherence was calculated as the percentage of prescribed drugs over the five day period that a patient took.
Statistical issues The sample size was computed using the formula for proportions that estimates sample size for an infinite population with a 5% level of precision and 95% confidence level10. The obtained sample size was scaled down to cater for the small number of patients that can be accessed at this clinic. Based on results from a study that was conducted among adults and children in Uganda8, the estimated sample size was 122 patients. The quantitative data was double entered in EpiData version 2.1b (The EpiData Association, Odense, Denmark) and exported to STATA statistical software version 8 (Stata, College Station, TX, USA) for analysis. Skewed numerical data was summarized as medians while categorical data was summarized as percentages and frequencies. The prevalence of non-adherence was computed as the percentage of patients that were non-adherent (i.e. taking less than 90% of prescribed medicines) over the whole sample size. Bivariate analysis was done to determine the association between each of the independent variables and non-adherence using cross tabulations and logistic regression. The factors with p-values not greater than 0.25 at bivariate analysis were considered for multivariate analysis. Logistic regression was used for multivariate analysis to determine the independent predictors of non-adherence and assess for confounding and statistical interaction. Odds ratios, their 95% confidence intervals, and p-values were determined. A 5% level of significance was used and all tests were two sided. A variable was considered an independent predictor if it remained in the multivariate model using stepwise selection methods. The variables that were eliminated from the model at this stage were assessed individually to determine if any of them changed the odds ratios of the independent predictors by more than 10%. The qualitative data was transcribed and analyzed manually by separation into emerging themes. It was then used to further explain the results from the quantitative data analysis.
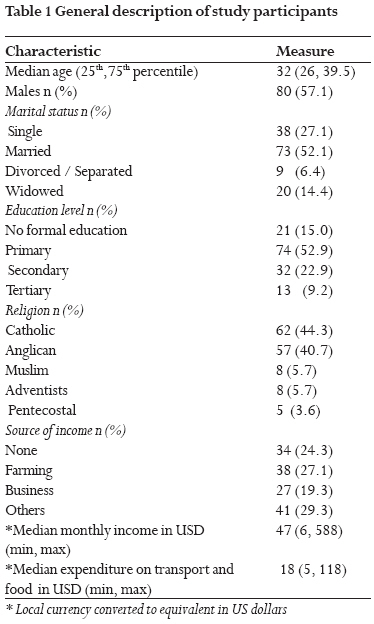
Results A total of 140 participants were enrolled into the study. The median age of the study participants was 32 years (25th percentile=26, 75th percentile=39.5); 57.1% (n = 80) were males; 52.9% (n = 74) had primary education as the highest level of education attained; 52.1% (n = 73) were married; 44.3% (n = 62) were Catholic; 75.7% (n = 106) had a source of income and 35.9% (n = 38) of those with source of income were farmers. The general description of participants is summarized in Table 1 The prevalence of non-adherence to anti-TB drugs was 25% (n = 35, 95% CI=17.8-32.0%). In addition, 15 of those not adhering to treatment (42.9%) had adherence levels of 0% having not taken any drugs in the five days prior to the interview. The most cited reason for not taking drugs was drugs getting finished (n = 23, 65.7%) followed by forgetting (n = 6, 17.1%). Those whose drugs were finished cited lack of transport money to collect more drugs as the most common reason why their drugs were finished (n = 17, 73.9%). Other reasons for not collecting drugs included being busy at work (n = 3, 13.0%), having family emergency (n = 1, 4.3%), sickness (n = 1, 4.3%) and forgetting the appointment date (n = 1, 4.3%).The key informants said the level of non-adherence among these patients was not very high. "I would say that about 3 in every ten patients do not adhere to treatment," said one key informant. "The level of non-adherence is low among these patients," said another key informant.
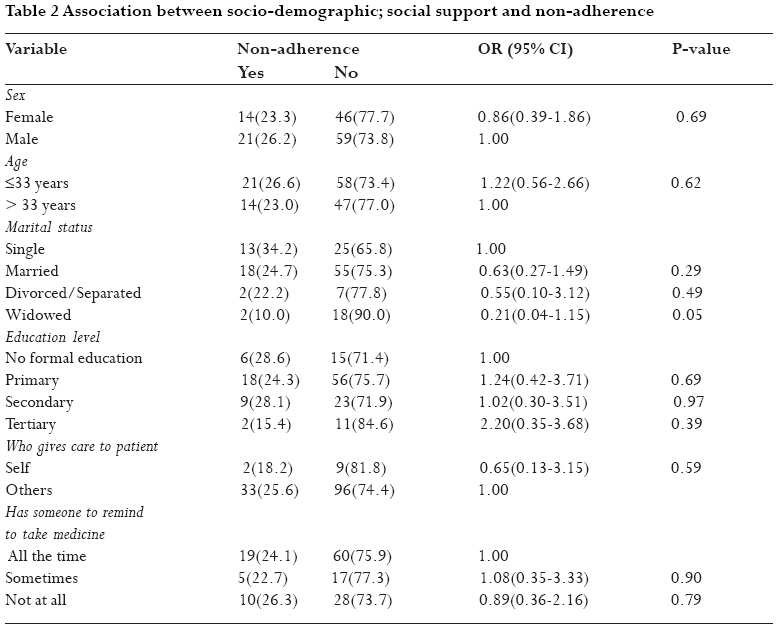
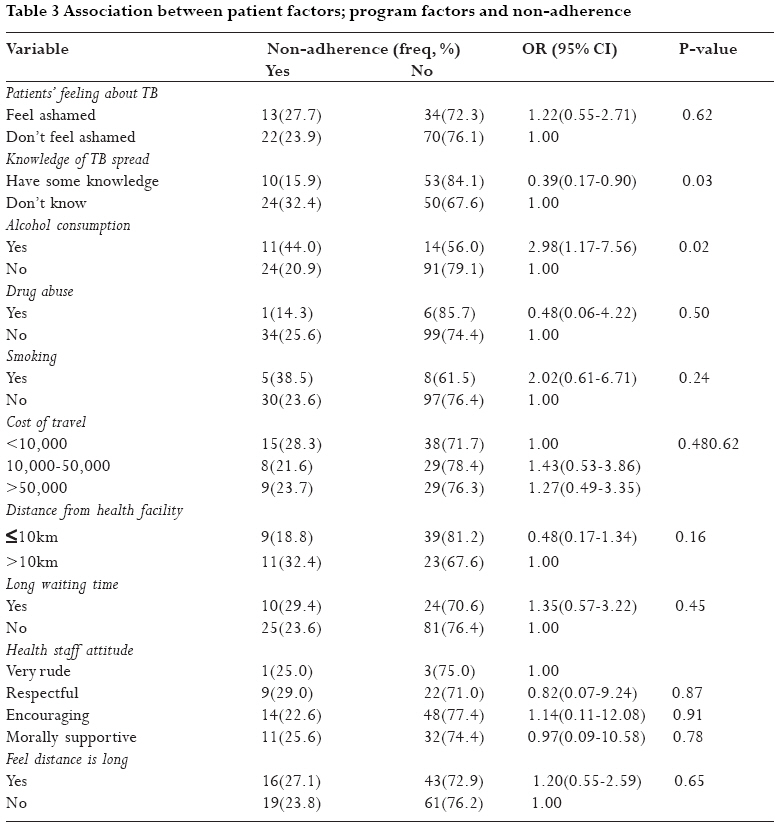
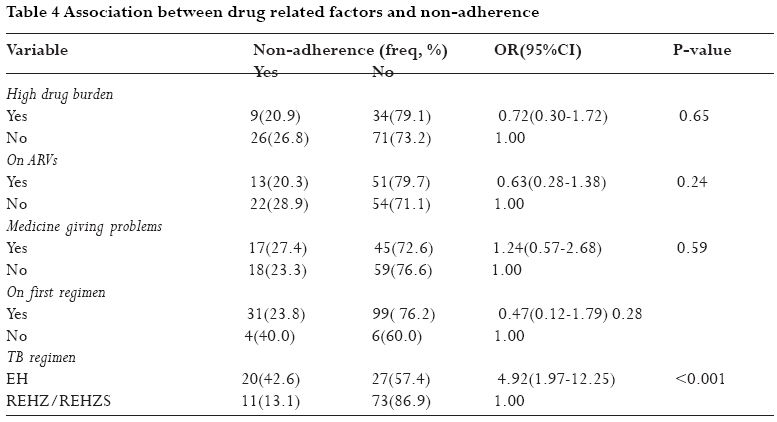
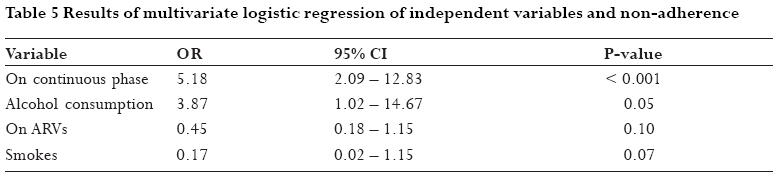
Factors associated with non-adherence At bivariate analysis none of the socio-demographic factors and program factors was significantly associated with non-adherence. Among the patient factors, knowledge of how TB is spread (OR = 0.39, 95% CI = 0.17 - 0.90) and alcohol consumption (OR = 2.98, 95% CI = 1.17 -7.56) were significantly associated with non-adherence. Patients who knew how TB is spread had a 61% reduced odds of non-adherence. On the other hand, those who consumed alcohol were almost three times as likely not to adhere as those who didn't. The phase of the TB regimen was the only drug related factor significantly associated with non-adherence. Patients on continuing phase were 4.92 times (95% CI = 1.97 12.52) as likely not to adhere as those on intensive phase. Results of bivariate analysis are summarized in Tables 2, 3 and 4. Having some knowledge of how TB is spread, alcohol consumption, distance to the health facility, smoking, being on ART and the phase of TB regimen were considered for multivariate analysis. When these variables were simultaneously controlled for, the only independent predictor of non-adherence was being on continuing phase of anti TB treatment (OR = 6.24, (95% CI = 2.41 16.15). Alcohol consumption, being on ART, and smoking were retained in the multivariate model as confounders of being on a continuing phase of anti TB treatment. In addition, there was a confounding relationship between alcohol consumption and smoking. Thus it was found important to control for these variables to validly assess the relationship. Alcohol consumption had borderline significance (OR = 3.87, 95% CI = 1.02 14.67). The results of multivariate analysis are summarized in Table 5. From the qualitative data, some key informants felt that patients who were on antiretroviral drugs were more likely to adhere to treatment. "Patients on both ARVs and TB drugs are counseled more often than those only on TB drugs, this makes the former take their medicines better than those on only TB drugs," said one key informant. Another key informant felt that the patients on continuing phase of anti TB drugs were more likely not to adhere. "When these people feel better, especially after finishing the intensive phase, they start taking their drugs irregularly". The other reasons cited by the key informants for missing medicines were transport, distance form the health facility making it hard for the patients to collect their drugs, adverse drug reactions and pill burden. "Patients complain of the drugs being many. They are tired of taking the drugs," said one key informant. "Transport is also a problem, especially for people who come from far. It has been made worse by this fuel crisis and I know a number of people have missed their appointment dates because they can't afford the transport costs". "Some patients say that the side effects are too much and they just can't continue with the drugs", said another key informant DiscussionPrevalence of non-adherence One in every four patients was not adhering to treatment. This finding is comparable to a similar study where 21.2% admitted non-adherence to treatment during the previous month8. The slight difference in the non-adherence levels between the two studies is probably due to the difference in time period over which adherence was assessed. Whereas we used 5 days, that study used one month. In addition, it is expected that the true level of non-adherence may be higher than what was observed in this study. This is because non-adherence was measured using self reports and with this method patients are likely to overestimate their adherence11. This may result into some patients being misclassified as adherent when in truth they are non-adherent. One study done to assess whether the overestimation of adherence using self reports would be apparent when objective measures of adherence were used found out that there was an over estimation of 27% in the level of adherence when self reports were used 12. However patients who recognize and report their non adherence easily accept and implement interventions for the improvement in their daily lives11, 13, 14. These levels of non-adherence are very worrying because the likelihood of development of Multi-drug resistance TB and X-Drug resistant TB is increased. This will further increase the burden of a disease that is already very big and increase the costs of its management5. It is thus necessary to institute adherence support measures to lower the non-adherence levels. Although the key informants felt the level of non-adherence was low, it has been found that physicians usually do not predict the adherence levels of their patients accurately based on their knowledge of these patients11. Factors associated with non-adherence to anti-Tb drugs among TB/HIV co-infected patientsSocio-demographic factors There was no association between social demographic factors and non-adherence. This is in line with many other studies done in both developed and developing countries that found no association between adherence scores and age, gender, educational level, marital status, religion and occupation15-17. However some studies have shown an association between socio- demographic factors and non adherence18. A study in rural Turkey showed that females were more adherent to their medication compared to their male counterparts18. This was mainly due to the gender difference in smoking where male smokers were more non-adherent than females. This gender difference in smoking was not evident in this study as smoking was not significantly associated with non-adherence. The socio-demographic factors studied in this study were similar to those in that study. Failure to find an association between socio-demographic factors and non-adherence in this study could also be due to the low sample size. This would mean that we do not have sufficient power to detect an association if it truly exists. However it is possible that non-adherence is independent of socio-demographic factors in this population.Patient Factors There was an association between knowledge of how TB is spread and non-adherence at bivariate analysis. However this was not significant at multivariate analysis after controlling for other factors. The findings at bivariate analysis showed that those who had some knowledge about the way TB is spread had a 40% chance of being non-adherent compared to the ones who did not know. However, several other studies have found an association between knowledge of TB spread and non-adherence. A study done in Eastern Nepal found that the majority of non-adherents were not well informed about their disease, effects and treatment15. Failure to find an association between knowledge of TB spread and non adherence at multivariate analysis in this study could have been due to the difference in the research design used. Whereas we used a cross-sectional study design, that study used a case control study. We may not have had sufficient power to detect an association if it truly existed. Consumption of alcohol was found to have an association with non adherence at bivariate analysis but at multivariate analysis it was found to be a confounder. However other studies have found a significant association between alcohol consumption and non-adherence. Adherence scores have been found significantly higher in patients who indicated no alcohol consumption (P=0.007)16. Another study found that patients who were not amenable to suggestions to stop drinking alcohol and continuous consumption showed non-adherence to their medication19. This difference in association could also be attributed to the difference in sample size. We used 140 patients whereas that study used 341 TB patients. The confounding relationship between phase of TB regimen, alcohol consumption and non-adherence is probably because of the relationship that may exist between alcohol consumption and the improvement in one's health status as they progress through the phases of TB treatment. It is likely that as patients take longer on treatment they may revert back to their drinking habits possibly because they feel their health status has improved as opposed to those who have just started. There was no association between smoking, drug abuse and non-adherence in this study. The confounding relationship between alcohol consumption, smoking and non-adherence is probably because many subjects that smoke usually also drink alcohol. Some studies have demonstrated that these psychosocial factors such as alcohol consumption, smoking, drug abuse and other factors have been associated with non-adherence to therapy18-20. Drug abuse was not common in this sample and this could be the reason why a significant association was not found. Drug Related Factors The type of TB regimen was shown to be significantly associated with non-adherence at both bivariate and multivariate analysis. Patients on continuous phase were about 6.2 times as likely to be non-adherent to their regimen as patients on the intensive phase. These findings are similar to those observed in another study carried out in Uganda which found that patients on continuous phase were 1.52 times (P=0.003) more likely to be non-adherent compared to those on intensive phase 15. The reason for this difference in adherence is probably due to the fact that the patients on intensive phase usually still feel very ill and are thus motivated to take their drugs. There was no significant association between non-adherence and pill burden or being on ART at bivariate analysis. This could be due to the low sample size of the study as we did not have sufficient power to detect an association if it truly existed. The Key Informants stated that patients on both TB treatment and ART were more likely to be adherent due to the intensive counseling undertaken at initiation of therapy and during continuous monitoring of therapy. This difference in adherence levels, calls for more effort in the counseling measures undertaken at the health center, for both groups of patients. At multivariate analysis, the confounding between being on ART and phase of the TB treatment was probably because at times the ART may be differed for some time while the patient is initiated on TB treatment to avoid the noxious effects that may arise through treatment of both diseases at the same time. In addition, the process involved in counseling and preparing the patient for ART may take some time while TB treatment can be initiated immediately. Thus patients may start ART during or close to the continuous phase. Although the pill burden did not have an association with non-adherence in this study, other studies have found a significant effect of pill burden on the level of adherence to medication19. The study in India found that patients were likely not to take their medication because they were too many and associated with various adverse effects. Failure to find an association in this study may be due to small sample size used. In addition, many of the previous studies have been done among patients with only TB while our study was among TB/HIV co-infected patients. These patients may have different motivation for taking their drugs. However, information obtained from the Key Informants was associating non-adherence to the high pill burden. Adverse effects did not have an association with non-adherence probably because the patients had been counseled to expect them and also on the measures to take when they experienced these effects. Key informants reported on counseling of the patients on the procedures to undertake when specific adverse effects were observed. However other studies have found an association between non-adherence and adverse effects15. Health Provider/Program Factors There was no significant association between attitude of health providers and non-adherence in this study. This is not in line with other studies that have shown that behavior and attitude of health providers has an important bearing on adherence15, 19. These studies found that a break down in the healthcare provider-patient relationship lead to significant levels of non-adherence. The interaction between health care providers and the patients is crucial to treatment adherence. Program factors such as cost of travel, distance to the health facility and waiting hours did not have a significant association with non-adherence. This conflicts results from other studies that showed significant associations8, 15, 19. Non-adherent patients have been found to have longer travel to the health facility19. The key informant also cited transport costs as an important hindrance to adherence. It is thus possible that although this may be an important factor among this population, we did not have sufficient power to detect any association. The drugs were obtained free-of-charge and were readily available at the TB center, thus this did not affect non-adherence. This is backed up by the information obtained from Key Informants. The study was limited in that self reports were used which usually overestimate adherence levels. In addition we used a cross sectional study thus we were not able to assess temporal relationships between variables. The associations found cannot therefore be assumed to be causal. The sample size was small and may therefore not have been able to detect important associations. In conclusion, the level of non-adherence among these patients was high. Interventions to reduce it need to be instituted. These should mainly target those patients on continuous phase who were at higher risk of non-adherence, smokers, those who consume alcohol and those not on ART. Transport costs for patients could be reduced by bringing the services closer to where they live or by providing transport to those who live far. The study could be conducted using a bigger sample size and more rigorous study designs so that important associations can be detected. Acknowledgements We would like to acknowledge the Mr Levi Mugenyi for his participation in data analysis. The research assistants Carmen and Julius for their role in data collection and the staff of Mbarara hospital for all the assistance accorded us that enabled us to do the study. We are also grateful to the study participants who gave their precious time. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09024t2.jpg] [hs09024t3.jpg] [hs09024t5.jpg] [hs09024t1.jpg] [hs09024t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}