 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, Special Issue 1, Aug, 2009, pp. S16-S22 The prevalence and severity of mental illnesses handled by traditional healers in two districts in Uganda Catherine Abbo1, 2, Solvig Ekblad 3, 1, Paul Waako2, Elialilia Okello2, Seggane Musisi2 1 Karolinska Institutet, Stockholm, Sweden Code Number: hs09025 Abstract Background: Little is known about the prevalence and severity of DSM-IV mental disorders treated by traditional healers
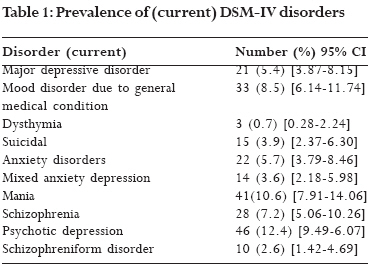
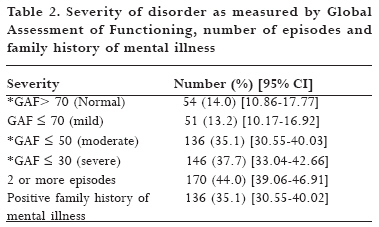
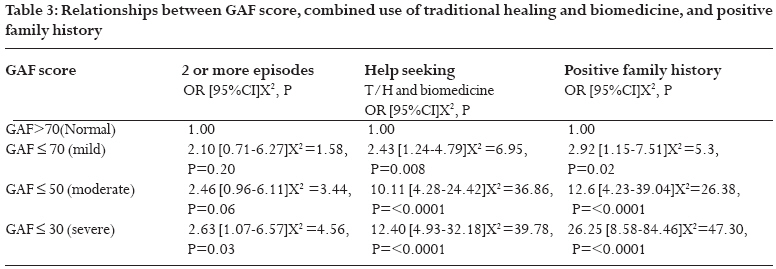
in Uganda. African Health Sciences 2009; 9(S2): 16-22 Introduction Populations throughout Africa use traditional healers to help meet their primary health care needs 1, 2. Besides being accessible and available, traditional healers are often part of the wider cultural belief system and are considered integral to everyday details and well being. Mental illnesses are a major public health concern in Uganda, both in communities and in health care facilities. Yet very few reliable prevalence studies are available with which to estimate the burden of mental illnesses in Uganda 3. The bulk of epidemiological research in Uganda has focused on primary care settings, where most psychiatric disorders are non-psychotic 4, 5. The reported prevalence rates vary widely, from 10% to nearly half of all primary care attendees (the quoted figures range from 10-25% of patients attending with a psychiatric problem, with or without a co-existing physical problem). The most common diagnoses are Depression and Anxiety 6-8. A community study from rural Uganda by Orley and Wing found the following prevalences: Depression 9.3%, Anxiety 8.5%, Bipolar disorder 4.9% and Schizophrenia 1.5 % 9. In a study of households in the Kabarole district of Uganda, Kasoro and others found that 30.7% of adults had psychiatric disorders 10. On the basis of the UNHS 2005/2006 Qualitative Module Report, the Uganda Bureau of Statistics found, for example, that 58% of all the households with disabled members (an estimated 7 % of all households in Uganda), had at least one member with a mental disorder 11. None of these Ugandan studies specifically addressed traditional healers' practices, neither did they highlight severe psychiatric illnesses (Psychosis). Instead, they concentrated on common mental disorders. Furthermore, it is possible that many patients with psychosis do not spontaneously seek primary health care 12. Thus, there is a paucity of literature on the prevalence of mental health care provided by traditional healer centres/shrines in Uganda. However, a study in urban Tanzania found that among persons attending a traditional healer centre in Dar-Es-Salaam, the capital, the prevalence of common mental disorders was 48%, which was twice the prevalence among persons attending the neighboring primary health clinic 13. Patel and others found a prevalence of 40 % in Harare 14. None of the studies reported on the severity of disorders among person attending traditional healer's shrines. The aim of this study was therefore to try to document the prevalence and severity of various specific mental illnesses among persons attending traditional healers, with the emphasis on major psychiatric disorders, the Psychoses, with the aim of providing policy makers with information about the burden of mental health problems born by traditional healers. Objective To determine the prevalence and severity of various specific mental illnesses handled by traditional healers in Jinja and Iganga districts, Eastern Uganda. Methods and materials This study was carried out in two districts of Uganda, namely Jinja and Iganga, located in the Busoga region of Eastern Uganda. The population of two districts totals 1,234,248 (2002 national census). The setting: The shrine The setting of this study was the shrine, the place for the practice of traditional healers. The shrine is usually located within the community. The details of the study setting have been described in a previous preliminary study 15. Study Design This was a cross-sectional descriptive survey of patients who attend traditional healers' shrines. The Self Reporting Questionnaire (SRQ-25) was used as the screening instrument to consecutively screen patients for psychological distress. A psychiatric diagnostic instrument, the Mini International Neuropsychiatry Interview (MINI plus), was administered to make specific psychiatric diagnosis and the Global Assessment of Functioning was used to measure severity. Sample size calculation Sample size was calculated using the Kish Leslie formula for single proportions for descriptive study. The calculation assumed a frequency of 48 % for mental disorders at the traditional healer's facility 13. For a 95% confidence interval and a precision of 0.05, a total of 400 patients were consecutively screened and administered the MINI. Candidates were included if they were 18 years and above and did not have signs of life-threatening illness, e.g. convulsions, altered consciousness, coma etc. Patients who were not competent to give their consent and whose relatives declined to consent on their behalf were excluded from the study. Sampling of traditional healers All traditional healers who admitted to treating clients with mental health problems and could be reached in the two districts were included in the study. Iganga had 60 registered healers and Jinja had 180. For inclusion, the traditional healers also had to be registered with their organization and to have practiced in the district for more than six months. The number of patients per traditional healer per district was worked out proportionally. Measures The study instruments consisted of: a) A socio-demographic questionnaire This was a prepared socio-demographic questionnaire comprising age, gender, marital status, tribe, religious affiliation, educational attainment, number of children, employment and household monthly income. This information was obtained through completion of the questionnaire. Additional questions were included on the number of episodes, family history and type of help sought for the same symptoms. b) The Self Reporting Questionnaire (SRQ-25) This was used for screening patients. The SRQ-25 is a WHO research instrument developed to screen for mental disorders in the community. The SRQ-25 consists of SRQ-20, which was derived from four psychiatric morbid instruments from a wide variety of cultural backgrounds 16, plus five questions to screen for Psychotic disorders and Epilepsy. Further details are reported elsewhere 15. Although only 65% of the screened patients had psychological distress and were therefore eligible for administration of MINI (see below), the diagnostic instrument was administered to all screened patients. This is because over 80% of the screened patients answered `yes' to at least one of the four questions that screened for psychosis. c) The Mini International Neuropsychiatric Interview (MINI) The MINI is a short structured diagnostic interview for DSM-1V (Diagnostic and Statistical Manual Fourth Edition) and ICD10 (International Classification of Disease, Tenth Edition) for psychiatric disorders 17, 18. It covers 17 Axis 1 categories in a shortened format and is designed to meet the need for a short but accurate structured interview. It was developed to address the shortcomings of SCID-1 (Structured Clinical Interview for DSM-IV) and CIDI (Composite International Diagnostic Interview), with which it shows good correlations, and has higher reliability and validity scores than either of them 17, 19. In Uganda, the MINI has been translated and backtranslated in Luganda and repeatedly used 20. For the purposes of this study, the MINI was translated into Lusoga, the language of the study area, and back translated by an independent clinician from Busoga. d) The Global Assessment of Functioning (GAF) This instrument was used to measure the severity of mental illness. The GAF values range from 0 (most severe) to 100 (least severe), with 10 anchor points at equal intervals 21. Each interval of the GAF is accompanied by a behavioral descriptor, ranging from "superior functioning in a wide range of activities … no symptoms" to "persistent danger of severely hurting self or others … persistent inability to maintain minimal personal hygiene." The interviewer first determines the descriptor that summarizes the client's current difficulties, and then indicates the severity of impairment with a nine-point range 21. Functioning according to GAF was rated by trained research assistants on the basis of information gathered from the patients at the traditional healer's shrine. GAF assessments referred to the current symptoms. All the four assessors attended a one-hour session which provided a description of the scale and instruction on its use. The good interrater reliablity of the GAF when used by research assistants has been demonstrated in previous studies 21. In this study, interrater reliability between psychiatrists and the research assistants after training was satisfactory (Intraclass Correlation Coefficient between 60 and 83). For the purpose of this study, GAF was classified as follows, based on previous studies 22,23: GAF ≤ 70=Mild ; GAF ≤ 50=moderate ; GAF≤ 30 =severe. Data collection Psychiatric Clinical Assistants working in Jinja and Iganga districts collected data. They were guided by individuals who were acquainted with the area's traditional healers. District officials and the traditional healers were officially contacted before the data collection began to inform them about the purposes of the study and ask for permission. A standard set of procedures and statements was prepared for the interviewers to introduce themselves to the traditional healers. The traditional healers were asked for permission to talk to their clients or patients, while the clients/patients or their relatives were requested to consent to participate. In case of need for referrals or advice, the trained psychiatric clinical assistants gave the advice and referred the patient after agreeing with the healer in charge. Strategies used to decrease embarrassment included: empathetic tone, initial allaying of anxiety, and enquiring about significant areas of life. The research assistants were themselves clinically competent to make psychiatric diagnosis. They used their clinical competence to confirm the diagnosis of the MINI Plus. When in doubt; the first author, a psychiatrist, was called in to double check the clinical diagnosis. Ethical clearances were obtained from the necessary sources, including the Faculty of Medicine Higher Degree Research and Ethical Committee (HDREC); the National Council of Science and Technology (NCST), Leader of traditional healers, the Resident District Commissioners of the two districts, and the Research Committee Ethical Council, Karolinska Institutet (Permission number 05/07). Concerning consent from the mentally ill patient, the research assistants assessed the patient's capacity to understand the purpose, nature, risks, benefits, and alternatives of the research. If this was found to be lacking, relatives or guardians who had accompanied the patient were requested to consent on behalf of the patient. Data analysis Completed forms were checked for completeness, consistency and accuracy on a daily basis and before data entry into a computer. We used Epidata for data entry and the descriptive data analysis and calculation of frequencies were performed using SPSS version 15.0 for Windows. To explore the relationship between severity and the combined use of biomedical services and traditional healers, we used Pearson's chisquare tests and odds ratios. The level of statistical significance was set at 5% (i.e. P<0.05). Results Socio-demographic characteristics The numbers of males and females were nearly equal (46% and 54%, respectively); the patients mainly belonged to the Basoga tribe (86.6%) and a majority were Christians (61.6%). Three-quarters of the respondents (297, 76.7%) were below 45 years of age and the mean age was 34.8 years (S.D. 13.55). A majority (350, 90.4%) earned the equivalent of less than 1 dollar a day and 223 (57.6%) were not in gainful employment. Four-fifths had obtained some education (311, 80.9%; primary school 50.9%, secondary school 29.5%). There were nearly equal numbers of married and non married: 196 (50.6%) and 191 (49.4%), respectively. Prevalence and severity of mental illness Of the 387 respondents, 233 (60.2%) had at least one current diagnosed disorder. There were 63 (16.3%) who had experienced at least one disorder in their lifetime, while 170 (44%) had had two or more episodes. Psychosis was most frequent, occurring in 115 (29.7 %) of the sample. Table 1 presents the distribution of the patients' current mental illnesses. The rates of the other disorders (common mental disorders) were lower. The exploration of the relationship between GAF scores, number of episodes, combined use of traditional healing practices, and a positive family history reveal that patients with GAF scores in the moderate and severe range were more likely to have a family history of mental illness, to have had two or more episodes previously and to have sought help from traditional healers and biomedical services for the same problems as shown in table 3. Discussion Our findings showed the rates of current mental disorders at the traditional healers' shrines were higher for psychosis but lower for anxiety and depression. This differs from findings in other studies 13, 14. In those studies, traditional healers were considered to be a part of primary health care, thus offering general health care services 13, 14. In this study, healers were sampled who reported that they were managing mental health problems, hence a specialised group. This may explain our finding of 29.7% for psychosis and lower rates for common mental disorders compared to previous studies 13, 14. Moreover, we did not consider other physical or social problems which the traditional healer may have been treating. The literature contains few studies that specifically document the prevalence of mental disorders, including psychosis, among persons attending traditional healers. The prevalence of about 60% for current mental disorders in our study is similar to that reported by Saeed and others in a study on native faith healers in rural Pakistan 24. Neither did that study report on rates of psychosis. Our rate for current mental disorders is twice the level found in primary health care studies in Africa 4, 6. Our finding of a lifetime prevalence of 16.3% is almost four times higher than the rate of 4.7% in the WHO study in Yoruba, Nigeria 7. It appears self-evident that common mental disorders with mild symptoms are present in the community and it seems that individuals with such disorders tend to seek help only when the disorder becomes severe and that when they do so, they may first consult traditional healers or a primary health care setting that treats everything (general practitioners). When the patients become psychotic, they finally go to `specialists': traditional healers who treat psychosis. On the other hand, in the context of limited resources, only people with socially disruptive behavior are likely to attract the attention of family and community members and therefore seek help 25 26; people who are depressed and essentially bother nobody else but themselves tend to be overlooked 25,26. Regarding severity, most of the disorders in our sample were moderate to severe; just over 13% were mild cases. This finding could be explained by the suggestion that although mental disorders are common in the community, a large proportion of those with such disorders nevertheless manage to avoid considerable functional limitations 8, 27, 28. When they do become dysfunctional or disruptive, help is sought 26. Patients with GAF scores in the moderate to severe range were more likely to use both biomedical services and traditional healers for their symptoms. This could mean that when people have a moderate to severe functional impairment, they will tend to look for help wherever they can find it. Previous studies have shown that communal cultural concepts of mental illness are still prevalent 26. However, it seems that when it is a matter of desiring to get well, biomedical and traditional concepts are combined to fulfill this desire. Further research may be needed in the area of how concepts of health and illness determine the utilization of available services. When considering our findings, the following four limitations should be noted:
Conclusion and implications About 60% of the attendees of traditional healing practices in Jinja and Iganga had at least one diagnosable current mental illness and 16.3% had at least one disorder in their lifetime. The majority had moderate to severe symptoms. These findings represent a first step in documenting the burden that caring for patients with mental illness places on traditional healers, thus providing evidence of a need for biomedical practitioners to work together with traditional healers. Rather than competing with each another over delivery of mental health care, the scarce mental health professionals and traditional healers could try to complement each other and work together. They must learn to recognize the limits and boundaries of their respective professions and be aware of each other's strengths and weaknesses. Training for both groups in this regard may be necessary. Initial screening for more severe psychiatric disorders could optimally occur at the traditional healer's shrine and primary health care centres, to ensure early recognition and timely referral to psychiatric professionals. When diagnosis and treatment of such patients have been initiated by the mental health professionals, the traditional healers could assist in follow up by supporting the treatment plans and providing culturally sensitive counselling, careful monitoring of treatment compliance and observation of the patient for disease exacerbation/relapse. Psychiatrists in turn could educate the traditional healers about signs of the more severe psychiatric illnesses and assist them in recognizing them and referring appropriately. Furthermore, mental health professionals could provide guidelines to help the traditional healers determine when their clients with milder psychiatric conditions should be referred for more specialised treatment. Close collaboration among psychiatrists and traditional healers offers the best hope of meeting mental health care needs in a timely, coordinated, ethical and cost-efficient manner. Thus, the creation of a new health cadre, the traditional mental health Attendant (TMA) 31, would be a useful addition to primary mental health care in Africa, where there is an alarming scarcity of western-trained mental health professionals. Acknowledgements We thank the Swedish government for funding this project through Sida/SAREC, all the participants for taking part in this study and the traditional healers for allowing the Western-trained health workers access to their clients and their shrines. We are grateful to the research assistants for collecting data and to Patrick Hort for proof-reading. References:
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09025t3.jpg] [hs09025t2.jpg] [hs09025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}