 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 143-146 Screening for hepatitis C among HIV positive patients at Mulago Hospital in Uganda Walusansa V and *Kagimu M Makerere University College of Health Sciences, School of Medicine, Department of Internal Medicine,
Gastroenterology Division Code Number: hs09033 AbstractBackground: In industrialized countries with more resources, it is recommended that HIV infected patients should
be screened for hepatitis C virus (HCV) on entry into the health care system. Implementation of these guidelines in a
country like Uganda with limited resources requires some modification after taking into account the prevailing circumstances.
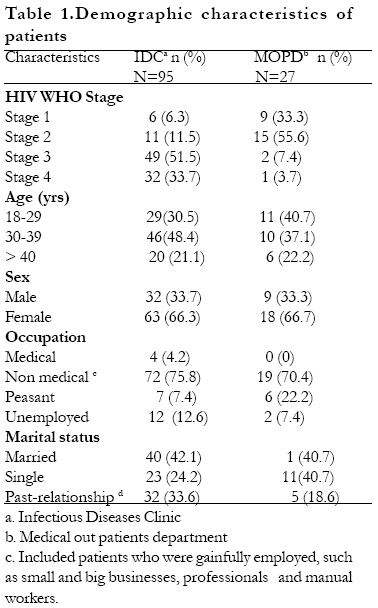
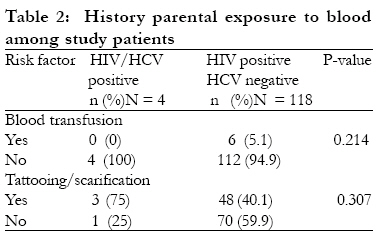
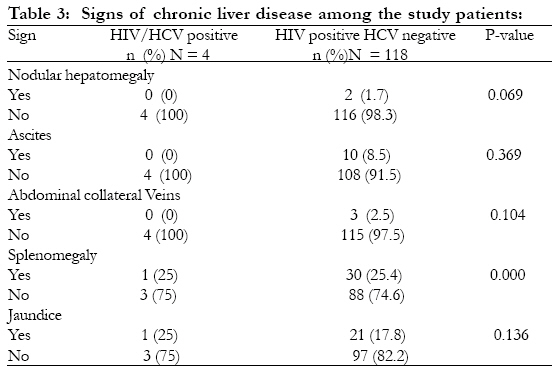
These include the prevalence of HCV in HIV positive patients and the cost of HCV testing. Introduction Human immunodeficiency virus (HIV) and Hepatitis C Virus (HCV) share routes of transmission. They both can be transmitted through exposure to contaminated blood, sexual intercourse and from mother to child. HCV is more transmissible through percutaneous blood exposure compared to HIV. In contrast HIV is more transmissible through sexual intercourse and from mother to child compared to HCV1. HIV infection has an impact on HCV infected patients and vice versa2. HCV is a hepatotrophic virus which causes liver cirrhosis in 20 30 years3. However, in HIV/HCV co-infected patients it is estimated that cirrhosis may occur in 6-10 years4. HIV patients with HCV have increased HAART-associated hepatotoxicity according to some studies5,6,7. In the United States with more available resources it is recommended that all HIV infected patients should be screened for HCV at entry into health care. The reasons given for this include the fact that many of their patients acquire HIV infection through intravenous drug use which is also associated with a high risk of HCV infection. In addition, knowledge of HCV status in the HIV positive patients on antiretroviral therapy may help in the interpretation of the causes of elevated liver enzymes. It is therefore, recommended that screening should begin with enzyme immuno assays (EIA) for antibodies to HCV. Positive anti-HCV samples should then be verified with recombinant immunoblot assays (RIBA) or reverse transcriptase polymerase chain reaction (RT-PCR) to assess HCV RNA8. Implementing these guidelines in a country like Uganda with limited resources can be challenging. There are various considerations that have to be taken into account before such recommendations are put into practice. One of these is the cost of the testing9. If the costs are very high then routine testing becomes difficult to apply. Another issue is the prevalence of HCV among HIV positive patients. If it is very low then routine HCV screening may not be cost effective. It is also important to know if there are risk factors and signs of chronic liver disease that are associated with HIV/HCV co-infection, which may identify patients for priority HCV screening. The frequency, with which HIV/HCV co-infection results in liver damage with elevated liver enzymes, is another important consideration. The study was done to assess the magnitude of some of these issues among HIV positive patients in Mulago hospital with a view of contributing to recommendations for HCV screening in a resource constrained environment. The objectives of the study were: to estimate the prevalence of HCV infection in HIV positive patients, to assess history of parenteral exposure to blood in patients with HIV/HCV co-infection, to determine the frequency of signs of chronic liver disease in patients with HIV/HCV co-infection, and to assess the frequency of elevated liver enzymes namely alanine transaminase(ALT) and aspartate transaminase (AST) among patients with HIV/HCV co-infection. In this study, elevated liver enzymes were defined as any values that were two or more times above the upper limit of the normal range. Methods The study was a descriptive cross sectional survey carried among HIV positive outpatients in Mulago hospital. These patients were recruited from the Infectious Disease Clinic and Mulago hospital Medical Outpatient Department. All consecutive patients above 18 years who consented to participate in the study and had serologically proven HIV infection, were recruited into the study. The patients from the Infectious Disease Clinic had with them medical records confirming their HIV sero-status. The patients from the Medical Outpatients Department were tested for HIV infection using the Abbot Determine Kit and the positive cases confirmed using Stat-Pak kit. A sample size of 124 was calculated using the Kish and Leslie's formula with an estimated HCV prevalence of 3% in sub-Saharan populations10,11. A questionnaire was administered to the patients to assess selected risk factors for HCV such as history of blood transfusion, tattooing, scarification and intravenous drug use. Physical examination was also done to assess features of chronic liver disease such as ascites, abdominal collateral veins and splenomegaly. Blood samples were taken from patients to assess anti-HCV and liver enzymes (AST and ALT). Samples for HCV serology were transported in dry ice to Roche laboratories in Mannheim Germany. Screening for anti-HCV was done using the Roche diagnostics GM BH assay. This is a rapid screening assay which has a sensitivity and specificity for anti-HCV similar to third generation recombinant immunoblot assay (RIBA III). The liver enzymes were assessed in the chemistry laboratory of Mulago hospital using an automated calorimetric machine.All the data was coded and entered in EPI-INFO version 6.02 computer soft ware package. Data analysis was done using SPSS version 10 software package. The study was approved by the Makerere University Faculty of Medicine Research and Ethics committee. Results Between October 2003 and February 2004, one hundred and twenty two HIV positive patients were recruited into the study. The baseline characteristics of the patients are shown in Table 1. The mean age of these patients was 33.9 years. The majority of the patients 81 (66.4%) were females. Only 4 of these patients had anti-HCV. Assuming all these patients had active infection, the prevalence rate of HCV among HIV positive patients was 3.3%. None of the patients with HIV/HCV co-infection gave a history of blood transfusion or intravenous drug use. Three of the patients gave a history of tattooing or scarification as shown in table 2. However, because of the small number of HIV/HCV co-infected patients statistically conclusive inferences could not be made. None of the HIV/HCV co-infected patients had physical signs of chronic liver disease such as ascites, abdominal collateral veins, palmar erythema, spider naevi, and nodular hepatomegaly. Only one HIV/HCV co-infected patient had splenomegaly and one patient had jaundice as shown in table 3. None of the HIV/HCV co-infected patients had elevated liver enzymes (ALT, AST). Discussion In this study, the prevalence of HCV among HIV positive patients in Mulago hospital was 3.3.%. This is quite low. It is similar to the HCV prevalence of 2.8% which was found among 102 HIV positive patients at the Joint Clinical Research Centre in Uganda in the year 200012. An earlier study in 1990 also found a low HCV prevalence of 2.5% among 160 Ugandan mothers13. Sixty percent of these mothers were HIV positive, but none of the HCV positive mothers had HIV infection. Another study among 603 sickle cell children in Mulago hospital found anti-HCV prevalence of 4%14. Other studies in the East Africa region show similar low prevalence rates. For example in Kenya, the prevalence of anti-HCV was found to be 0.1% among blood donors and 2.9 among patients with Hepatocellular carcinoma15 The prevalence of active hepatitis C infection could even be lower. This is because antibody tests for HCV detect a significant number of false positives due to cross reaction with other tropical infections such as malaria16. In addition, it is possible that some of the patients who were exposed to HCV cleared the infection and remained with only antibodies to HCV. It is estimated that 25 52% of symptomatic and 10 15% of asymptomatic HCV infections are spontaneously cleared17. In the study among sickle cell children only 11% of the anti-HCV positive children were confirmed to have viral RNA by reverse transcriptase PCR14. It was not possible to predict which of the HIV patients was more likely to have HCV infection by assessing history of parenteral exposure to blood. Assessment of physical signs of chronic liver disease as well as measurement of liver enzymes were also not helpful in this regard. The reason for this could be due to the small numbers in the study. Another reason could be that HCV is not commonly associated with advanced chronic liver disease among our HIV positive patients. However this is not easy to confirm because it has been observed that physical signs and serum transaminases are poor predictors of chronic liver disease in HCV infection. This is because they tend to manifest only in end-stage liver cirrhosis18.The costs for screening for HCV are considerable. In a study among blood donors in Uganda in 2000, the cost for one enzyme immuno-assay test was estimated to be US$ 5.19. The cost for anti-HCV screening per blood donation was estimated to be US$ 5.95. It was calculated that screening for HCV is 112 times more expensive than screening for hepatitis B virus9. In the case of screening patients for HCV it is important to confirm active infection by testing for viral RNA using reverse transcriptase PCR3. This will avoid informing patients that they have HCV infection when in fact their infection could have been cleared or the test could have been a mere false positive. This additional testing adds considerably to the screening costs for HCV. Our study is limited by the small samples size which restricts the generalizability of the results. However, a similar study in Kenya with a larger sample size, showed the HCV prevalence of 3.7% among 458 HIV positive patients19. In view of this low HCV prevalence found in our study and similar studies and considering the current high costs of the screening tests we conclude that routine HCV testing should not be recommended for all HIV positive patients in Mulago hospital and similar health care settings constrained by resources. Under these circumstances we recommend that HCV screening should be limited to investigating HIV positive patients with features suggestive of liver disease in order to identify HCV as a possible cause. Acknowledgment We are grateful to Dr. Namale Alice, Dr. Moses Kamya, Dr. M. Laderman, Dr. D. Zdunek, Ms. Lisa Gerwig, and Kulika Charitable Trust for their support in this study. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09033t2.jpg] [hs09033t3.jpg] [hs09033t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}