 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 153-160 Prevalence factors associated with Hypertension in Rukungiri District, Uganda - A Community-Based Study Wamala JF ¹, Karyabakabo Z2, Ndungutse D3, *Guwatudde D3 1. Epidemiology and Surveillance Division, Ministry of Health, Kampala, Uganda. Code Number: hs09035 Abstract Background: Hypertension is a growing public health problem in Uganda and Africa as a whole. We conducted a study
to determine the prevalence and identify factors associated withy hypertension among residents of the rural district
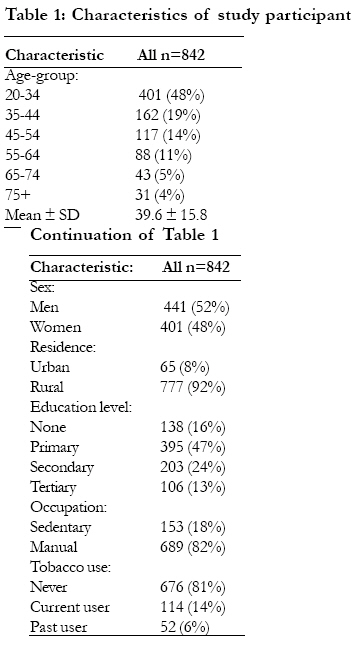
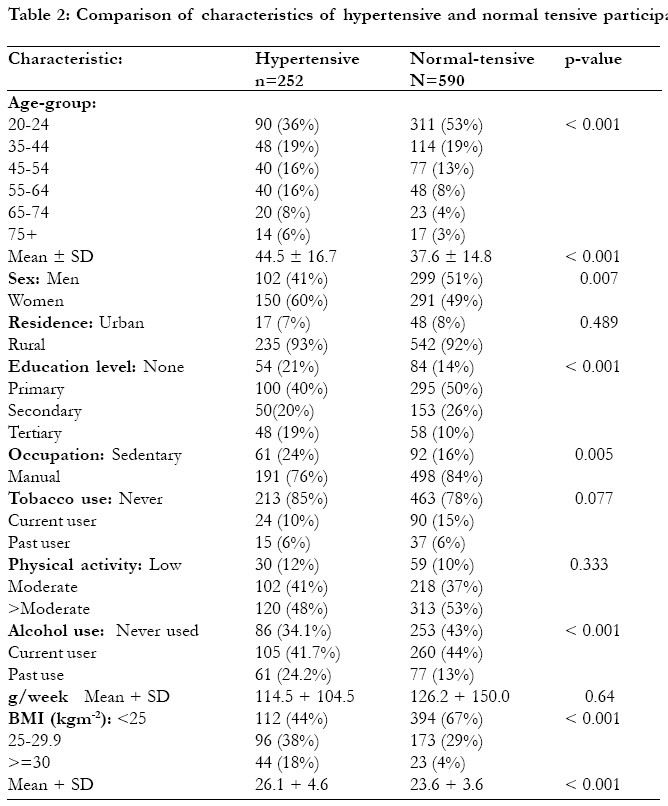
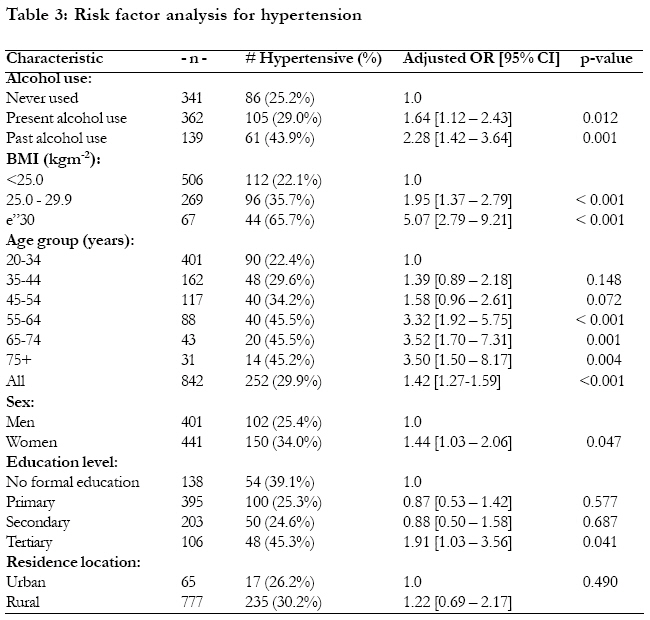
of Rukungiri, Uganda. Key words: Prevalence of Hypertension, Risk factors for hypertension, Community-based study, Rural Setting, Uganda. Introduction Hypertension is classified into primary hypertension, which accounts for the majority of adulthood hypertension with no identifiable cause, although there are usually recognisable risk factors; and secondary hypertension, which accounts for the majority of childhood hypertension1. Some of the known risk factors for primary hypertension like age, heredity, and gender are non-modifiable. However, the majority of the other risk factors like tobacco use, alcohol use, unhealthy diet, physical inactivity, overweight and obesity can be effectively prevented2. Hypertension is the most common cardiovascular disorder affecting approximately 1 billion people globally and accounts for approximately 7.1 million deaths annually3. Until recently, hypertension has been given low priority in Africa. The condition is now being widely reported in many parts of Africa and is the most common cause of cardiovascular disease on the continent3. Recent studies conducted in Africa have revealed prevalence ranging from 7.5% in Sudan (Elbagir and Ahmed 1990 cited in Addo et al 20074, to as high as 37.7% in Tanzania5. A literature search on the prevalence and/ or determinants of hypertension in Uganda reveal no recent publications on this problem in the past few decades. Published community-based studies to estimate the prevalence of hypertension in Uganda were conducted before the 1960s. The first was conducted in the then Teso District in 1941, which showed a prevalence of hypertension of 2.9% among adults aged 21-50 years6. Another population-based survey was conducted in the early 1960s in Kasangati, a rural community outside of Kampala city, which revealed prevalence of hypertension of 13.7% among persons aged 10 years or older7. There is therefore scanty literature on the estimated burden, and the determinants of hypertension in the Ugandan population. Anecdotal data however suggests that hypertension has increased over the years, and is increasingly becoming a public health problem. A recent study conducted among Makerere University students showed prevalence of systolic blood pressure of 11% and diastolic blood pressure of 18%8. An exploratory study conducted in 2005 among adults attending outpatient clinics in Rukungiri District in Uganda revealed a hypertension prevalence of 23.7% [Wamala et al., 2005, un-published report]. Prompted by this relatively high prevalence of hypertension among outpatients, combined with the fact that currently there is limited information on the prevalence and determinants of hypertension in Uganda, we conducted a community-based study to determine the prevalence, and identify factors associated with hypertension in this rural Ugandan district. MethodsSetting and Sample Selection Rukungiri District is a rural district located in South Western Uganda, approximately 400km west of Kampala, the capital city of Uganda. According to the 2001 Uganda population census, the district has a total population of approximately 287,544 people9. The district has one main township, Rukungiri town, and the inner part of the district portrays characteristics of a typical Ugandan rural community with limited telephone service, electricity or tap water, and is mostly accessible via dirt roads. Between January and February 2006, a sample of residents in the district was enrolled in this study. Study participants were selected using a two-stage sampling procedure. First, 19 villages were randomly selected from the 11 sub-counties in the district. The calculated sample size was allocated to the 19 villages in proportion to the estimated population size in the villages according to the 2001 Uganda population census9. Our study is the only community-based study conducted in recent years in Uganda to estimate the burden, and identify the determinants of hypertension in the general population. A household was defined as a group of individuals living within one domicile, who normally shared meals together. Only one consenting adult household member aged 20 years or older within each of the sampled households was included into the study. Further, only subjects who had resided within the district for at least one year prior to the date of identification of the household by the research team were eligible for inclusion into the study. The conduct of this study was approved by the Makerere University School of Public Health's Higher Degrees, Research and Ethics Committee. Measurements A cross-sectional study design was used to conduct this study. Trained research assistants performed the physical measurements and administered a standardized questionnaire. The questionnaire collected data on demographics, social economic and exposure history to various potential risk factors for hypertension for the period of up to 10 years prior to the date of interview. Blood pressure, weight and height of participants were also recorded. Hypertension was defined as systolic blood pressure (BP) 140mmHg and/or diastolic BP 90mmHg, or being on regular anti-hypertensive therapy. Potential risk factors for hypertension were classified into two categories, modifiable and non-modifiable. The modifiable potential risk factors measured included: amount of salt use in diet; history of alcohol use; tobacco use; fruit and vegetable consumption; physical activity; weight, use of hormonal contraceptives, occupation, highest level of formal education attained, and location of residence urban or rural as defined by the Uganda Bureau of Statistics9 ; that is, participants residing in Rukungiri township were classified as urban and rest as rural. The non-modifiable potential risk factors assessed included: height, age, history of diabetes mellitus, history of renal disease, and first degree family history of hypertension. Height was measured without shoes using roller type, Seca 208 body meter to the nearest 0.5cm. Weight was measured to the nearest 0.5kg with a manual round-dial flat, SecaÔ weighing scale, with the participants in light clothing and without footwear. Body mass index (BMI) was calculated as weight (kg) divided by squared height (m²)3. Blood pressure (BP) and pulse rate were measured after the participant had been sitting upright for at least 5 minutes with an automatic machine (Speidel+Keller). The medium adult cuff for arm circumference 22 to 32cm was used. Three blood pressure readings were taken 1 minute apart. The average of the last 2 readings was used in the analysis10. Statistical Analysis Prevalence of hypertension was calculated as the percentage of participants classified as hypertensive, with all study participants as the denominator. Prevalence was standardized by age using the method suggested by Morris and Gardner11. Thus the age-standardised hypertension prevalence was calculated by directly standardising to the New-world population aged 20 years or older. Binary logistic regression analysis was used to identify potential risk factors associated with hypertension. Only potential risk factor variables with a p-value of less than 0.05 were retained in the final logistic regression model. For this analysis, Odds Ratios (OR) with their corresponding 95% confidence intervals (95% CI) are reported. All statistical analyses were performed using the Statistical Package for Social Sciences Version 10.0.112. Results Characteristics of study population A total of 842 residents of Rukungiri District participated in this study, of which 441 (52%) were females. The average age of participants was 39.6 (SD=15.8) years, and 48% were aged 20-34 years. Only 37% of the participants reported to had attained secondary school education, or higher. Only 65 participants (8%) were enrolled from Rukungiri Township, therefore were classified as "urban" residents. Most of the participants, 689 (or 82%) reported to be engaged in manual type of work as their main occupation. Of all the participants, 503 (60%) reported to have ever used alcohol, and 365 of these were current users Only 166 (20%) of the participants reported to have ever used tobacco, and 114 of these were current users. Forty percent of the participants (336) had a BMI of 25 or higher. Table 1 provides a summary of the characteristics of the study participants. Prevalence of hypertension A total of 252 study participants were classified as being hypertensive, giving a crude prevalence of hypertension of 30.4%, with a 95% Confidence Interval (CI) of 26.1 - 34.6%. Among hypertensive participants, the average systolic blood pressure reading was 144.0 (SD=17.4) and the average diastolic blood pressure reading was 90.4 (SD=9.7); whereas the normal-tensive participants, the average systolic blood pressure reading was 120.1 (SD=12.5) and the average diastolic blood pressure reading was 76.2 (SD=8.6). The age-standardised prevalence of hypertension was 30.5% [26.6 - 34.3%]. There was no significant difference in the age-standardised prevalence of hypertension between urban and rural dwellers (p-value =0.489). Hypertension prevalence was significantly higher among females, 34.0% [29.6% - 38.4%] compared to males 25.4% [21.1% - 29.7%]; (p-value =0.007). The majority of participants with hypertension (55%) were aged between 20 to 44 years (see Table 2). Participants with hypertension were significantly older with an average age of 44.5 (SD=15.8), compared to normal tensive participants with an average age of 37.6 (SD=14.8); (p-value < 0.001). Participants with hypertension also on average had greater BMI (average of 26.1 + 4.6), compared to those without hypertension (average of 23.6 + 3.6), p-value <0.001. Factors associated with hypertension Of the modifiable factors measured in this study, three were found to be significantly associated with hypertension, that is alcohol use, level of education, and Body Mass Index (BMI). Current alcohol users were more likely to be hypertensive compared to participants reporting to have never used alcohol, with an adjusted Odds Ratio (OR) of 1.64, [95% CI= 1.12 2.43]. Past alcohol users were also more likely to be hypertensive compared to participants reporting to have never used alcohol with an adjusted OR=2.28 [1.42 3.64]. Participants reporting to had attained tertiary level of education were more likely to be hypertensive, compared to those reporting to have never received any formal education with an adjusted OR= 1.91 [1.03 3.56]. Having a BMI greater than 25 was significantly associated with hypertension, the association being highest in subjects with BMI of 30 or higher, with an adjusted OR of 5.07 [95% CI= 2.79 9.21], compared to subjected with BMI less than 25 (see Table 3). The non-modifiable factors measured in this study that were found to be associated with hypertension included age and sex of the participant. The likelihood of hypertension increased with advancing age, with a significant association to hypertension starting from the age group 55-64. Among subjects aged 55-64 years, the adjusted OR was 3.32 [1.92 5.75], whereas the adjusted OR in subjects aged 65-75 was 3.52 [1.70 7.31], and in subjects aged 75 years or older the adjusted OR= 3.50 [1.50 8.17], all compared to subjects aged 20-34 years. Female participants were more likely to be hypertensive compared to men, with an adjusted OR=1.44 [1.03 2.06]. Discussion Our study has determined that approximately one in every three adults aged 20 years or older in the rural Ugandan district of Rukungiri is hypertensive. The age-standardised hypertension prevalence was found to be 30.5%, which is much higher than that found in the few community-based published studies previously conducted in Uganda. It should be noted that comparison with previous surveys is problematic since previous studies used diverse definitions of hypertension and varying phases of recording the diastolic BP. Despite the differences in measurement of hypertension however, hypertension prevalence in Uganda appears to have increased over the years. A blood pressure survey by Williams (1941) in the then Teso District of Uganda showed that 2.9% of adults aged 21-50 years had diastolic BP (4th korotkoff phase) just over 90mmHg6. Another hypertension prevalence study conducted among Baganda men and women aged 10 years or older residing in Kasangati, Uganda in the 1960s found a hypertension (160/95mmHg- 4th phase diastolic BP recording) prevalence of 13.7%7. The prevalence of hypertension in this rural district is also relatively much higher than what has been found in recent studies conducted in other parts of Africa. A recent review of published studies on hypertension in Africa by Addo et al showed prevalence of hypertension ranging from 7.5% in Sudan (Elbagir and Ahmed 1990 cited in Addo et al 20074 ) to 29.5% in Ghana13. Only one recent community-based study conducted in Tanzania has reported prevalence higher than that in our study of 37.7%5. Our findings therefore confirm the growing concern of hypertension as a public health problem in Uganda. We found three modifiable risk factors to be associated with hypertension, including alcohol use, level of education and weight. It should be noted that the three modifiable factors of tertiary education, alcohol use and being overweight or obese were identified in the World Health Report of 1997 as risk factors for hypertension2. Current alcohol users were approximately 1.6 times more likely to be hypertensive, while past alcohol users were 2.3 more likely to be hypertensive; all compared to those who had never used alcohol. Several studies have reported alcohol use to be a risk factor for hypertension. Here in Africa, Agyemang (2006), Aubert (1998) and the first demographic study in South Africa, among others have demonstrated an association between alcohol use (moderate to heavy consumption) and hypertension13-15. The magnitude of the risk imposed by alcohol use found in our study also closely compares with that found by Jo et al who have reported that adults aged 18 to 92 years in Korea who were present alcohol users were 1.3 times more likely to be hypertensive compared to those who had never used alcohol16. Participants reporting to had attained tertiary education were nearly 3 times more likely to be hypertensive compared to those reporting to have never gone to school. This finding is consistent with findings by Ordunez et al (2005), whose study revealed that Cuban men with a lower level of education had a 14% lower risk of hypertension compared with those above the median17. In Jamaica, Mendez et al (2003) found that blood pressure was positively associated some high school education among men18. In the developed world, studies have consistently revealed an inverse education-blood pressure association. In a multi-country study by Stamler (1992), found that age-adjusted systolic blood pressure was 1.3mmHg higher (p-value = 0.05) for men and 4.5mmHg (p-value < 0.001) for women with 10 fewer years of education. The less educated were found to have higher sodium excretion, greater body mass, and a higher alcohol intake leading to increased blood pressure19. Our findings are also similar to those from a study conducted in an urban population in early epidemiological transition in Tanzania where Bovet et al (2002), reported that non- educated men were more likely to have higher systolic blood pressure than those with primary education (p< 0.01) 20. Participants with a BMI greater than 25 were more likely to be hypertensive compared to those with a BMI of 25 or lower. In Tanzania, Bovet et al (2002) found that body mass index was strongly and independently associated with systolic and diastolic blood pressure (1.01 mmHg systolic BP per 1 kg/m2 increase in BMI) 20. In Nigeria, Agyemang (2006) has also reported an independent association between BMI and BP13. Similar results were reported by Önal et al (2004) who found that hypertensive adults aged 25 years or older were twice more likely to be overweight or obese in Istanbul, Turkey21. These findings imply that having a normal weight, or losing weight among those who are overweight or obese, would reduce the chances of developing hypertension. BMI is greatly influenced by dietary practices like high intake of saturated fatty acids, irregular fish consumption, tobacco use and low physical activity3. However in our study all these factors were not significantly associated with hypertension. Perhaps the risk imposed by these is all reflected in the BMI of the individual. Two non-modifiable risk factors were found to be associated with hypertension, including age and sex. Adults aged 55 years or older were more likely to be hypertensive compared to those in the younger age groups. This is consistent with findings from several studies that have reported the risk of hypertension increasing with advancing age. Edwards et al (2000) found that hypertensive men and women in rural and urban areas in Tanzania tended to be significantly older compared to those who were not hypertensive5. Another study conducted among adults aged at least 20 years in Soussa, Tunisia found that hypertension was significantly higher for adults older than 40 years of age22,23. Advancing age increases the risk of exposure to the lifestyle risk factors for hypertension and hence the observed increase in hypertensive risk with aging. In the present study, the female participants were nearly 1.5 times more likely to be hypertensive compared to male participants. Similar findings have been reported by Amoah (2003), who found higher age-adjusted hypertension prevalence in females (29.5%) compared to males (27.6%) in a study done among adults aged 25 years or older in Accra, Ghana24. Although it has been observed that many people in Uganda have tended to adopt "western-type" diet and sedentatry life styles that facilitate fat accumulation in blood predisposing them to Cardio-Vascular Diseases25, having sedentary (non-manual) occupation was not associated with hypertension in this study. Also location of residence (urban or rural) was not significantly associated with hypertension. Studies conducted in developing countries have revealed a higher risk of developing hypertension in upper socio-economic groups (good education, and sedentary occupations). Generally this corresponds to emerging middle-class populations and it probably represents the initial stage of the epidemic of cardiovascular diseases2. Conclusion Our study is the only community-based study conducted in recent years in Uganda to estimate the burden, identify the determinants of hypertension in the general population. The prevalence of hypertension in this rural Ugandan district is relatively high. Our findings confirm the growing public health challenge of Non Communicable Diseases (NCD) like hypertension as a public health problem in Uganda. However more community-based studies of this nature are required to determine the extent of this problem, and the risk factors for hypertension in other communities in Uganda. Interventions aiming at reducing the risk factors identified in this study are needed, and should target both the high risk and the overall population in order reduce the risk and prevalence of hypertension Study limitations Because we used a cross-sectional study design to identify factors associated with hypertension, and due to the long latent period between exposure to risk and the development of hypertension, it may be difficult for the study participants to remember exposures that preceded the disease from those that occurred after the disease had developed. Further, prevalent cases of hypertension may not be representative of all cases as some severe cases may die soon after developing the disease. We however we believe that the methods used in the conduct of this study enabled us minimize the possible effect of these limitations on the findings in this study. Acknowledgements We are grateful for the guidance, support and courteous help offered by the staff of Albert Cook Medical Library, the School of Public Health, and the Faculty of Medicine, all of Makerere University; and the Uganda Government Analytical Laboratories. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09035t3.jpg] [hs09035t1.jpg] [hs09035t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}