 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 161-166 A Comparison of two measures of quality of life of Nigerian clinic patients with type 2 Diabetes Mellitus 1Kolawole BA*, Mosaku SK2, R.T. Ikem1 1. Medicine Department, Obafemi Awolowo University, Ile-Ife, Nigeria Code Number: hs09036 Abstract Background: We present data comparing the quality of life effects of type 2 diabetes determined by the Bradley
well-being questionnaire and the WHOQOL-BREF, a generic instrument. We also present data on the reliability and validity of
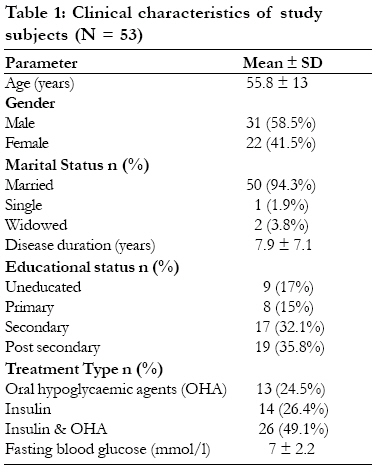
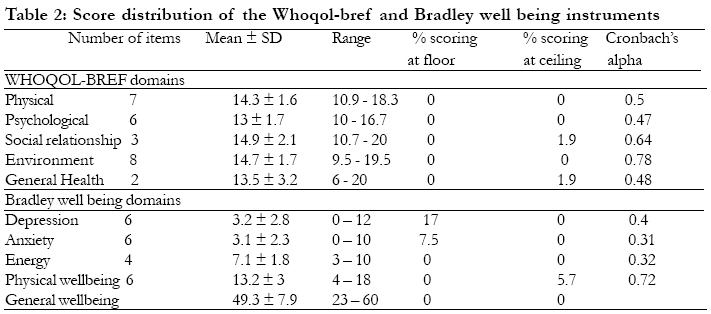
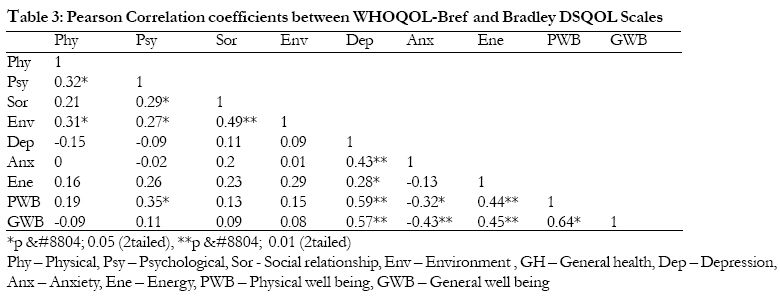
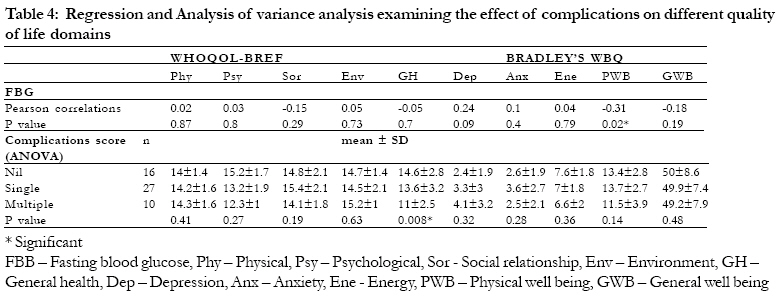
these instruments. Keywords: Comparison, Type 2 diabetes, quality of life, scales Introduction The incidence and prevalence of diabetes mellitus, once considered a rare medical condition in Africa is now increasing in most of these populations.1 Majority of patients also present with type 2 diabetes.2 Because of increasing life expectancy, an aging population and rapid urbanization, it has been predicted that by the year 2025, the majority of the world diabetes population will be living in the developing countries.3 Type 2 diabetes and its associated long term complications will therefore continue to impact individual and general health in these communities. Over the past two decades, health care research has shifted towards effectiveness research, i.e., studies that measure the multidimensional nature of health and health outcomes in naturalistic care settings.4 The focus of these studies include physical health, quality of life and functional ability as outcome measures. Quality of life and glycaemic control are now recognised as independent and achievable outcomes in diabetes management.5 The instruments and techniques used to assess quality of life vary according to the identity of the respondents, the setting of the evaluation and the type of questionnaire used. Generic instruments are used in general populations to assess a wide range of domains applicable to a variety of states, conditions and diseases.6 They are usually not specific to any particular disease state. Disease specific instruments on the other hand focus on domains most relevant to the disease or condition under investigation and on the characteristics of patients in whom the condition is most prevalent.7 We had previously validated the Bradley diabetes specific Well-being questionnaire8 among Nigerian type 2 diabetics.9 We found it to be a reliable instrument for measuring diabetes specific quality of life although it was originally designed and developed among a UK population. This was perhaps the first use of the Bradley questionnaires among indigenous Nigerians. There is no existing local literature comparing the quality of life findings in diabetic patients using both disease-specific and generic instruments. In an attempt to bridge this gap, and also expand our earlier study, we present data comparing quality of life effects of type 2 diabetes using the Bradley well-being questionnaire and the WHOQOL-BREF 10- a generic instrument. This kind of comparison increases our understanding of the psychometric properties and clinical utility of these alternative approaches to quality of life assessment among diabetic patients.11 Materials and MethodsPatients Fifty-three consecutive type 2 diabetics attending the Diabetes/Endocrinology clinic of the Obafemi Awolowo University Teaching Hospital, Ile-Ife, South-western Nigeria were recruited after obtaining their informed consent. Patients were not excluded on the basis of diabetic complications but newly diagnosed and newly presenting patients were excluded from the study. At recruitment, the Well-being Questionnaire (WBQ)8 and the WHOQOL-BREF 10 were self-administered by literate patients while the interview-administered mode was conducted by one of the authors (SKM) in illiterate patients using the Yoruba language translated version.9 Patients' demographic data, mode of treatment and educational status were also recorded. Glycaemic control was determined by calculating the mean blood sugar levels (both fasting and 2 h post-prandial) over the previous three clinic visits. The glycated haemoglobin (HBA1c) test usually preferred for the assessment of long-term glycaemic control was not available to us. Well-being and WHOQOL-BREF Scales The Well-being Questionnaire consists of 22 items scored on a 03 Likert scale, from which are calculated subscale scores for depression, anxiety, energy, and positive well being. A higher value on the scale indicates more of the mood described on the scale description. A general well-being score was calculated by reversing the scores of negative items, summing the subscale scores and adjusting to achieve a scale maximum of 66 (General well-being = 36 - depression - anxiety + positive well-being + energy). The WHOQOL-Bref instrument comprises 26 items, which measure the following broad domains: physical health, psychological health, social relationships, and environment. It assesses individual's perceptions in the context of their culture and value systems, and their personal goals, standards and concerns. Ohaeri et al12 had previously compared the WHO 4-domain and 6-domain models of the WHOQOL-Bref with the 8-domain model obtained from factor analysis (FA). Data from 118 recently recovered Nigerian psychotic patients were used in confirmatory factor analysis (CFA) to assess goodness of fit and clarity of concept. Their FA model had superior goodness of fit for CFA and provided clarity of concept. Complications Diabetic complications were identified from a review of patient medical records by BAK and RTI who were unaware of patient responses to the questionnaires. For all patients we noted the presence of all current diabetes-related complications as well as other current medical conditions found in the record. We then categorised complication severity based on the presence of none, single or multiple complications, e.g. symptomatic neuropathy, diabetic nephropathy and retinopathy. Statistical Analysis Data was analysed on computer using the SPSS statistical software. Computation was done in the following aspects: (1) Descriptive statistics, (2) The internal consistency of the quality of life scales was assessed using Cronbach's alpha, (3) Convergent and discriminant validity, (4) Known groups validity - Using regression analysis, we determined the relationship of fasting blood glucose and quality of life. We also determined the effects of diabetic complications on quality of life using analysis of variance. P values less than 0.05 are regarded as significant. ResultsCharacteristics of study patients Our patients had a mean age of 55.8 ± 13years. 31 (58.5%) were males. Most of them were in a marriage relationship 50(94.3%) and had at least primary school education (82.9%). 26 (49.7%) patients were being treated with a combination of oral hypoglycaemic agents and insulin while the others received either tablets or insulin. They had a mean blood glucose of 7 ± 2.2 mmol/l. Other descriptive statistics for the WHOQOL-BREF and Bradley's WBQ The score distribution of the WHOQOL-BREF and Bradley's WBQ are summarised in table 2. All the WHOQOL-BREF domains exhibited minor or no (in most cases) floor or ceiling effects. None of the domains exhibited the full range of score distribution. The depression and anxiety subscales of the Bradley's WBQ exhibited flooring effects (17% and 7% respectively) while ceiling effects were observed only for the positive well-being subscale (5.7%) Reliability of the Well being questionnaire and WHOQOL-BREF We computed the reliability coefficients (Cronbach's alpha) for the subscales of both quality of life measures. The alpha coefficients ranged from 0.31-0.72 for the Bradley's WBQ subscales and from 0.47-0.78 on the WHOQOL-BREF scale. Only the Environment domain of the WHOQOL-BREF and the Positive well being domain of the Bradley's WBQ had Cronbach's alpha values above 0.70. Table 3 presents correlations for the inter domain/scale scores of the WHOQOL-BREF and the Bradley's WBQ. The range of correlations for the inter-domain/scale of the WHOQOL-BREF was 0.21 0.49 (all p < 0.05 except for the association between the Physical and Social relationship domains). It showed a positive association among domains. Higher associations were observed among the domains of the Bradley's WBQ (range = -0.13 0.64). The association between the anxiety and others apart from depression were negative. All interscale correlations were significant except the relationship between anxiety and energy. Correlations between the scales of the WHOQOL-BREF and the Bradley's WBQ are also shown in table 3. Most domains showed weak relationships. The highest significant association was between the psychological domain of the WHOQOL-BREF and the positive well-being domain of the Bradley's WBQ. This may imply that they measure a similar concept. Negative associations were found between the physical domain of the WHOQOL-BREF and the depression and general well-being scales of the Bradley's WBQ as well as between the psychological domain/scale (WHOQOL-BREF) and the depression and anxiety domain/scales of the Bradley's WBQ. Weak associations were observed between the physical, social relationship and environment domain/scale of the WHOQOL-BREF and all the domains of the Bradley's WBQ (r range = -0.15 0.29). Influence of demographic factors on QOL In general, the quality of life measures were not influenced by characteristics such as gender, educational status or marital status. Age correlated negatively with the WBQ indices except depression but this did not reach statistical significance. Age also correlated negatively with the WHOQOL-BREF indices except physical functioning. This also did not reach statistical significance. Known groups validity/Diabetes complications and quality of life indices Table 4 shows that fasting blood glucose levels correlated negatively with the social relationship and general health domain/scale scores of the WHOQOL-BREF as well as the positive well-being scale of the Bradleys WBQ (p = 0.02). All other scales had very weak positive association with fasting bllod glucose. The scores on all domains/scales of the WHOQOL-BREF and Bradley's WBQ were however similar regardless of the number of complications except the general well-being scale of the WHOQOL-BREF for which patients with multiple complications scored significantly lower (p = 0.008 ANOVA) Discussion In the present study, we compared the quality of life indices determined using a disease specific and generic instrument in Nigerians with type 2 diabetes. The Cronbach's alpha values were significant (greater than 0.7) only for the Environment and Positive well-being domains of the WHOQOL-Bref and Bradley's WBQ respectively. This contrasts with findings from previous reports from use of the questionnaire among indigenous Nigerians.9,12 Mean domain/scale scores were however comparable with previously documented data.5,9,12 Noteworthy flooring or ceiling effects were not observed for any of the domains of the WHOQOL-Bref and Bradley's WBQ instruments. Correlations between the scores of physical and psychological domains of the WHOQOL-Bref and the anxiety and depression subscales of the WBQ were negative, though this did not reach statistical significance. The content of the physical domain in particular include facets such as activities of daily living, dependence on medications, and pain/discomfort while the psychological domain centres around body image, negative and positive feelings, self esteem among others. In contrast, the anxiety/depression domains measure negative feelings alone. These two domains of the WBQ were actually later merged to form a single negative well-being scale known as the WBQ 12.13 It therefore appears as if these set of domains measure different concepts. Interestingly, Aigner et al14 demonstrated an overlap between the concepts of well being/treatment satisfaction and depression. This is because of the negative influence of the depressed mood on the perception of oneself and the environment and because of the measurement overlap between quality of life instruments and psychopathological depression rating scales.15,16 It was therefore suggested that the WHOQOL_Bref should only be used in conjunction with an assessment of depressive symptomatology and to check for "contamination" of the quality of life measure by depressive symptom before drawing conclusions about QOL in such patients. We have not been able to reproduce these observations. In general, the quality of life measures we tested were not influenced significantly by socio-demographic parameters such as age, gender, education or marital status. We also did not find significant association between socio-demographic characteristics and quality of life indices in our previous use of the Well-being questionnaire.9 This is very similar to the experience of Ohaeri et al17 with the WHOQOL-BREF scales amongst Nigerians with a psychiatric diagnosis. One US study had explored the relationship between marital relationship domains, glycaemic control and psychosocial adaptation to diabetes18. Better marital satisfaction was related to higher levels of diabetes related `satisfaction and general quality of life. In spite of the fact that scientific evidence is still lacking, it appears that coping mechanisms such as the extended family system, spirituality and overall psychosocial functioning may be higher in the Nigerian population than among Caucasians. This may explain in part, the apparent lack of a significant relationship between quality of life indices and socio-demographic characteristics in this study. The influence of diabetes complications on quality of life is variable. Jacobson et al11 found that the Diabetes Quality of Life Measure (DQOL) scales were consistently sensitive to severity of complications and less consistently responding to number of complications. Generally speaking however, diabetic complications tend to negatively influence quality of life.15-17 Diabetic complications did not significantly influence quality of life in this study. Perhaps a different approach, i.e. relating quality of life to complication severity may have yielded a different outcome. One obvious limitation to our study is the small population studied. Though we have a fairly substantial pool of type 2 diabetic patients, data was obtained from only from those who were willing and able to participate. A second limitation was that we studied only outpatients. A reasonable number of inpatients were excluded because of the severity of their illness and we may not have obtained reliable responses. Our use of a cross-sectional design could be a limitation in a way because the responsiveness of these two quality of life instruments to change in patients' clinical status was not determined. Our study has shown how two different measures of quality of life perform in patients with type 2 diabetes. Even though the subscales of the Well-being and WHOQOL-BREF were not very sensitive to external criteria of disease impact (complications) casting a doubt on their utility as psychological outcome measures, they demonstrated fairly reasonable internal consistency in our patients with type 2 diabetes. Further larger studies are thus required to clarify this given our present limitations. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09036t4.jpg] [hs09036t3.jpg] [hs09036t1.jpg] [hs09036t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}