 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 170-173 Pattern and outcome of childhood intestinal obstruction at a Tertiary Hospital in Nigeria *Ogundoyin OO, Afolabi AO, Ogunlana DI, Lawal TA, Yifieyeh AC Department of Surgery, College of Medicine, University College Hospital, Ibadan, Nigeria Code Number: hs09038 Abstract Background: Intestinal obstruction is a common cause of pediatric surgical emergency with a high morbidity and
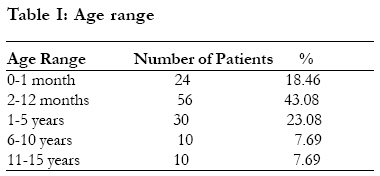
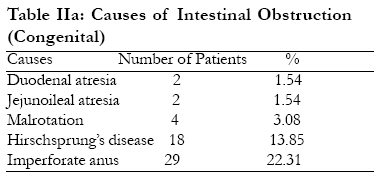
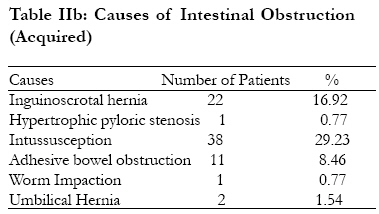
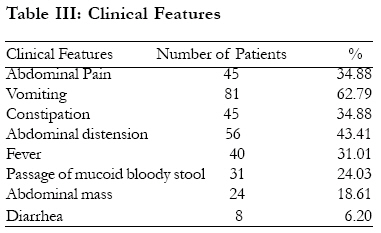
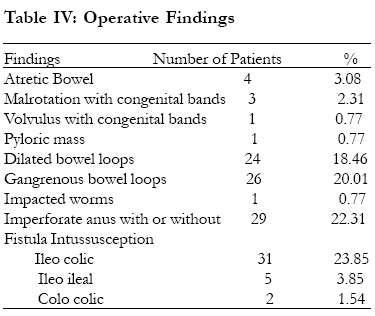
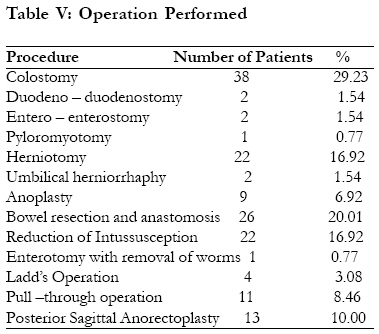
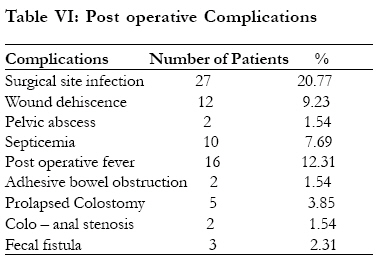
mortality in Africa. Key words: Childhood intestinal obstruction, Pattern, Management outcome. Running title: Pattern and management of childhood intestinal obstruction African Health Sciences 2009; 9(3): Introduction Intestinal obstruction is a common cause of pediatric surgical emergency in Africa1 3 . The pattern and causes of intestinal obstruction among different age groups in children in this country is different from what is seen in Europe and North America1, 3 5 . The clinical presentation is still similar to previous reports from this country but the attendant morbidity and mortality is still very high in this environment2. The aim of this study was to examine the pattern of the various causes of intestinal obstruction in children and the management outcome. Patients and Methods This was a 10-year retrospective review of all children aged 15 years and below, managed for intestinal obstruction between January, 1996 and December, 2005 at the Pediatric Surgical Division of University College Hospital, Ibadan, Nigeria. Data extracted from their case notes and analyzed included the patient's age, sex, causes of intestinal obstruction, symptoms and signs, management outcome and post operative complications. The cases of paralytic ileus were excluded from this study. Results A total of 213 children were managed in our center for intestinal obstruction. Out of these, 130 case notes were available for review from the hospital records department. The ages of these patients ranged from 2 hours (after birth) to 14 years with a mean of 1.96 years. Eighty patients (61.54%) were under the age of one year. Twenty four (18.46%) of the patients were neonates as indicated in Table I. There were 85 boys (65.39%) and 45 girls (34.62%); M: F = 1.9:1. Congenital causes accounted for 55 cases (42.31%) while 75 cases (57.69%) were due to acquired causes as shown in Tables IIa and IIb. Of the congenital causes, anorectal malformations and Hirschsprung's disease were the most common causes accounting for 22.31% and 13.85% respectively. Intussusception and obstructed inguinoscrotal hernia were responsible in 38 patients (29.23%) and 22 patients (16.92%) respectively in the acquired group. Of the 38 patients with intussusceptions, 64.7% of them presented between the ages of four and six months and majority were ileo colic. Other causes were adhesive intestinal obstruction 11 patients (8.46%), external umbilical hernia 2 patients (1.54%), worm impaction and hypertrophic pyloric stenosis 1 patient (0.77%). Table III shows the clinical presentation of children with intestinal obstruction. The classical presentation of vomiting, abdominal pain (excessive cry), constipation constipation and abdominal distension were observed in 81 patients (62.79%). Other presentations observed were fever in 40 patients (30.77%), passage of bloody mucoid stool in 31 patients (23.85%), diarrhoea and abdominal mass in 8 patients (6.15%), and 24 patients (18.61%) respectively. Operative findings were consistent with the various causes of intestinal obstruction as shown in Table IV. Of note were the findings of dilated loops of bowel in 24 patients (18.6%) and gangrene of the bowel in 26 patients (20.01%). Other findings included ileo colic, ileo ileal and colo colic intussusceptions in 31 patients (23.85%), 5 patients (3.85%) and 2 patients (1.54%) respectively, Imperforate anus with or without fistula in 29 patients (22.31%), atretic small bowel in 4 patients (3.08%), pyloric mass 1 patient (0.77%) and 1 patient (0.77%) with impacted worms one hundred and eighty seven in number. Of the 26 patients (20.01%) with gangrene of the bowel, intussusception was responsible in 16 patients (12.31%), inguinoscrotal hernia in 7 patients (5.39%), post-operative bowel adhesion in 2 patients (1.54%) and mid gut volvulus in 1 patient (0.77%). A total of 38 patients (29.23%) had an initial colostomy to relieve the obstruction, bowel resection and anastomosis was carried out in 26 patients (20.01%), herniotomy and reduction of intussusception was carried out in 22 patients (16.92%) each. Other procedures included posterior sagittal anorectoplasty in 13 patients (10.00%), pull through operation in 11 patients (8.46%), Anoplasty in 9 patients (6.92%) and Ladd's Operation in 4 patients (3.08%) among others, as indicated in Table V. Surgical site infection and wound dehiscence were seen in 27 patients (20.77%) and 12 patients (9.23%) respectively. Sixteen patients (12.31%) had post operative pyrexia while adhesive bowel obstruction and faecal fistula were observed in 2 patients (1.54%) and 3 patients (2.31%) respectively see Table VI. Four patients (3.08%) died and these included 3 neonates (2.31%). Fourteen patients (10.77%) with colostomy had surgical site infection and of the 26 patients (20.01%) with gangrene of the bowel, 9 patients (6.92%) developed surgical site infection while 4 patients (3.08%) died post operatively. Discussion Intestinal obstruction is a common paediatric surgical problem and cuts across the different age groups in children. Its occurrence in children may be acute or chronic. Presentation in the neonate is usually acute and is the most common emergency surgical condition seen in them6 8. Published peak incidence of intestinal obstruction has usually been under the age of 1 year2; our series show that it is mostly seen in children less than 5 years with the peak in infancy which agrees with similar reports elsewhere in the country5,9. All but one neonate had congenital causes of intestinal obstruction in the present series with the only acquired condition being intussusception. Perinatal intussusception is a rare and an unusual cause of intestinal obstruction in infants10, 11. It gives a confusing clinical picture that often delays its diagnosis and treatment thus causing a high mortality10 15. The pattern of the etiology of intestinal obstruction in this study agrees with the previously reported patterns with intussusception as the most common1 3,5,15 19, although our findings also showed a slight variation in the incidence of other causes of intestinal obstruction in this series compared to these previous reports1,4.The obstructed external hernias were more of inguinoscrotal hernias; only 2 patients (1.54%) had obstructed umbilical hernia. This is contrary to a report by Archibong et al4 in which more of obstructed umbilical hernias than groin hernias were reported. Surgical complications related to Ascaris infestation do not occur frequently nowadays because of the common use of antihelminthic agents and the success of medical treatment20. Previous reports showed that an increase in the worm load in a child could increase the risk of intestinal obstruction from worm impaction and suggested that the risk can be reduced through repeated massive treatment, improved sanitation and increased health education21,22. These may probably explain the relatively low incidence of worm impaction causing intestinal obstruction in this report compared with previous reports1, 4. We observed that upper gastro intestinal obstruction is still more common than lower gastro intestinal obstruction as suggested by previous studies1-5. The relatively high incidence of adhesive bowel obstruction was found to be due to previous peritonitis from perforated typhoid ileitis. Although, 8 out of the 11 patients with peritoneal adhesions had previous surgery, it is possible that the remaining could have had previous intra abdominal infections. The classical features of intestinal obstruction, namely, vomiting, excessive crying/abdominal pain, constipation and abdominal distension were observed in over 34% of our patients and this is consistent with reports from other parts of the country1 2. Postoperative complications related to sepsis occurred more commonly in this study. Surgical site infection was the most common while septicemia and post operative pyrexia were the other common occurrences. We believe that these complications resulted from the operative findings of bowel gangrene with intestinal perforation and peritonitis which prolonged their duration of hospital stay. Our overall mortality is low compared with other reports in this country1 4. Conclusion In conclusion, acquired causes of intestinal obstruction are still more common than the congenital causes and are mostly upper gastrointestinal in origin. The aetiological pattern and clinical presentation of intestinal obstruction is still similar to previous reports from the other parts of the country2,4 5. Though the mortality is low, the management of the patients is still associated with high morbidity (60.78%) in our environment. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09038t5.jpg] [hs09038t4.jpg] [hs09038t1.jpg] [hs09038t2b.jpg] [hs09038t3.jpg] [hs09038t6.jpg] [hs09038t2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}