 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 174-178 Epstein Barr virus latent membrane protein-1 in Hodgkin's lymphoma in Nigerians *Adelusola KA1, Titiloye NA2, Rotimi O3, Durosinmi M4 1-Department of Morbid Anatomy & Forensic Medicine, Obafemi Awolowo University, Ile-Ife, Nigeria Code Number: hs09039 Abstract Background: The burden of lymphomas on the health care system in Nigeria is enormous. Correct diagnosis
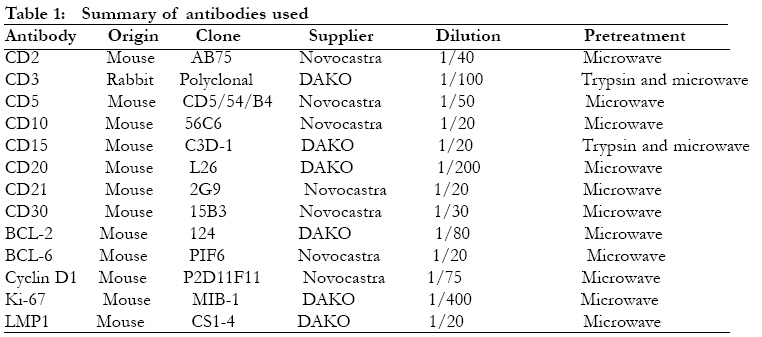
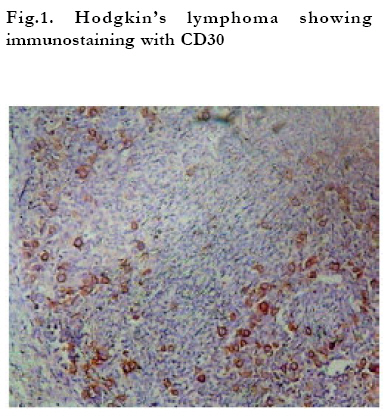
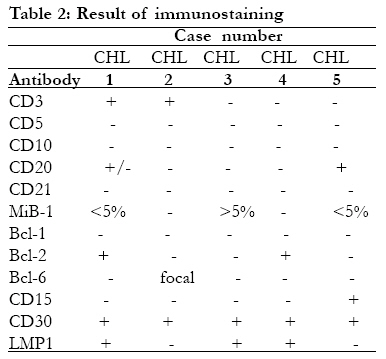
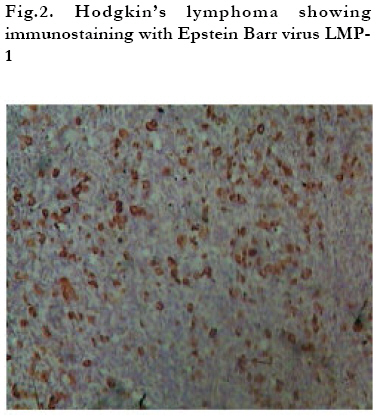
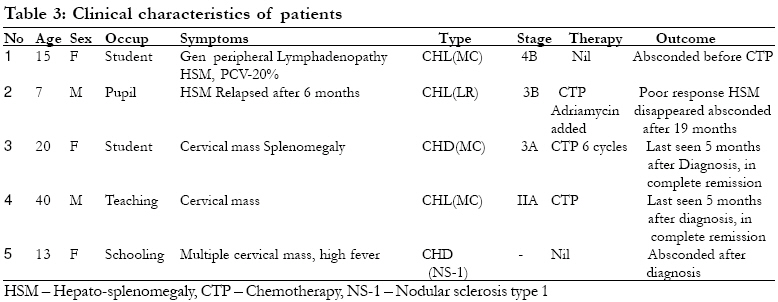
and identification of aetiological factor are important steps in reducing this burden. Running title: Epstein-Barr virus, Hodgkin's lymphoma in Nigerians. Introduction Hodgkin's lymphoma (HL) is an unusual lymphoid neoplasm in that the bulk of the tumour is composed of reactive inflammatory cells within which are scattered a few morphologically abnormal mononucleated and multinucleated neoplastic giant cells called Hodgkin's and Reed-Sternberg (R-S) cells. It is now known that the R-S cell is a germinal centre B-cell with non-productive immunoglobulin gene rearrangement, representing a failed attempt at antibody production1. The WHO sub-classifies HL into classical Hodgkin's disease and the nodular lymphocyte predominance Hodgkin's disease (NLPHL). HL is high on the list of malignancies associated with the Epstein Barr virus (EBV)2, an association that is reported by some authors to have some prognostic significance3. Familial cases associated with EBV and with linkage to class 1 HLA are known4. This as well as other studies suggest some genetic factors in the aetiology of HL5. The literature on Hodgkin's disease in Nigerians is extremely scarce, with just a passing reference to HL and virtually no focus on the histopathology aspect particularly the association with EBV6,7. Moreover, many of the literature are rather old, predating the use of cellular markers for lymphomas in general and the R-S cell and EBV in particular. Though not specific for R-S cells the cellular markers for R-S cells to date remain CD15 and CD30. It is likely the EBV plays a role in the aetiology of HL in Nigeria. This paper reports on the immunophenotyping of cases of HL seen within a period of six years in a university teaching hospital in Nigeria. The aim is to document the possible involvement of EBV in the cases seen. Materials and Methods Eight out of 55 cases diagnosed as lymphoma by H&E only between 1999 and 2004 at the histopathology department of the Obafemi Awolowo University Teaching Hospital, Ile-Ife in Nigeria were Hodgkin's lymphoma. These 8 cases were immunophenotyped using the indirect immunoperoxidase method. Serial sections of 5? formalin-fixed, paraffin-embedded tissue were cut. Sections were dewaxed in xylene and rehydrated in industrial methylated spirit (IMS). Endogenous peroxidase activity was blocked by incubation in 3% hydrogen peroxide. Antigen retrieval was done by microwave heating in combination with trypsination. Sections were incubated in swine serum for 10 minutes, followed by incubation in 1% tris-buffered saline (TBS) and 0.1% bovine serum albumin (BSA). Sections were incubated with the primary antibody appropriately diluted in TBS and BSA at room temperature for one hour (see table 1 for the summary of primary antibodies used). After washings in TBS/tween sections were incubated with secondary biotinylated swine anti-rabbit immunoglobulin for 45 minutes at room temperature and conjugated with avidin-biotin complex for 45 minutes. Reaction products were visualised using a colour solution consisting of diaminibenzidine, 30% hydrogen peroxide and TBS. Sections were thereafter stained with haematoxylin, dehydrated in IMS, cleared in xylene and mounted. Immunohistochemical controls were performed by replacing the primary antibody with non-immune serum. The diagnosis of HL was based on the characteristic cellular morphology of HL and immunoreactivity with CD15, CD30, and in some cases, also EBV LMP1. Results Only five cases out of the original 8 diagnosed as HL by routine Hand E stain only were found to be true HL on immunophenotyping. They were positive for one or two markers of R-S cell CD15 and CD30 in addition to showing the characteristic background cellular appearance of HL by Hand E stain. The remaining 3 turned out to be non-Hodgkin's lymphoma (NHL) by immunophenotyping. They comprised diffuse large B cell lymphoma (n-2), and null cell anaplastic large cell lymphoma (n=1). Fig. 1 shows immunostaining with CD30. There were two males and three females. All five cases of HL were classical HL: 3 mixed cellularity (MC), 1 nodular sclerosis (NS) type 1 and 1 lymphocyte-rich (LR) classical HL. Table 2 shows the result of immunostaining of the five cases. Three cases (60%) were EBV+ tumours as shown by immunoreactivity with LMP1 (Fig.2). The clinical characteristics of the patients are as shown in Table 3. The oldest patient was 40 years and the youngest 7 years. Four of the five patients were of school age and they presented at an advanced disease stage namely 3B and 4B. Cervical lymphadenopathy followed by splenomegaly were the most common presenting signs. Only two patients could afford the cost of chemotherapy, with good results in two, at least initially. Eventually all were lost to follow-up after varying periods of time. Discussion This is a report on a series 5 cases of immunohistochemisry-confirmed HL seen in a teaching hospital over a 6-year period. This low number of cases compared with the number of NHL seen over the same period is not surprising. Most lymphomas are non-Hodgkin's. There has also been a steady rise in the incidence of NHL since the middle of the twentieth century, whereas the incidence of HL has remained more or less flat. The common presenting sign in all the cases in this study was cervical lymph node enlargement, and this is in keeping with the fact that, HL is, in most cases a nodal disease. All the patients were young with 60% being in the paediatric age group. The oldest in the series was 40 years. Childhood HL is known to be heterogenous. Certain subtypes are commonly seen at some periods of life. NLPHD and the mixed cellularity subtypes, for example may predominate in preadolescent children8. In this study out of the three cases of MC subtype seen the only case seen in preadolescent age was in a 15-year old girl. Because of the small number of cases seen, it may be difficult to conclude that the MC subtype is uncommon in adolescents in Nigeria or otherwise. The association of HL with EBV is well known and 30-50% of HL is known to be EBV-associated. However, the association of EBV with HL is known to depend on the histologic subtype, sex, ethnicity, age and country of residence. EBV-positive HL appears to be less common in developed countries but much higher in underdeveloped countries9. Thus in the study by Katebi et al in Iran 93% of the cases of HL studied was EBV-positive10, whereas in the study by Herling et al the MD Anderson cancer centre in Texas only 21% of the cases showed EBV LMP-1 expression11 In the current study 60% of the cases seen showed EBV LMP-1 positivity. A study in Vietnamese children showed that nearly all cases of HL, including the NLPHL subtype were associated with EBV12. The association between tumour EBV status and clinical outcome in HL is still controversial13. Several studies have shown that MC is the most common subtype of HL associated with the EBV14,10,11. All the three cases of MC subtype in this study were EBV-positive. Incidentally these were the only EBV-positive cases. The survival of EBV-positive HL in the elderly and immunosuppressed is poor15. In a large population-based study of classical HL Keegan et al3 found that the effect of EBV on survival depends on age and that in children less than 15 years old the presence of EBV was associated with a favourable survival. In the study by Krugmann et al.14 patients with EBV-associated disease showed a significant longer mean time to first relapse compared with EBV-negative cases, although overall survival did not correlate with EBV association. The fact that three of the patients in this study were lost to follow-up after a short period ranging from 5 months to 19 months and two other patients absconded prior to chemotherapy does not give room for discussion on the clinical course and prognosis with respect to association with EBV in this study. This peculiar problem commonly encountered by clinicians and pathologists sometimes makes it difficult to comment on the courses and outcomes of diseases in some cases. This study shows that there is association between EBV and HL in Nigerians, in particular with the MC subtype. The existence of an underlying immunosuppression has been suggested as the reason for the high incidence of EBV-positive cases of HL in underdeveloped countries. Various infections (apart from the human immunodeficiency virus infection) and malnutrition are some of the possible causes of immunosuppression in underdeveloped countries. Since the bulk of the viral genomes in HL are in monoclonal form infection of tumour cells most likely has occurred before their clonal expansion. Obviously there is need for a larger study to confirm the association of EBV with the various subtypes of HL in Nigerians. This study also illustrates the problem of diagnosis, treatment and follow-up of patients with malignancy in a developing country. Durosinmi et al16 had previously alluded to the problem of cancer treatment in a developing country where the majority of the populace is poor, as in Nigeria. Many patients cannot afford the cost of investigation, making staging very difficult. Most cannot afford the cost of cancer treatment and are lost to follow-up. Urgent steps need to be taken by policy makers in the health sector to address these and other issues that constitute constraints to effective healthcare delivery to all. Acknowledgement The cases reported in this study were immunophenotyped in the laboratory of Prof. K.A. MacLennan, at the Cancer Medicine Research Unit, St. James's University Hospital Leeds, UK. He is thankfully acknowledged. The trip was sponsored through Obafemi Awolowo University Research Committee Grant. We also wish to thank Dr. Filomena Esteves and Ailsa Rose, both of the Cancer Medicine Research Unit, St. James's University Hospital, Leeds, UK for their immense technical assistance. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09039t3.jpg] [hs09039t1.jpg] [hs09039f1.jpg] [hs09039f2.jpg] [hs09039t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}