 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 193-199 Case finding for hypertension in young adult patients attending a Missionary Hospital in Nigeria *Ekore RI1, Ajayi IO2, Arije A3 1-University Health Services (Jaja Clinic), University of Ibadan Code Number: hs09042 Abstract Objectives: This study was carried out to search for cases of undetected hypertension in young adult male and
non-pregnant female patients (18 - 44years) attending a catholic mission hospital in Ibadan, Nigeria so as to provide evidence
for routine blood pressure checks in this age group. It also sought to determine risk factors present in those found to
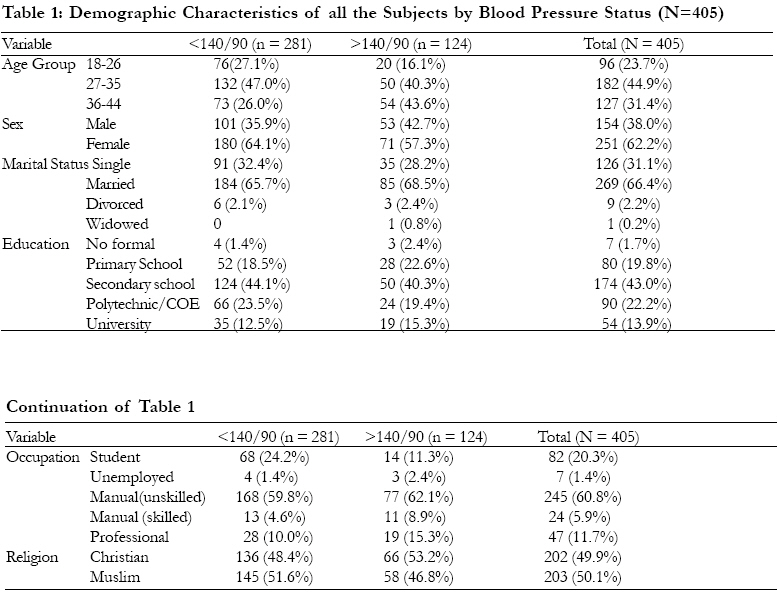
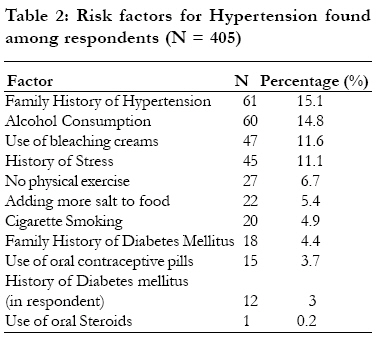
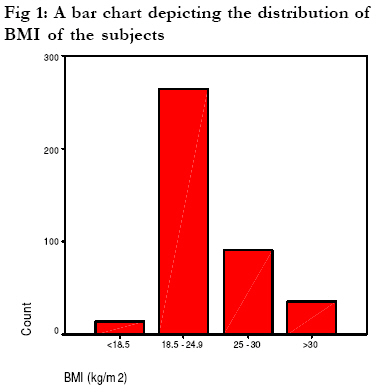
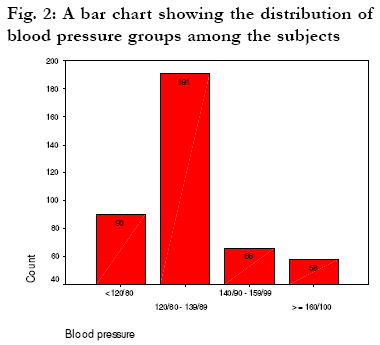
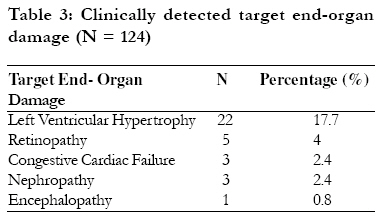
be hypertensive and to detect complications of hypertension, if present. Introduction Hypertension is a chronic illness that affects people of all age groups, both sexes and at the same time cuts across all socio-economic classes. It is said to exist when the value of the systolic blood pressure is equal to or greater than 140 mmHg, and the diastolic blood pressure is equal to or greater than 90 mmHg1. Case finding refers to the process of searching for asymptomatic disease or risk factors for a disease among patients who are consulting a physician in a hospital setting for unrelated symptoms2. It is a process of opportunistic screening which involves using the time when a patient is involved with the medical services to measure aspects of their health, as opposed to population screening which involves setting up services specifically aimed at identifying problems3. Case finding is the method used in family practice and is an aspect of screening which, basically, is a form of secondary prevention. Some identified risk factors for the development of hypertension include cigarette smoking, obesity, lack of regular exercise, dyslipidaemia, diabetes mellitus, sleep apnoea, microalbuminuria or estimated glomerular filtration rate (GFR) 60ml/min, increasing age (>55 years for men; >65 years for women), family history of premature cardiovascular disease or hypertension, African American (black) ancestry, use of oral contraceptive pills/hormones, long-term use of steroid (oral or topical), stress, excessive alcohol consumption, excessive dietary sodium (salt) intake, and insufficient intake of potassium1. Some of these risk factors are modifiable while others are not. Epidemiology Hypertension is the most common chronic non-communicable disease world-wide2, the most common cardiovascular problem in the world4 and it affects approximately one billion individuals worldwide1. It is very common in the African, with a prevalence of 10 - 15% in the adult population5, 6. Studies done in Nigeria revealed prevalence rates of 5 - 10% of rural and 10 12% of urban communities7, and 17 - 20%4,8. Another study done on a Nigerian population revealed a prevalence rate of 7% among persons aged over 25 years 9. A study done on black Africans with hypertensive heart failure revealed that 44% of the subjects were unaware that they had hypertension5 while a report of observations from some studies done on hypertension in Nigeria stated that less than a third of those with high blood pressure are aware of the fact that they are hypertensive and less than a third of those who are aware that they have the disease are under any form of treatment7. A population-based study done on young male adult military recruits in Singapore revealed a prevalence rate of 1.6%, after ruling out white-coat hypertension by means of ambulatory blood pressure monitoring among the subjects. However, there is a dearth of data on hypertension in young adults in Nigeria. The study was designed to detect cases of undiagnosed hypertension in young adult patients presenting to the hospital for the first time. It was also aimed at determining the risk factors and to detect the presence of target organ damage in those found to be hypertensive. Methods The study was a hospital-based, descriptive cross-sectional one which took place at the Out-patient Department of St. Mary's Catholic General Hospital, Eleta, Ibadan. It is a secondary health care mission hospital located in the core of Ibadan in Nigeria. All consenting young adult male and non-pregnant female patients, aged 18 44 years and not acutely ill (not requiring hospital admission and urgent care), attending the hospital for the first time and not known hypertensive patients, participated in the study. Consecutive sampling method was used and the sample size was 405. Ethical approval was granted by The University of Ibadan/University College Hospital (UCH) Institutional Review Board. Individual consent was obtained from the participants Data for the study was collected as a single survey using a semi-structured questionnaire administered by the researchers. This was done in two parts: Part one Informed verbal and written consent were obtained from patients who met the inclusion criteria. Questionnaires were then administered to them. The blood pressure of each patient was measured after the patients had rested for about 10-15 minutes10, with the patient sitting up with the arm bared, supported and positioned at heart level, using a mercury sphygmomanometer (Accoson) with an appropriate size arm cuff11, 7. A second and then a third reading were taken again at 5 minutes intervals and the average blood pressure calculated. Physical examination of all the systems was then carried out on the subjects, including anthropometric measurements like weight in kilograms (kg), height in meters (m), body mass index, waist circumference, measured to the nearest centimeters (cm), hip circumference, measured to the nearest centimeters (cm), waist-to-hip ratio. Those with sustained elevated blood pressure readings that fell within the stage 1 class of hypertension were given a short appointment (two weeks) during which two more blood pressure measurements were taken and the average blood pressure reading noted. However, those with severe hypertension (stage 2 JNC 7) at the initial visit proceeded immediately to Part 2 of the study. Those with hypertensive urgencies were admitted to the medical ward for in-patient care. Part two The subjects with sustained elevated blood pressures (hypertension) were recruited to participate in the second part of the study during which they had their pulse rates and blood pressure rechecked, and fundoscopy done to detect retinal changes. They were then informed of the fact that they had hypertension, counseled and educated on lifestyle modification. For those who were still willing to continue with the study, blood samples were taken and sent to the laboratory for analysis, including packed cell volume (PCV), serum total cholesterol, random blood glucose, serum potassium, serum urea, serum creatinine. Urine samples were also collected for analysis (protein and sugar). In addition, those with stage 1 hypertension were advised to adopt lifestyle modification measures alone, and their blood pressures were to be monitored for the next three months, while those with stage 2 hypertension were placed on anti-hypertensive medication, in addition to lifestyle modification measures. They were all given follow-up appointments. Results Data collected was analyzed with the eleventh version of Statistical Package for the Social Sciences (SPSS) software. Descriptive statistics such as mean and median were used to describe the data. Chi-square and student's t-test were used to explore association between categorical and continuous variables respectively. One-way ANOVA was used to test differences in groups. The p-value was set at 5% level of significance. A total of four hundred and five (405) consenting young adults aged 18 and 44 years, that met the inclusion criteria, took part in the study. Table 1 shows the demographic characteristics of all the subjects as described subsequently. The mean age of the subjects was 31.6 ±6.9 years. The demographic characteristics as shown in Table 1 reveals that half of the subjects, 182 (44.9%) were in the age-group of 27-35 years. Those who are in the 36 - 44 years age group were 127 (31.4%), whereas those in the 18-26 years group were 96 (23.7%). An independent t-test analysis of age with systolic blood pressure showed a significant difference (t = 4.39, df = 403, p < 0.05), and t-test analysis of age with diastolic blood pressure also showed a significant difference (t = 4.22, df = 403, p <0.05). This means that those with older age had higher blood pressure than those with younger age, that is, age is a significant factor influencing both systolic and diastolic blood pressure. There were 154 (38%) males and 251 (62%) females in the study population. Fifty-three (42.7%) of the hypertensive subjects were male while 71 (57.3%) of the hypertensive subjects were female. Chi-square test done to compare sex with blood pressure did not reveal a significant association (÷2 = 3.36, df = 403, pns). Two hundred and forty-five (60.5%) were manual unskilled workers, 24 (5.9%) were manual skilled workers, 47 (11.6%) were professional, 82 (20.2%) were students and 7(1.7%) were either unemployed or full-time housewives. The result of a one-way analysis of variance (ANOVA) done to compare the occupation of the subjects and their blood pressures indicated significant difference in occupational levels and the blood pressure of the subjects (F (4,398)=4.29, p < 0.01). The mean monthly income of the respondents was An independent sample t-test analysis done to compare monthly income and systolic blood pressure revealed that there was no significant difference between the two (t = 1.74, pns) and that done to compare monthly income and diastolic blood pressure respectively was also not significant (t = 1.21, pns). These results imply that monthly income is not a significant factor in systolic and diastolic blood pressure among young adults. Table 2 shows a list of other known risk factors for hypertension (apart from those already mentioned in the demographic data) found among all the study subjects. Chi-square tests and one-way analysis of variance (ANOVA) were done to compare the effect of risk factors on blood pressure in the subjects. None of the risk factors had a significant association with blood pressure.Body Mass Index and Blood Pressure The mean weight of the study population was 64.0 ±11.5 kg, the mean height was 1.64 ±0.08 m while the mean body mass index of the subjects was 23.7 ±4.3 kg/m2. Figure 1 is a bar chart depicting the body mass index of the subjects. Independent t-test analysis of BMI with systolic and diastolic blood pressures revealed significant differences (t = 2.92, df = 403, p <0.05) between the hypertensive and non-hypertensive subjects. Waist Circumference, Hip Circumference, Waist-to-hip Ratio and Blood Pressure The mean waist circumference was 85±12 cm while the mean hip circumference was 101±12 cm. The mean waist-to-hip ratio was 0.84 ±0.08. Statistical analysis using the independent t-test to compare waist circumference, hip circumference and waist-to-hip ratio with systolic and diastolic blood pressure revealed significant differences between both waist and hip circumference with systolic and diastolic blood pressure. The results of the t-test analysis were as follows: waist circumference and systolic blood pressure (t=3.72, df=403, p <0.05), waist circumference and diastolic blood pressure (t=4.42, df=403, p < 0.05), hip circumference and systolic blood pressure (t=3.54, df=403, p < 0.01), hip circumference and diastolic blood pressure (t=3.72, df=403, p <0.05). However, there was no significant difference between waist-to-hip ratio and both systolic blood pressure (t = 1.27, df = 403, p > 0.05), and diastolic blood pressure (t = 1.96, df = 403, pns) between the hypertensive and non-hypertensive subjects. Prevalence of Hypertension and its Complications A total of 124 (30.6%) out of the 405 subjects were hypertensive, giving a hospital prevalence rate of 30.6%. Sixty-six (53.2%) of the hypertensive patients had stage I hypertension and 58 (46.8%) had stage II hypertension. Mean (SD) systolic blood pressure was 129.5 ±21.7 and mean (SD) diastolic blood pressure was 85.7 ±14.01. One hundred and ninety-one subjects (47.2%) were pre-hypertensive and 90 (22.2%) were normotensive. The mean (SD) systolic blood pressure of the hypertensive subjects was 154.8 ±19.9 while the diastolic blood pressure of the hypertensive subjects was 101.5 ± 10.9.The distribution of blood pressure groups among all the subjects is shown in figure 2. Among the subjects, some indications of complications and possible target end-organ damage were detected and these are shown in Table 3, which reveals that 22 (17.7%) of the hypertensive subjects had left ventricular hypertrophy, 5 (4.0%) had hypertensive retinopathy, 3 (2.4%) had congestive cardiac failure, 3 (2.4 %) had features suggestive of hypertensive nephropathy while 1 (0.8%) had encephalopathy. Among those with retinopathy, four of the subjects had stage 1 retinopathy while one had stage IV retinopathy. Discussion This descriptive cross-sectional study was done to find cases of undetected hypertension in young adult patients, find out predisposing risk factors in them and detect complications due to the hypertension. A total of 124 (30.6%) subjects were hypertensive. This prevalence is relatively high, considering the age range of the study population. This figure is higher than that of a similar study which reported a prevalence of 1.6% in young adult military recruits in Singapore, although in that study, they were able to rule out cases of white-coat hypertension12. However, it is lower than the prevalence of 44% seen in another study5. The difference in prevalence of undetected hypertension in both cases may be attributable to the older age of the subjects in the latter. The prevalence of undetected hypertension in young adults found in this study is also significantly higher than that found by Akinkugbe in a review of hypertension studies done in adult populations in urban and rural Nigeria7. The relatively lower prevalence rates reported by Akinkugbe may, however, be due to the fact that a higher cut-off blood pressure value (160/100 mmHg) was used to define hypertension. That not withstanding, analysis revealed that hypertension in this age group could be significant. This calls for a re-think and re-orientation for health care workers and policy makers towards directing more attention to, and providing funds to increase awareness, detect and adequately manage hypertension, particularly in young adults as virtually all attention has been diverted to management of HIV/AIDS which is very common in this age group, thereby neglecting chronic diseases such as hypertension which is silently maiming and killing young adults who make up a large proportion of the work force of the nation and are the potential leaders of tomorrow. The age range for the study was 18 44 years 13. Analysis showed a positive and significant relationship between age and blood pressure. This corroborates existing information in most literature with regards to increasing age being a predisposing factor in the development of hypertension2, 14. The subjects were mainly manual unskilled workers. Again, this is not surprising as most of the subjects attained only a secondary education and are virtually all into trading. There was a significant association between occupation and blood pressure, with differences in mean blood pressure increasing with rise in occupational status. The mean income per month was N7, 852 (H" $65). It is surprising that a very large proportion of these traders had no idea of their daily or monthly earnings. The association between monthly income and blood pressure was not significant and this is in contrast to findings from studies which state that there is a significant association between socio-economic status and the development of hypertension16,17,18,19. The study population was basically a lean one with a mean BMI of 23.7kg/m2. However, 22.5% of the subjects were overweight and 8.6% were obese. The association between BMI and blood pressure was significant (p <0.05) and supports findings from previous studies20. Waist circumference also showed a significant correlation to blood pressure. This corroborates evidence from previous studies21, 22. Waist-to-hip ratio, however, was found not to have a significant association with blood pressure (p >0.05), corroborating findings from a study that said waist circumference is a better predictor of cardiovascular disease than waist-to-hip ratio21. Clinical evidence of complications were evident in a small proportion of the subjects. With the proportion of subjects found to be hypertensive in this study, it is obvious that hypertension in young adults may not only be significant, but there may be a significant proportion of young adults with target end-organ damage that could have been detected earlier or prevented if they had been screened during routine examination. No significant association was found between lifestyle habits like diet, alcohol consumption, cigarette smoking and physical exercising. This is in contrast to findings from studies done previously23, 24. This finding not withstanding, health education on risk factors should always be provided to patients. Conclusion From observations made in this study, it can be concluded that undetected cases of hypertension exist among young adults in Ibadan, Nigeria and that complications are also present in hypertensive patients in this age group. This study has provided a greater insight to the urgent need for a change in attitude toward young adults attending hospitals in Ibadan and elsewhere in Nigeria, especially in screening them for hypertension as part of clinical examination. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09042f2.jpg] [hs09042t1.jpg] [hs09042f1.jpg] [hs09042t3.jpg] [hs09042t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}