 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, Special Issue 2, Oct, 2009, pp. S81-S85 Funding the promise: monitoring Uganda's health sector financing from an HIV/AIDS perspective Agaba E Coalition for Health Promotion and Social Development (HEPS-Uganda) Code Number: hs09051 Abstract Background: HIV/AIDS prevalence in Uganda is beginning to show an upward trend despite increased inflow of
funds to fight HIV/AIDS in Uganda. Key words: Health financing, HIV/AIDS, funding, budgeting Introduction Health spending in Uganda covers about 1/3 of what the country needs to meet its minimum health care package. According to WHO, Uganda spends only US$14 per-capita on health. Of this, US$9 is out-of-pocket and US$5 from public sector (government and donor funding) 1. The public sector needs to spend US$28 per-capita and up to US$40 when ARVs are included2. Health spending has accounted for 7-9% of the Uganda National Budget in the last five years, which clearly indicates that government funding of the health sector is low. Despite large inflows of funds to Uganda for HIV/AIDS, most people who need care cannot access it. Of the estimated 1.1 million people living with HIV/AIDS, about 150,000 need ART, but only 67,0003 are accessing it. Results from the HIV Sero-survey show an upward trend in prevalence rates of HIV infection currently at 6.4%4. This study aimed to monitor health sector financing from an HIV/AIDS perspective so as to produce recommendations for effective health service delivery mechanisms in Uganda. The specific objectives were to: (a) Establish the level of Uganda
government's commitment to funding the fight against
HIV/AIDS; Methods The study mainly used qualitative approaches to: 1) Establish the level of commitment on
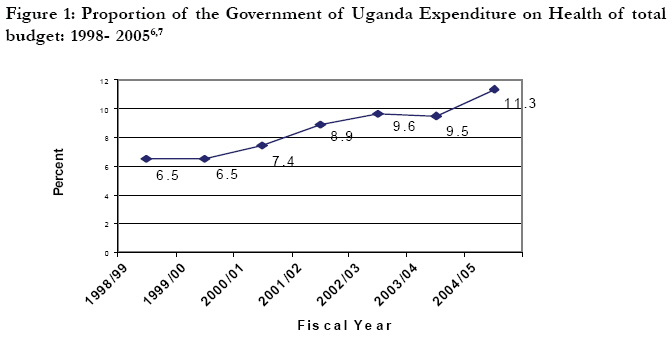
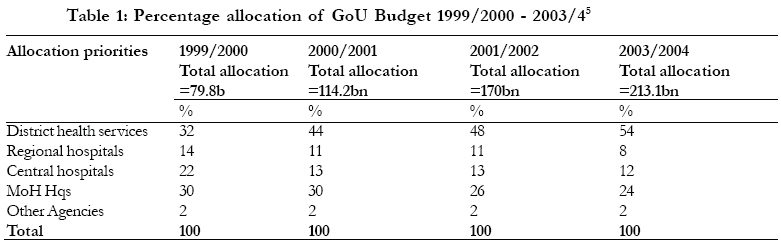
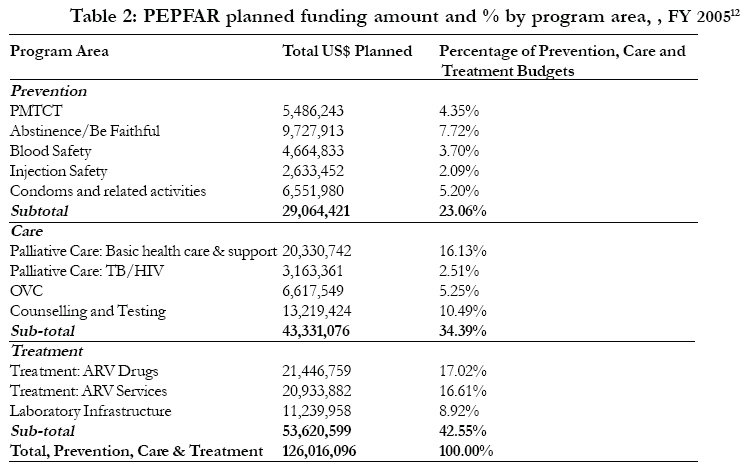
the part of the Government of Uganda (GoU) to funding the fight against HIV/AIDS; We reviewed relevant literature, undertook observations, and conducted key informant interviews with selected respondents in HIV/AIDS policy, programming, and working with communities. Thematic and content analysis guided the process and presentation of data. Primary data were collected from four districts; Lira, Soroti, Rakai and Kamwenge by trained research assistants. Districts visited were purposely selected to provide regional representation with Soroti in eastern, Lira in northern region, Rakai in south and Kamwenge in the western region. Documented data was mostly collected from Ministry of Health, Uganda AIDS Commission and other key partners. An extensive review of documented literature specific to policy and programming for HIV/AIDS at the national and district level was done. Results Allocations in national budgets (recurrent and development budgets) Between fiscal years (FY) 2000/1 and 2002/3, health received the largest proportionate rises in its budget compared to other sectors. Government of Uganda (GoU) funding-including donor budget support in that period rose from Ug.Shs114 billion (US$63 million) to Uganda Shs196 billion (US$107 million), representing 72% increase. In FY2002/3, the health sector budget constituted 9.6% of the total budget. In FY2002/3, the health sector budget constituted 9.6% of the total budget. In the following year (2003/04), health budget constituted 3% of GDP. Using the late 1990s as a baseline, existing data generally shows some gradual, albeit slow increase in health sector budget as a proportion of the overall budget. In the FY 2003/04, health was fifth while in 2004/05, it was fourth, ranked by proportionate share of the total national budget5. The proportion of health budget directly allocated to districts has increased from 32% in 1999/2000 to 48% in 2002/2003. GoU had promised to continue increasing districts' direct share to 54% of the health budget in 2003/4 as shown in Table 1 below. However, the FY2004/05 budget and Medium Term Expenditure Framework (MTEF) projections show zero growth in the following years. Allocations in district budgets (recurrent and development budgets) Local government's contributions to health have been low for many years. Available data shows that in the fiscal year 1998/99, local governments contributed only US$0.04 per capita towards health financing and in 99/2000 it fell even further to US$0.03 per capita, even with the abolition of cost sharing the picture has not changed. At the national level, whereas additional resources have been allocated for essential drugs with 50% of the non-wage health budget allocated and per capita funding for essential drugs increasing from US$0.8 in 2000/01 to US$1.85 in 2004/05, this has not been enough to stem country-wide high stock-out rates. This figure represents only a third of the US$3.5 estimated need for essential drugs (excluding ARVs)8. Nevertheless, available data shows that recurrent health spending is over US$12 per head, although public expenditure accounts for only about ¼ of this. Out-of-pocket expenditure accounts for about 70% of total expenditure - three quarters of which is spent on drugs. A high degree of donor dependence; covers about 1/3 of recurrent spending and about 90% of capital expenditure9,10. Donor support to HIV/AIDS by priority areas At the onset of the HSSP, donor project funding was the largest financing element contributing Ug.Shs135bn (55%) of the health Medium Term Expenditure Framework (MTEF). However, due to the shift towards budget support, this fell in FY2002/3, when donor project funding accounted for only 42% of total resource envelope (US$141.8bn)11. Prevention of infection with HIV/AIDS Response to the HIV/AIDS epidemic has mainly focused on prevention and control of further spread through behaviour change. In recent years there has been a shift in the global paradigm in favour of treatment is reflected in the budget and funding allocations of some of the major HIV/AIDS funding mechanisms. For instance, PEPFAR program in the FY2005 allocated almost half (42.6%) of the total prevention, care and treatment budget to treatment, and 23.63% to procuring ARV drugs and instituting ARV related services (Table 2 ). Facilities to deliver services are still inadequate in relation to demand. In the PEPFAR FY2005 budget, this program received only 4.35% (USD 5.4 million) of the total budget for prevention, care and treatment. Similarly, the GFATM allocation for the program is meagre with only US$3.5 million allocated (3.6% of the total fund approved for rounds 1 and 2) 14. Other funding mechanisms like GFATM present a similar scenario. For instance the bigger proportion (55%) of the Global Fund money for rounds 1 and 2, i.e. FY2003 and FY2004 was allocated to HIV/AIDS prevention 13. Discussion District financing for HIV/AIDS from locally generated funds is irrelevant and no allocations are made in district budgets for HIV/AIDS activities. This makes allocation of the funds difficult because one is required to apportion available funds not according to need but equity. We use the credit line but all this depends on money allocated to us on the PHC funds and the money is not enough. Like we have a budget of 23 million, half is for drugs. Our consumption for cotrimoxazole here is 2 tins per week, so when they supply us with 5 tins for three months, then they are not enough (HSD, Health in-charge, Lira district) Uganda continues to enjoy bilateral and multilateral support from partners, financially and materially to address HIV/AIDS. But despite increased funding for the health sector, health expenditure is still very low. However it was not possible to isolate specific HIV/AIDS allocations from the overall health budget. From this analysis, the available funding opportunities are mostly donor sourced and therefore, donor funding is considered an indispensable ingredient in HIV/AIDS financing; if donors closed or stopped funding HIV/AIDS activities, districts would have to reduce expenditure on other aspects of health, such as malaria, to fund HIV/AIDS. On the other hand, districts indicated that they could commit real monies for HIV/AIDS but are sometimes frustrated by the Central Government, because funds from the centre are unreliable. "We plan for some activities but don't get all the money. Like Primary health care: we expected 1.2 billion but got 50%...so if drugs were to take 50% then what has been got is again split (DDHS Lira district)" Over the years, Uganda has undertaken programs to reduce transmission of HIV from mothers to children either during pregnancy, labour/delivery and through breastfeeding. Coverage was expanded to cover 56 districts at the end of 200414. However, facilities to deliver services are still inadequate in relation to demand. In the PEPFAR FY2005 budget, this program received only 4.35% (USD 5.4 million) of the total budget for prevention, care and treatment. Similarly, the GFATM allocation for the program is meagre with only US$3.5 million allocated (3.6% of the total fund approved for rounds 1 and 2) 14. Harmonization of the different funding mechanisms Uganda AIDS Commission (UAC) is mandated to coordinate HIV/AIDS response and harmonise the different funding mechanisms. UAC has developed an inventory of agencies with HIV/AIDS activities showing which community has which actors and the gaps. Initiatives (like the UNAIDS Country Response Information System (CRIS)) exist to harmonise the different resource tracking systems promoted at the different levels to track resources for HIV/AIDS activities and Lot Quality Assurance and Supervision (LQA). UAC has also developed and disseminated coordination guidelines for districts and lower level governments. All initiatives are in support of harmonisation of the funding mechanisms; yet in reality almost all the districts visited have achieved no harmonisation. This is partly due to partial information-sharing, especially regarding funds. Most CSOs give the offices of the focal point officers only indicative financing figures at the beginning of the financial years. The indicative figures simply show which source is committing what amount of money, but sometimes these figures change in the process of implementation. Districts also argue that even the way some HIV/AIDS programmes are run (in reference to PMTCT program) makes it difficult for the districts to know how much funds have come into the district. However, Uganda has also put in place Partnership Forum on HIV/AIDS under UAC to discuss, share information, build consensus, undertake joint planning, share experiences and practices, and provide mutual support among all constituencies, including district representatives. Overall, harmonisation of the funding mechanisms is still difficult. Funding Gaps The current funding level is below what is required to fully implement Health Sector Strategic Plan (HSSP). This requires about US$28 per capita to meet the target 2.5 treatment episodes per person per year compared to the current US$9 per capita14. The estimated immediate shortfall in health sector funding is about Ug.Shs 200 billion. This gap cannot be closed until the fiscal year 2020, even if health budget continued to grow at 6% per year to achieve 15% of the GoU budget15. However, it would be possible to close this gap with stronger political commitment. While reflecting on the Abuja commitment of 15% funding for health, districts acknowledged that they and the country at large are still a long way from achieving the target. They observed that if the commitment is being measured against local revenue committed, they are still far off target. But if it includes budget support from donors, then the country is near the target. It was observed that a lot of costs are integrated given that HIV/AIDS is a cross cutting issue. Sustainability of funding for HIV/AIDS programmes Nearly half of Uganda's budget is financed by donors through soft loans and grants. Some of this money goes directly into the GoU budget to finance recurrent expenditure, and another portion is committed to development projects - focusing on infrastructure development, social service provision, private sector development, decentralisation, and agriculture modernisation, as well as policy and institutional reform. In fact before abolition of user fees in public health units and hospitals in 2000, households were the highest individual contributor to the health sector budget closely followed by donors. In all districts visited, most HIV/AIDS initiatives are financed by donors. Some districts have lobbied development partners for funds to implement planned activities in the District Strategic Plans, and this is the most common way to mobilise resources. Conclusions and recommendations Public health spending is still less than what is needed to realise the target of 2.5 health treatments per person per year; thus greater commitment of state funds is essential to the longevity of scaled-up programs, particularly treatment. Although health expenditure accounts for around 6% of Uganda's GDP, drug supply at the health facilities has remained inadequate. Higher priority must be given to per capita funding for essential drugs and uninterrupted access to ARVs and other drugs for treating OIs cannot be overemphasized. At this rate, shortfall in HIV/AIDS funding is about Ug.Shs 200 billion and with a 6% consistent growth rate in the health budget will only close this gap by 2020, when the country achieves 15% of the GoU budget. Therefore stronger political commitment, is needed improved equity in distribution of resources, and increased impact assessment of HIV/AIDS budget. Acknowledgements The author would like to thank ActionAid International Uganda for providing financial assistance. The author knowledge HEPS-U, EQUINET and Uganda Health Equity Network for capacity support towards the publication of this paper. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09051t1.jpg] [hs09051t2.jpg] [hs09051f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}