 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, Special Issue 2, Oct, 2009, pp. S90-S96 Delivering on a gendered definition of health needs in local government budgeting: experiences and concepts Buyana K. Social Sciences, Cavendish University Uganda Code Number: hs09053 Abstract Background: Local governments are granted budgetary power in the Local Governments Act of the Republic of
Uganda2, which allows for local-level participation and flexibility in the allocation of financial grants channelled annually from central to
local governments. The act prescribes a legal mandate to allocate public resources based on local priorities including the
health needs of women compared with men. This study investigated the responsiveness of local government budgeting to
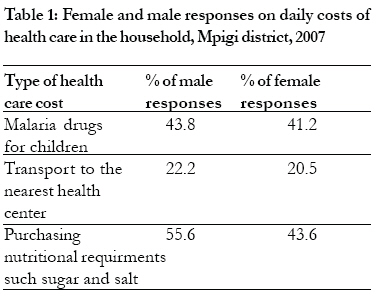
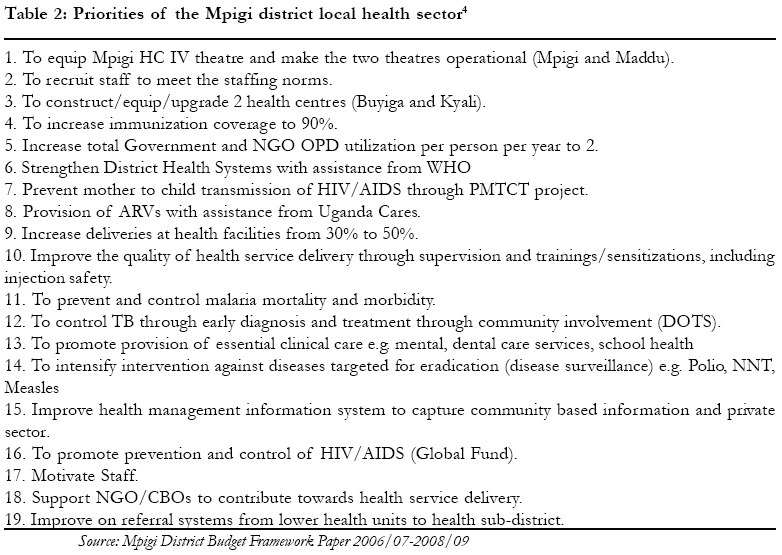
the health needs of women as compared to men. Keywords: Gender, Health Needs and Local Government Budgeting Introduction Local government budgeting is a policy reform direction under the larger decentralisation framework, adopted by governments across sub-Saharan Africa1. In Uganda, local government budgeting came into being after enacting the Local Governments Act of the Republic of Uganda2 (LGA). The act stipulates that the decentralisation of budgeting responsibilities shall involve locally elected representatives to table the needs of the local people. The LGA further provides for one third of women's representation in Local Governments Technical Planning Committees (responsible for overseeing the budgeting process at district level) to balance the concerns of women and men in local government budgeting. To reinforce the budgeting autonomy of local governments, the Fiscal Decentralization Strategy of the Republic of Uganda3 was also passed to allow local-level flexibility in the allocation of recurrent sector conditional grants (financial allocations channelled annually from central to local governments). As such, local governments in Uganda have a legally prescribed mandate to allocate public resources based on the health priorities of women compared with men. Therefore, priority setting in local-level budgeting should be based on a broad gendered understanding of health needs. Accordingly, a two-fold framework is presented in this paper for the gendered categorisation of health needs, based on the lived experiences of women as compared to men in Mpigi district. The framework includes health needs arising out of common disease infections on the one hand; and those premised on socio-economic constraints on the other hand. Methods The findings were generated through a qualitative study carried out in a purposively selected district - Mpigi, central Uganda. The district is divided into seventeen sub-counties and Bulo sub-County was randomly selected for the study. Bulo sub-County has a population density of 199-276 persons per square kilometre with 3,170 households (7,477 males and 8,088 females) according to Mpigi District Planning Unit (2007). The sub-County is further divided into five parishes with several villages and Waduduma village in the east of Bwala parish was randomly selected for the study. A set of qualitative data collection methods were used, including: a) three (3) focus group discussions that comprised of 8 male and 8 female residents of Bulo sub-County; b) face-to-face interviews with a random sample of 120 households in Bulo sub-County, 75% of which were male-headed and 25% female-headed, ; c) key informant interviews with ten (10) administrative officers in Mpigi district ; and d) desk-review of the Mpigi district Budget Framework Paper4.Information from focus group discussions, key informant interviews and desk-reviews was then isolated, synthesised and analysed using themes and sub-themes derived from the objectives of the study. The findings from both female-headed and male-headed households were processed using the Statistical Package for Social Scientists (SPSS) to derive descriptive statistics that were analysed and interpreted qualitatively. The data presented here, however, cannot be generalised to the entire country, but rather reflect that a two-fold gendered framework, needed to gain a broad understanding of health needs. ResultsThe Community-wide understanding of health needs Health needs in Mpigi district are diverse, ranging from health care concerns about household welfare to constraints met within the local health care system. The gendered experiences captured from Mpigi district revealed that both women and men have a broad understanding of health needs, including not only common disease infections but also social-economic constraints that affect the quality of life. Therefore the findings presented in this section are grouped into two: i) health needs that arise out of common disease infections; and ii) needs that are premised on socio-economic hardships. Gender health heeds arising out of common infectious diseases In this section, I discuss the main health needs arising out of common disease infections, as follows: 1) access to essential medicine; 2) freedom from stigma associated with HIV and AIDS; 3) the right to adequate maternal care; 4) access to safe and clean water and sanitation; and 5) access to health information. Access to essential medicines The primary concern of the community was inaccessibility to essential medicines for treatment of disease due to persistent drug stock-outs. Female and male respondents noted the increasing daily expenditure on essential medicines especially malaria drugs for children, as shown in table 1. Group discussions with the respondents revealed that local health personnel at `Tonkom' Health Center III in Bulo sub-County always complain that drugs used to prevent or cure diseases such as malaria, are not enough in terms of supply. Respondents indicated that even at the village level, local health personnel cannot administer first aid to children because of the unavailability of drugs from the sub-County health centre: …..the drugs brought to us during community-outreaches on Tuesdays and Thursdays are not enough, usually the people who need the drugs are more than what is available which forces the health workers to reduce on the dose given to each person…. An official on the Village Health Team during Focus Group Discussions in Bulo sub-County Women and men further revealed that informal relationships between health users and providers impede on the community's access to essential medicines at local government health centres: …. LC members, local business men and relatives of health personnel, receive drugs before any other person at Tonkom… Male respondent in Focus Group Discussion at Bulo sub-County From the findings above, health needs in the community are expressed in terms of local health service deficiencies. This means that the community-wide understanding of health needs is not necessarily limited to measures of high morbidity or mortality rates, that, pre-dominate local health sector budgeting, but rather the readiness of local health systems to respond to the growing demands of women compared to men for the adequate supply of essential medicines. Freedom from stigma associated with HIV and AIDS Female respondents cited stigma from local health workers at Prevention of Mother to Child Treatment (PMTCT) centres as a result of compulsory screening and testing of expectant mothers. Women explained that this is why some people are not willing to go for Routine Counselling and Testing (RCT) at local government health centres. The study also revealed that HIV-positive women endure stigmatisation from their husbands as, for example, explained in the experience below: My husband tells everybody, because of her, my son was born with this disease. My son is an innocent child but she brought him this disease…. A female respondent during a household interview in Waduduma village The same respondent indicated that for purposes of marital stability, most women have chosen not to disclose their sero-status to their sexual partners. This means that although male spouses are socially expected to be the primary care-givers to HIV positive partners, their attitude towards HIV/AIDS is sometimes socially unacceptable. This further reveals that the interaction between sociological and biological factors results into gender differentials in the risk of HIV and AIDS infection5. Household gender relations too influence women's and men's vulnerability to HIV and AIDS by shaping the negotiation of sexual relationships. Therefore, the health needs of HIV positive women and men require a gendered understanding in local health programming and budgeting. The right to adequate maternal care Regarding child deliveries at health centres, women reported that they do not acquire sufficient medical attention from local health workers and are treated unfairly in the process of accessing local maternal services. Women said that the attention received from paid health personnel differs from one person to another depending on the perception of the health worker about the behaviour of the patient. Some respondents added that some expectant mothers prefer Traditional Birth Attendants (TBAs) to government health personnel because of inappropriate reactions towards their maternal condition: .....Some women in this sub-county prefer giving birth at home because of the unfriendly behaviour of some government health workers....... A female respondent during a focus group discussion at Bulo Trading Center Therefore, the community-wide understanding of effective maternal health services is largely in terms of the quality, not the quantity of deliveries at government health centres, which usually constitute the planning yardstick for assessing the functioning of local maternal health systems. Access to safe and clean water and sanitation With regard to accessing safe and clean water for preventing water-borne epidemics, women said borehole systems are still limited to trading centres, although most people stay in the villages. But men were concerned about water shortages resulting from power cut offs that malfunction the bore hole systems in Bulo trading centre. Male respondents added that unhygienic public toilets and threats of acute cholera are caused by such periodic water shortages. Respondents lamented that local councils have failed to fairly distribute borehole systems for political reasons: areas where reigning local politicians expect more votes usually get the first priority in borehole allocation. Therefore decentralisation of water services does not necessarily offer opportunities for equitable redistribution to respond to gender health needs. And, whereas women need access to clean and safe water nearer to homesteads, men demand the same health service in the public where they carry out daily income generating activities. Access to health information Access to health information is affected by transport constraints in Mpigi district. Sensitisation programmes, for example, usually take place at locations far away from people's homesteads. Women said that the location of the `Sanitation Campaigns' in 2006 at Muduma and Kyegonza towns, deprived many community members from participating in the `Sanitation Week'. Women and men also said that they are unable to understand the Information, Education and Communication (IEC) materials pinned at health centres, electric poles, shops, and inside bars; they argued that in the villages most people are illiterate and therefore highly depend on word-of-mouth to acquire messages regarding health issues. This means that the location and language used in communal health activities, such as sanitation, can be an impediment on women's and men's right to access health information. It is important therefore to sufficiently invest in better local transportation networks and solve the existing language barriers as a way of boosting local access to health information and services. Gender health needs arising out of socio-economic constraints This section presents health needs that arise out of the gendered welfare concerns and socio-economic hardships. Such needs include: 1) the right to adequate food supplies; 2) access and control over productive employment; and 3) decision-making power in family planning. The right to adequate food supplies In households, inadequate food stuffs are a health constraint in Mpigi District. Men argued that the size of people's farm lands is small compared to their family sizes, which makes it hard to grow enough food varieties. Purchasing food such as maize flour is also very expensive for most families. Elderly women said that they often lack foodstuffs and only receive transitory incomes from relatives to feed their families. Households of elderly women depend on the presence of paid work for relatives in the city and stable social relationships with these working contacts. This form of health provisioning means that stable familial networks are part of the household health care processes. Such familial networks also require a gendered understanding because they are premised on the division of socially-shared responsibilities and the underlying motivations6. Control over productive employment The health status of families in Mpigi also depends on access to and control over productive employment. Male respondents argued that, insufficient earnings from employment threaten family welfare: ……unemployment makes a man fear that another man or the relatives of your wife shall come in to provide for the home…. Male respondent during a focus group discussion in Bulo sub-County Female interviewees also agreed that being healthy includes being able to engage in income earning activities. The respondents said that having control over productive employment reduces women's dependency on the male spouse and significantly raises women's ability to participate in decision-making. Further discussions with male interviewees revealed that having command over the distribution of health resources such as; savings for private curative health services and the transport means to the health centre impacts on a man's emotional/psychological well-being.The lived gendered experiences manifest that while the possession of finances may not be perceived as a factor in health, the decision-making power that comes with having financial resources makes access and control over productive employment a health need. However, the nature of healthcare financial contributions made by women as compared to men in the household requires a gendered understanding. This is because women, unlike men, often spend a lot of time accomplishing a number of health-related tasks even when their financial contributions to the family budget are considered to be relatively modest. But the usual health care analyses tend to be tilted towards the amount of the direct money earned and spent on familial access to local services, with less emphasis on the amount of time spent on health care work, indirectly or directly supporting the financial earnings7. Therefore the healthcare process is such that women contribute their time, labour and finance in quantities that may differ from men's contributions. Family planning decision-making The study revealed that men as primary decision-makers in the household deny women the right over fertility control. Men said that their spouses cannot make decisions related to the number of children to be borne by the couple because women's command over resources like shelter for accommodation and land for growing food is minimal. According to the respondents, women are free to stop conceiving only after bearing at least six to eight children: ….a man is the boss in the family and a woman cannot use family planning without seeking his consent… Male respondent during a household interview in Waduduma village Experiences captured on family planning imply that women with less command over the bulk of household resources only assume the right over their fertility after going through an acceptable number of pregnancies. Therefore in extending the use of contraceptives for family planning, local governments need to consider the gendered power relations in decision-making regarding the distribution of household resources. To conclude on the community-wide understanding of health needs, the main argument is: women's and men's definition of health needs is two-fold, which, consists of the daily requirements that arise out of common disease infections and the socio-economic constraints that affect the quality of life. The section that follows presents findings on the priorities of the district budgeting process, to ultimately draw a comparison between the community-wide and local health sector understanding of health needs. The priorities of the district health sector In this section, I present the findings on the priorities of the district health care budget. The approach used in priority-setting is mainly based on disease control measures (see Table 2). According to officials in the Department of District Health Services (DDHS) objectives 4, 8, 11, 12, and 14 are in line with people's health problems. The officials said that people are generally affected by constant malaria attacks (adults and children), HIV/AIDS among sexual partners, prevalence of Tuberculosis, abortions among adolescents, epilepsy, syphilis, diarrhoea, cholera, coughs and colds. The interviewees further argued that the aforementioned health problems affect both women and men, and that is why they are a priority in the local government health sector. Further probing also revealed that priority-setting in local government budgeting involves all stakeholders, i.e. female and male councillors, district technical staff, and civil society organisations who meet to discuss local needs and how they should be addressed, in line with the guidelines and oversight responsibilities of the central government. The involvement of several actors shows that budgeting at the local government level provides possibilities for the broad gendered understanding of health needs. However, further discussions with the official in the District Finance Department revealed that the final budget priorities must be in line with the indicative sector ceilings and guidelines of the central government. This implies that the technocratic processes imposed on budget decision-making may not readily change to ensure that the priorities set are a reflection of the broad community-wide understanding and gendered nature of health needs. At the same time female and male representatives of the communities do not `functionally' participate in budgeting. For instance, local council officials in Bulo who sit on the sub-county Health Management Committee agreed that their views are sought during the Quarterly Work Plan meetings and budgeting. The interviewees, however, said that local needs in budgeting are restricted to the guidelines of the national Ministry of Health during such meetings: …. In the quarterly meetings our views are always ignored because the district health officials say we have to follow the guidelines of the Ministry of Health…. A local representative indicated in Mpigi District These experiences imply that the outcome of budgeting is an arrangement between the central government and the District Health Technical Team. The local councillors who can possibly articulate the gender health needs of the community do not have the powers to influence a change in budgeting guidelines. This brings to light the loopholes of participation that informs the Local Governments Act of the Republic of Uganda2. Discussion The priorities of the district health sector do not reflect the broad community-wide understanding and gendered nature of health needs. District health sector priorities primarily focus on common disease infections such malaria, HIV/AIDS and tuberculosis, without emphasis on the socio-economic constraints of women and men. Therefore, the health needs of women as compared to men are narrowly defined in the local health sector because the identification of such needs is limited to measures of ill health (incidence and prevalence of disease) in the community. Although such ill health concerns are important, there is increasing recognition that overreliance on such measures in priority-setting can be counterproductive8. This is because ill-health concerns solely focus on the physiological aspects of women's compared to men's needs. As such, there is need to move towards a more holistic view that the communities take in terms of health, by taking into account the gendered nature of ill-health concerns and social-economic needs, while budgeting for health in local governments. However, there are limitations associated with this complete understanding of health needs as perceived by women and men in the community. Information about health needs can be heterogeneous depending on the social-cultural relations in the community, far harder to gather, analyse and present. The form in which health care needs are perceived may also differ between those who see needs in medical terms, those who see them in health service terms, and those who see them in broader social-economic terms8. But the two-fold framework for the gendered understanding of health needs is more holistic than the disease-based approach because it captures all the different aspects of health care. Conclusion and recommendations In Mpigi district the definition of health needs in the community differs from the priorities of the district health sector. Women's and men's responses reveal that health needs range from health care concerns about household welfare to deficiencies in the local health system. Conversely, the understanding of health needs in the district health sector is largely based on ill-health indicators. Therefore, in designing local health budgets, local governments need to move towards a holistic definition of health needs that encompasses not only common disease infections, but also the socio-economic constraints that impact on the well-being of women and men. As such, the two-fold framework for the gendered categorisation of health needs is essential in aligning local health care budgeting to the differing priorities of women and men. The two-fold gendered framework combines both disease-based health needs and socio-economic needs of women as compared to men. To apply the two-fold gendered framework, local government budgeting should primarily be concerned with collecting gender disaggregated information for a complete understanding of health needs: the effects of common disease infections and socio-economic hardships that impact on the well-being of women and men. Baseline information for budgeting should also include important issues such as the daily household budget expenditure on health care for women compared to men, sharing and distribution of income savings among household members and how unpaid health care work subsidises local government spending. The information collected can be used to develop a Local Governments Gender Budgeting Framework. The framework should: 1) integrate gender disaggregated data on the prevalence of disease (BoD) and the socio-economic hardships of women and men in health care provision; 2) revisit planning and local governments budgeting policies against actual allocations and health programmes; 3) provide tools for analysing the gender implications of the prioritised expenditure; and 4) provide information on monitoring progress towards increased gender responsive budgeting. Before being made functional, the two-fold gendered framework should have a zero measurement to evaluate the pros and corns of its implementation at both higher and lower local governments. By giving evaluation its proper place in developing the framework, a process of social learning will be attained. Automatic feedback will be generated on every element of the framework from all local governments (preferably with regard to the cycle of planning and local government budgeting). Acknowledgements The research documented in this paper came to fruition thanks to the support of many people. Women and men in Mpigi district shared their ideas, points of view, dreams, concerns and worries with me while talking about their way of life. I acknowledge their contributions to the research, their patience, hospitality and good company. Special thanks go to my graduate supervisor, Dr. Josephine Ahikire of Makerere University Kampala, who provided spirited input and critical feedback on my graduate thesis from which this paper was developed. Financial support for the research was provided by the Belgian Technical Cooperation in Kampala (BTC), thank you for being Uganda's development partners. Lastly, I acknowledge the technical capacity offered by the Regional Network on Equity in Health, HEPS-Uganda and Makerere University School of Public Health, in writing and publishing this paper. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09053t2.jpg] [hs09053t1.jpg] |
| |||||||||

{kind=link}
{kind=link}