 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 4, December, 2009, pp. 247-253 Factors influencing time to diagnosis of childhood cancer in Ibadan, Nigeria *James BO1, Ajayi SO2, Ogun OA3, Oladokun RE1 1. Department of Paediatrics, College of Medicine, University of Ibadan Code Number: hs09060 Abstract Background: Early diagnosis of cancer allows an opportunity for timely treatment while disease burden is in its
earliest stages. Unfortunately, late presentation and delayed diagnosis of childhood cancers remains a problem in
developing countries. Introduction During the past three decades, survival of childhood cancer has markedly improved particularly when appropriate protocols are used. In developed countries, the 5-year survival rate increased from 30% for children treated in the 1960s to over 70% for children treated in the 1990s.1-3 In low income countries however, cure rates are at least 20-30% lower than in high income countries4, reflecting an advanced stage of disease at diagnosis (usually due to delayed diagnosis) and higher rates of fatal toxicity and abandonment of therapy.5 Similarly in Nigeria, childhood cancer survival is poor and frequently characterized by late presentation. 6,7 Early diagnosis of cancer is a fundamental goal in oncology because it allows an opportunity for timely treatment while disease burden is in its earliest stages. Consequently, prognosis may improve, and a cure can be attained with minimal side or late effects.8 Various researchers have carried out studies to find out the time to diagnosis of a variety of childhood cancers and the factors associated with delayed diagnosis. Some researchers have focussed on the time between a patient's first symptom recognition to a diagnosis of cancer. This time period, called diagnosis delay has also been designated as pre-diagnosis symptomatic interval, time to diagnosis, lag time or wait time by different authors.8 Others have made a distinction between patient and physician delays.9,10 The former was defined as the length of time between the onset of signs and symptoms and the patient's first visit to the health care system, whereas the length of delay between the first health care visit and the diagnosis was designated physician delay. The latter definition of physician delay may however not be strictly applicable in Nigeria where for a variety of social and cultural reasons, patients after entering the health care system may leave it for alternative medical practices for no fault of the physician. A study in Nigeria is particularly important because of existing socio-cultural factors different from those in countries where previous studies have carried out. The objectives of this study were to describe the clinical stages of the tumours at diagnosis, the pre-diagnostic symptomatic intervals and the factors influencing these time intervals or diagnosis delays in cases of childhood cancer seen at the University College Hospital, Ibadan, Nigeria Materials and Methods This study involved all cases of childhood cancer seen between March 2006 and August 2008 at the Department of Paediatrics of the University College Hospital, Ibadan, Nigeria. Information was obtained from the patients' clinical notes and included socio-demographic variables, stage of the cancer, duration of illness at diagnosis and other health seeking activities embarked upon. The time between onset of symptoms and diagnosis was divided into two namely parent delay and health system delay. Parent delay also called patient delay by other authors was the interval between onset of symptoms and the first visit to the health care system. We used the term health system delay to represent what other authors called physician delay i.e. the interval between the first contact with the health care system and diagnosis. For the purpose of uniformity and ease of comparability, clinical staging was done using the SEER (Surveillance, Epidemiology and End Results)11 clinical staging as follows: Localized tumour: A malignancy limited to organ of origin with no spread beyond organ of origin
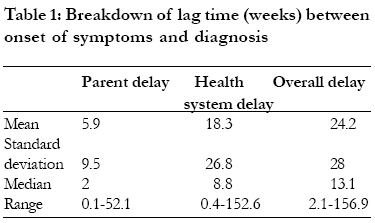
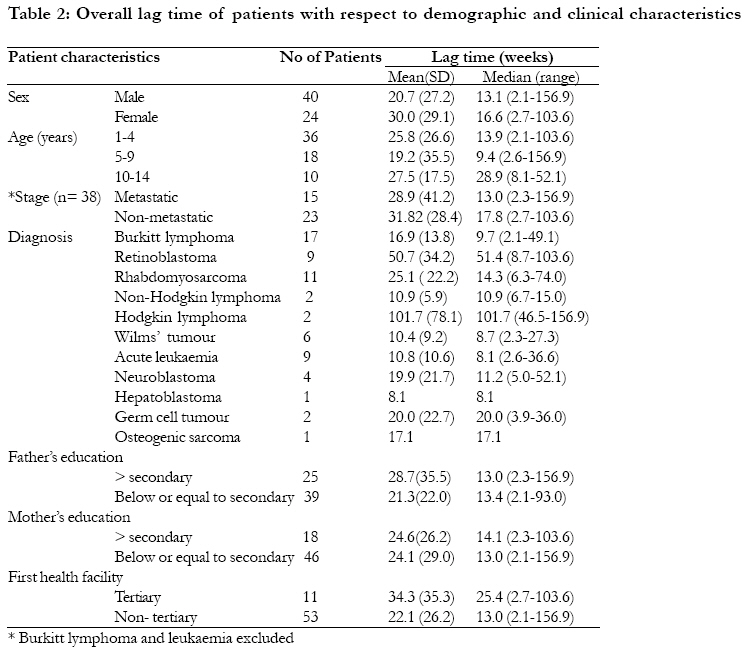
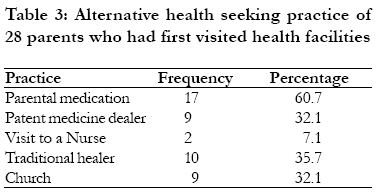
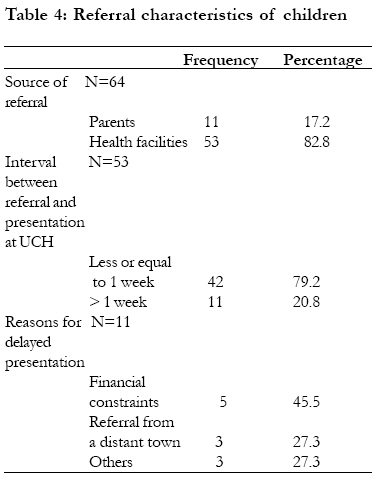
In this study, staging was done using at least clinical signs and diagnostic imaging (ultrasonography), in all patients, and when necessary surgery and cytology of bone marrow aspirate. Data were recorded onto a case record form, entered into a computer and analysed using SPSS version 15.0. Frequency distributions of categorical variables were computed and continuous variables described with parametric tests. Since time lag was found to be skewed, median figures and ranges were presented. For the same reason, Mann-Whitney and Kruskal-Wallis tests, which are non- parametric statistics, were used in comparing time lag between different categorical variables and Wilcoxon Signed Ranks test in comparing paired time lag between parent delay and health facility delay. Statistical significance was set at p < 0.05. Results A total of 64 children were studied comprising 40 males and 24 females giving a male: female ratio of 1.7:1. Their ages ranged from 1 to 14 years with a mean (standard deviation) of 5.3 (3.3) years. Based on SEER staging, disease was localized in 14 (21.9%) patients, regionalized in 19 (29.7.0%), and metastatic in 31 (48.4%) of the children. Median overall lag time was 13.1 weeks (2.1-156.9 wk), median parent delay was 2 weeks (0.1-52.1wk) and median health system delay was 8.8 weeks (0.4-152.6 wk)[ table 1]. Paired comparison of the parent delay and `health system' delay revealed the latter to be significantly longer (Wilcoxon Signed Ranks tests, p < 0.001). The lag time of patients with respect to demographic and clinical characteristics is shown in table 2. A significant difference in lag time was found among tumours types with the shortest lag times in acute leukaemia and Wilms' tumour and the longest in Hodgkin lymphoma (Kruskal-Wallis test, p 0.034). In analyzing the effect of the presence of metastatic disease at diagnosis on lag time, cases of Leukaemia and Burkitt lymphoma were excluded. This is because, cases of leukaemia are assumed metastatic at diagnosis and Burkitt lymphoma being multi-focal in nature may present with disease at multiple sites right from the onset ( i.e. time zero). There was no association between overall lag time and presence of metastatic disease (Mann-Whitney U, p=0.296). Although lag time was longer in female than in male children, this difference did not reach statistical significance (Mann-Whitney U, p = 0.185). Although, the lag time was least for the 5-9 year age group and longest for the 10-14 year age group, there was no significant difference in lag time across the different age groups (Kruskal-Wallis test p = 0.106). There was also no significant difference in lag time between children whose parents had post secondary education and those with lower educational levels (Mann-Whitney U , p= 0.496 for paternal educational level, p= 0.870 for maternal educational level). In addition, no significant difference was observed in the lag time between patients whose first health facility visit was tertiary and those who visited lower level facilities (Mann-Whitney U, p=0.455). Duration of illness when patients visited tertiary health facilities was significantly longer than duration of the illness when they visited non-tertiary facilities (Mann-Whitney U, p=0.005). For most parents, 48 (75.0%), the first port of call for medical attention was a health facility; 13 (20.3%) administered drugs bought over the counter for their children and 1(1.6%) each consulted a patent medicine dealer, used herbal preparation and took the child to a church respectively. Among the 48 patients who visited health facilities first, 28 subsequently engaged in other health seeking behaviours as shown in table 3. Among those who sought alternative sources 14 (50%) of 28 had metastatic disease at diagnosis compared to 8 (40%) of 20 who only attended health facilities. Although there was a greater tendency for those who sough health care outside health facilities to present with metastatic disease, this did not reach statistical significance (Fisher's exact significance p = 0.565). When eventually each of the 64 patients presented at a health facility, 11 (17.2%) first presented to tertiary health facilities, 42 (65.6%) to secondary health facilities and 11 (17.2%) to primary health centres. Seven children presented first at the UCH out of which 6 followed through to diagnosis and management whilst 1 was scheduled for surgery but defaulted for 67weeks before presenting again at the hospital. Of the remaining 57 children for whom the first health facility visited were other health facilities aside from UCH, 17 (29.8%) were referred to UCH within 2 weeks of presentation. The others were managed in the health facilities for periods ranging from 1 day to 156 weeks with a median of 6.0 weeks and mode of 8 weeks; they were either subsequently referred after a long time of treatment or taken away by parents due to unsatisfactory response to treatment. Regarding sources of referral, eleven parents brought their children to the University College Hospital and the remaining children were referred by health facilities; details shown in table 4. Discussion Late presentation has been reported to be associated with an increased risk of mortality in childhood cancer12. Our finding of metastatic or diffuse disease occurring in majority of children at diagnosis is in keeping with previous reports in our country.13 This may ultimately result in poor prognosis in such cases. It is therefore important to find out factors that influence the time of presentation of children with cancer in order to design strategies aimed at facilitating early diagnosis. Diagnostic delays in our study population were much longer than reported by Haimi et al in Israel.10 While the latter reported median parent's delay of 1 week, doctor's delay of 4 weeks and overall delay of 7 weeks, the corresponding values in our study were 2, 8.8 and 13.1 weeks respectively. The delays in our patients appear to be twice as long as those in Israel. This may be due to differences in the health seeking attitudes which may in turn be related to socio-cultural factors and the challenges of access to health services in a developing country like Nigeria. The health service delay in diagnosis (interval between first contact with the health care system and diagnosis) was significantly longer than the parent delay in our study in keeping with findings by Haimi et al.10 However, unlike in the latter study, we have refrained from calling it doctor's delay since in our setting; multiple factors including parental decisions and not exclusively the doctor contribute to delay in diagnosis after the first contact with the health services. Important factors include delayed referral of children to centres where appropriate management can be provided. These patients were kept for a median of 6.0 weeks but in an extreme case for three years being managed for a wrong diagnosis before referral. This contrasts with a country like Canada where half of children under 15 years of age wait less than one month from the onset of symptoms to their first anti-cancer therapy .9 Parental factors contributing to delayed diagnosis after contact with the health system include seeking health care through alternative means such as "parental self medication", patent medicine dealers, traditional healers and churches. Other factors that contributed to the health system delay were financial constraints faced by the parents and the need to travel to a referral centre that is far from the city of residence of the family. The habit of seeking alternate sources of care after initial contact with the health care system suggests a lack of confidence in the system. It is also a reflection of the socio-cultural factors influencing health seeking behaviour in the country. Unfortunately, higher educational level of parents did not seem to confer any advantage with regard to diagnosis delay in our study. Persons of higher educational levels in Nigeria, tend to patronize private hospitals and deliberately avoid government owned specialist centres because of the series of diagnostic tests often requested and the processes involved in seeing a doctor which are often longer than those in private hospitals. Consequently, persons with higher educational levels often suffer delayed diagnosis despite being frequently more economically empowered. Our finding of significant difference in lag time with regard to tumour types confirms previous observations by Pollock et al14 and Haimi et al.10 Apart from hepatoblastoma in which only one case was seen, the shortest delays in diagnosis in our patients were seen in acute leukaemia and Wilms' tumour with median times of 8.1 and 8.7 weeks respectively. This is in keeping with findings by Fajardo-Gutierrez et al 15 who also observed that, leukaemias had the shortest time to diagnosis in Mexican children but with a median time of 1 month. Further corroborating our findings, Haimi et al 10 observed the shortest delays in children with kidney tumours in Israel but with a median time of 2.5weeks. In our patients, acute leukaemia and Wilms' tumour which had the shortest times to diagnosis were closely followed by Burkitt lymphoma (median time 9.7 weeks). The longest delays in our patients were in retinoblastoma and Hodgkin lymphoma with median times of 51 weeks and 101 weeks respectively. This is also in keeping with findings by Fajardo-Gutierrez et al 15 in Mexican children in whom Hodgkin disease and retinoblastoma had the longest time to diagnosis but with a median time of 5 months. With leukaemia having the least delay and Hodgkin disease and retinoblastoma having the longest delays our finding are also similar to those in Mexican children. However, the median times in Nigerian children seem to be at least twice as much as those in Mexican children just as it was in comparison to children in Israel. The delay in the diagnosis of Hodgkin lymphoma in our patients is probably due the indolent course of some forms of Hodgkin lymphoma; Miettinen reported an 80 percent 10 year survival for untreated nodular lymphocyte predominant Hodgkin lymphoma.16 In addition, one of our two patients spent about 3 years in the source of referral receiving various treatments for infections probably due to the clinical similarity between Hodgkin lymphoma and infections in the tropics like tuberculosis. The late presentation of tumours is a cause for concern and particularly so for retinoblastoma considering the loss of vision that may occur even if the patient gets cured eventually. A delay in the diagnosis of retinoblastoma is not uncommon particularly in unilateral cases presenting with subtle signs like strabismus or masquerading features such as hyphaema, uveitis or secondary glaucoma 17, 18. In a study by Wirix et al in Belgium, a child was found to have been followed up for strabismus for four years without any proper fundus examination, in whom a diagnosis of retinoblastoma was later made.17 The presence of leukocoria itself, though present in up to 60% of patients, denotes a large tumour and may not even be noticed by the parents as it depends on the direction of light entering the eye to produce the characteristic cat's eye reflex.17 Patient's presenting with a squint particularly suffer longer delays before diagnosis as compared with other symptoms.17 This therefore underpins the need to emphasize to parents, physicians and ophthalmologists alike, the need to promptly and exhaustively evaluate any child presenting with a squint to exclude an occult intraocular tumour. Some researchers have reported an increase lag time to diagnosis of cancers with increasing age.14,19 Although our study similarly observed the longest delay in the 10-14 year age group, a trend of consistent increase from infancy upwards was not noted. The shortest lag time in our study was in the 5-9 year age group probably due to the high proportion of Burkitt Lymphoma which is highly proliferative and peaks at that age in our environment20. We also observed no difference in lag time between male and female in keeping inconsistent gender differences observed in various studies. In a review by Dang-Tan, only 2 out of 9 studies observed significant differences in diagnosis delay between male and female patients.8 We found no difference in lag time between cancers diagnosed at different stages in keeping with findings by Saha et al.19 On the contrary, some other researchers have observed an association between shorter time at presentation and improved stage at diagnosis.21 The relationship between diagnosis delays and disease stage is complex. It is rational to think that longer delays would lead patients to be diagnosed at a more advanced stage of the disease. However, more aggressive, fast-growing tumours may lead parents to seek medical attention for their child early exemplified by the findings of Halperin and Friedman who observed that meduloblastoma patients with advanced stage exhibited shorter lag times compared with early stage disease patients.22 Therefore aggressiveness of disease and the attendant severity of symptoms likely play a role in the relationship between diagnosis delay and cancer stage. Haimi and colleagues observed that lag times were shorter for children first examined by Paediatricians in comparison to family physicians and other specialists. 10 We did not examine the lag time in relation to specialists first seen by the patient but rather by the level of health care facility first visited by the patient. We expected that children seen at tertiary centres are more likely to be attended to by Paediatricians and therefore be diagnosed earlier. We observed no difference in lag time for patients first seen at a tertiary health facility compared to those first seen at lower level facilities. This however was not a surprise since the duration of illness at presentation in tertiary centres was significantly longer than those at presentation at lower level health facilities. It seems therefore that parents take their children directly to tertiary centres when the illness has been protracted and the disease probably more advanced. Conclusion Diagnosis delay of childhood cancer in Ibadan, Nigeria, tends to be longer compared to more developed countries. Education of physicians on the need for a high index of suspicion of cancer and prompt investigation of suspicious clinical features for early referral is strongly indicated. In our study, following referral (although late in most instances), most parents immediately complied and took their children to the referral centres. This suggests that if children are referred early, parents may also comply, resulting in early diagnosis. Education of parents on the importance of early presentation at health facilities and continuing within the system until a diagnosis is established and management started is necessary. This may be further enhanced by improved operation of the newly instituted National Health Insurance Scheme in the country.23 This is a scheme whereby an agreed amount of a worker's salary is deducted from source on a monthly basis and paid to enable the insured and dependants access health care without having to pay at the point of need. Some of the objectives of the Scheme are to ensure that every Nigerian has access to good health care services, to protect families from the financial hardship of huge medical bills and to ensure equitable distribution of health care costs among different income groups. Successful shortening of the diagnosis period may ultimately improve prognosis of childhood cancer in Nigeria. Acknowledgement Our acknowledgements go to the entire consultant staff and resident doctors in the department of Paediatrics who have contributed to the management of the patients and proper documentation of clinical records of patients. References 1. Gatta G, Capocaccia R, Coleman MP, Reiss LAG, Berrino F. Childhood cancer survival in Europe and the United States. Cancer 2002:95:1767-1772. 2. Reaman GH. Pediatric oncology: current views and outcomes. Pediatr Clin N Am 2002; 49:1305-1318. 3. Coebergh JW, Capocaccia R, Gatta G, Magnanin C, Stiller C A. Childhood cancer survival in Europe 1978-1992: the EUROCARE study. Eur J Cancer 2001; 37:671-672. 4. Bonilla M, Moreno N, Marina N, et al. Acute lymphoblastic leukemia in a developing country: Preliminary results of a nonrandomized clinical trial in El Salvador. J Pediatr Hematol Oncol 2000; 22:495501. 5. Howard SC, Pedrosa M, Lins M, et al. Establishment of a pediatric oncology program and outcomes of childhood acute lymphoblastic leukemia in a resource-poor area. JAMA 2004; 291:24712475. 6. Aikhionbare H A, Yakubu A M, Afolayan A E. Neuroblastoma, an under-diagnosed tumour: a seven year experience in Zaria. Ann Trop Paediatr 1988;8:149-152. 7. Familusi J B, Aderele W I, Williams O H. Features of neuroblastoma in African children. East Afr Med J 1979; 55:182-90. 8. Dang-Tan T, Franco E L. Diagnosis Delays in Childhood Cancer: Review. Cancer 2007; 110:70313. 9. Klein-Geltink JE, Pogany LM, Barr RD, Greenberg ML, Mery LS. Waiting times for cancer care in Canadian children: impact of 3. Kumar S, Sarr MG, Kamth PS. Mesenteric venous thrombosis: Review Article. N Engl J Med. 2001; 345 (23) : 1683 1688.4. Acosta S, Alhadad A, Svensson P, Ekberg O. Epidemiology, risk and prognostic factors in mesenteric venous thrombosis. Br J Surg. 2008; 95:1245-1251 5. Schoots IG, Koffeman GI, Legemate DA, et al. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. Jan 2004;91(1):17 PubMed -27. [Medline]. 6. Abdu RA, Zakhour BJ, Dallis DJ. Mesenteric venous thrombosis -1911 to 1984. Surgery. Apr 1987; 101 (4): 383 PubMed -8. [Medline]. 7. Kaleya RN, Boley SJ. Mesenteric venous thrombosis. In: Najarian JS Delaney JP, eds. Progress in gastro intestinal surgery. Chicago: year Book Medical. 1989 : 417 25. 8. Rhee RY, Gloviczki P. Mesenteric venous thrombosis. Surg Clin North Am. Apr 1997;77 (2):327-38. [Medline]. 9. Haward TR, Green D, Bergan JJ, Rizoo RJ, Yao JS. Mesenteric thrombosis. J Vasc surg. 1989; 9: 328-33 10. Hassan HA, Raufman JP. Mesenteric venous thrombosis. South Med J. Jun 1999; 92 (6): 558 PubMed 62. 11. Tomchik FS, Wittenberg J, Ottinger LW. The roentgenographic spectrum of bowel infarction. Radiology 1970; 96: 249-60 PubMed . 12. Matos C, Van Gansbeke D, Zalcman M, et al. Mesenteric vein thrombosis: early CT and US diagnosis and conservative management. Gastrointest Radiol. 1986; 11 (4) : 322-5. [Medline]. 13. Bradbury MS,Kavanagh PV, Bechtold RE, et al. Mesenteric venous thrombosis: diagnosis and noninvasive imaging. Radiographics. May-Jun 2002; 22(3): 527-41. [Medline]. 14. Hotoleneau C, Andrercou O, Andrercou A. Mesentric Venous Thrombosis with bowel infarction and hyperhomocysteinemia. Vascular and endovascular surgery 2008;42 (5): 477-481 15. Lopera JE, Correa G, Brazzini A, et al. Percutaneous transhepatic treatment of symptomatic mesenteric venous thrombosis. J Vasc Surg. Nov 2002; 36 (5) : PubMed 1058-61. [Medline]. 16. Takahashi N, Kuroki K, Yanaga K. Percutaneous transhepatic mechanical thrombectomy for acute mesenteric venous thrombosis. J Endovasc Ther. Aug 2005;12(4):508 PubMed -11. [Medline]. 17. Cho YP, Jung SM, Han MS, et al. Role of diagnostic laparoscopy in managing acute mesenteric venous thrombosis. Surg Laparosc Endosc Percutan Tech. Jun 2003;13 (3):215-7. [Medline]. 18. Khodadadi J, Rozencwajg J, Nacasch N, et al. Mesenteric vein thrombosis. The importance of a second-look operation. Arch Surg. Mar 1980; 115(3): 315 PubMed -7. [Medline]. 19. Eldrup-Jorgensen J, Hawkins RE, Bredenberg CE. Abdominal vascular catastrophes. Surg Clinic North Am. Dec 1997; 77 (6): 1305 PubMed -20. [Medline]. 20. Roman RJ, Loeb PM. Massive colonic dilatation as initial presentation of mesenteric vein thrombosis. Dig Dis Sci. Mar 1987; 32 (3): 323-6. [Medline]. 21. Nishida S, Levi D, Kato T, et al. Ninety-five cases of intestinal transplantation at the University of Miami. J Gastrointest Surg. Mar-Apr 2002; 6(2): 233 PubMed -9. [Medline]. Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09060t4.jpg] [hs09060t1.jpg] [hs09060t2.jpg] [hs09060t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}