 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 4, December, 2009, pp. 258-263 Zero prevalence of parasites associated with oral lesions of HIV infected and AIDS patients in South Western Uganda *Agwu E1, Ihongbe JC2, Pazos V1, Tirwomwe JF3 1. Department of Medical Microbiology and Parasitology, School of Health Sciences, Kampala International
University, Uganda Code Number: hs09062 Abstract Background: Despite paucity of information regarding oral lesions with parasitic etiology, parasitic diseases continue to
be problematic among impoverished and immunocompromised individuals in developing countries. Key words: Parasites, Oral lesions, HIV/AIDS, Uganda. Introduction Human immunodeficiency virus (HIV) infection is a major global health problem. By the end of 2007, there were around 33 million HIV-infected people in the world and more than 67% of the HIV-infected live in the developing countries1. HIV-related oral lesions are frequent and often an early finding in HIV infection. They affect the quality of life of the patient, are useful markers of disease progression and immunosuppression and their importance has been demonstrated in many studies 2, 3. The origin of oral infection may be exogenous (from pathogenic organisms) or endogenous (from oral flora). Any adverse changes resulting from immunosuppression may predispose to oral microbial infections 4. Oral lesions with different microbial etiology have been well documented in HIV infected and AIDS patients. Candida albicans is the predominant yeast isolated from oral lesions followed (in descending order of virulence) by: C. glabrata, C. tropicalis, C. parapsilosis, C. pseudotropicalis, C. krusei and C. guilliermondi 5. C. dubliniensis is a newly discovered novel species, and its virulence potential is much like that of C. albicans due to their close genomic relatedness 6. Despite the existing diversity among the non-albicans species 7, it is the general belief that they are of low virulence and that disease manifestation is determined by the health of the host. Tuberculosis and poverty are among the predisposing factors of cancrum oris (noma), an infectious disease resulting in the destruction of the oro-facial soft and hard tissues, affecting predominantly children aged 2-16 years in sub-Saharan Africa where the estimated frequency varies from one to seven cases per 1000 children 8, 9. Staphylococcus aureus is a common cause of osteomyelitis of the jaws, a relatively rare condition, which may be precipitated by immunosuppression 10, 11. Oro-facial lesions of secondary 12 and tertiary syphilis 13 have been described in HIV positive subjects. Oral Hairy Leukoplakia (OHL) has since been shown to be associated with a localized Epstein-Barr virus (EBV) infection and occurs most commonly in individuals whose CD4 lymphocyte count is less than 200 per millimeter cube 14. The incidence of Herpes Simplex Virus-1 and II oral ulceration is reported to be between 0.69% in HIV positive patients and lesions can be more severe and prolonged 15. There have been recent reports of oral ulcers co-infected by Herpes Simplex Virus-1 and II and Cytomegalo virus 16, though the pathogenesis of such lesions remains unknown. Recurrent oral varicella zoster virus (VZV) infection, seem to be more severe and prolonged in HIV positive patients and are reported to have an incidence seven times greater in HIV positive patients than in the general population 17. Oral warts due to Human papilloma virus (HPV) have dramatically increased in the HAART era 18, 19. Parasitic diseases are widely distributed throughout the world and they continue to be problematic in developed and less developed countries. The presence of parasitic diseases among impoverished and especially among immunocompromised individuals is now being reported. The disease-causing parasites are typically obligate organisms, dependent on vertebrate hosts, arthropod hosts or both for survival. The parasites may produce serious infections and, occasionally, the death of their hosts 20. Reports of oral lesions with parasitic etiology especially from developing countries are very rare. Oral myiasis, also known as dental and gingival myiasis, is a larval infection of tissues of the oral cavity 21. Oral myiasis is rare, and most cases have been reported from developing countries, particularly in Asia 22. Oral manifestations of teniasis which present as a red, edematous, hyperplastic mucositis, accompanied by gingival bleeding and pain in a patient diagnosed with T. saginata have been reported 23, 24. The larval form of echinococcosis causing hydatid cysts of the oral structures have been reported in six human cases 25. Human infections caused by nematodes are most prevalent in children 26. Oral cases of Gongylonema pulchrum, a small roundworm generally found in the digestive tract of domesticated farm animals has been reported in humans according to the review of Thomas and Francisco 27. Yilmaz et al., 28 recently reported oral Ascariasis in a man undergoing final stage of anesthesia in Turkey. Despite the documented literature regarding prevalence, medical importance, knowledge of etiology and improved management protocol of oral lesions, it still constitutes a major health concern especially in HIV infected and AIDS patients. Thus, oral lesions with different microbial etiology remain big global health problem particularly in HIV infected and AIDS patients living in Africa. We are not aware of any similar study documenting the role of parasites in the induction, progression or rebound of oral lesions in this region. This follow-up survey was therefore designed to determine the prevalence of parasites in the previously diagnosed and identified29 oral lesions of HIV infected and AIDS patients in south western Uganda. The ultimate goal of this study was to find out every remotely possible etiology of reported continued prevalence of oral lesions among people living with HIV in Uganda 29. This would assist in decisively suggesting improved treatment protocols, better surveillance and overall improvement in our current understanding regarding oral lesions in HIV/AIDS patients living in Uganda and Africa.
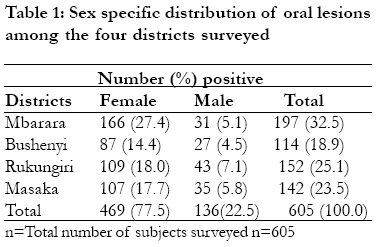
Materials and Methods Three centers of The AIDS Support Organization "TASO", located in four Districts of South Western Uganda namely: Masaka, Rukunguri, Bushenyi (Katungu, Motoma and Kigarama outreach centers) and Mbarara head office (including Ibwanda and Nyihanga outreach centers), were used for this investigation. The inclusion criterion for the selected 3 TASO centers located in the 4 South Western Uganda Districts surveyed was based on center participation in a previews study 29 of oral lesion prevalence in a similar cohort. The conditions for which patients were included in this study were that patients: must have tested positive to HIV using an Enzyme linked Immunosobent Assay (ELISA) and any other immuno-serological method; must have had his/her HIV/AIDS clinical staging done not earlier than one month prior to time of sample collection; must be a current TASO Client above 18 years of age and must have a lesion in the mouth clinically diagnosed by trained and calibrated oral clinicians29. Patients who were taking any anti-parasitic agents were excluded from the study. Six hundred and five samples (469 from females and 136 from males), were randomly collected from oral lesions of TASO HIV/AIDS patients in 4 selected Districts (Masaka-142, Rukungiri-152, Bushenyi with Mbarara-305) of South Western Uganda as indicated in Table 1. The sample collection for this survey lasted for six months between June and December 2006. Six hundred and five patients sampled was guided by the upper limit required to give 95% level of confidence at an expected prevalence of about 55% 29, using the precise prevalence formula: Sample size (N) = Z2P (100-P)/D2 (Epi-info version 3.2 data-base; 1995), where Z is a constant given as (1.96), P is expected prevalence (55%), and D is acceptable error (5%). The center selection criterion was participation in a previous study29, which revealed different kinds of oral manifestations of HIV/AIDS infection. Samples from patients who met the inclusion criterion described above but lacking any clinically diagnosable oral lesions served as control. Informed consent was sought and obtained from: Uganda National Council of Science and Technology, Kampala International University Research and Ethics Committee, The AIDS Support Organizations (TASO) at both local and National level and TASO clients (patients) through their informed consent. After visual inspection of the mouth to re-confirm presence of oral lesions and for visible segments or lava of parasites, duplicate swab samples were taken from identified oral lesions of patients with HIV and transported on sterile physiological saline 30 to the Laboratory Unit, Department of Medical Microbiology, Kampala International University, Western Campus, for analysis. At the Laboratory, direct microscopy of one of each duplicate oral swab, was undertaken to detect the presence of parasites. Saline and iodine wet preparations for parasitic analysis were made and examined using the procedure contained in our earlier report with slight modification to suit oral swab analysis 31. The backgrounds of wet smears were stained with eosin to increase visibility of trophozoites of parasites as reported by Cheesbrough 32. The second of each duplicate swab samples soaked in sterile physiological saline were then incubated for 18-24 hours at 37oC and examined after incubation. This step is important because protozoan parasites may be detected according to their different motility after incubation as recommended by Vrablic et al., 33. Smears were made from the oral swabs before and after incubation, fixed and stained with Giemsa- Romanosky stain following the steps we adopted in our earlier report 31. According to Vrablic et al., 33, Giemsa- Romanosky staining of oral swabs will characteristically stain the cell organelles of protozoans and other parasites enabling them to be quickly detected. It is technically simple, not time consuming, not laborious and of low cost making it optimal for the diagnosis of oral parasites. History of patients pre-exposure to other antimicrobial agents was taken after excluding those who were taking any anti-parasitic drugs. Results There were no ova, cyst, trophoziotes, lava or segment of parasites seen in the oral lesions identified among the studied population. Forty four (7.3%) patients were exposed to clotrimazole while 27 (4.5%) were exposed to Fluconazole. Patients were also exposed to: Ketoconazole 62 (10.2%), Nystatine 68 (11.2%) and Anti-retroviral Therapy 48 (7.9%). Table 1 shows the result of six hundred and five samples (469 from females and 136 from males) randomly collected from oral lesions of TASO HIV/AIDS patients in 4 selected Districts (Masaka-142, Rukungiri-152, Bushenyi with Mbarara-305) of South Western. Discussion Since all patients were not exposed to any form of parasitic drug, we could not ascertain the possible reasons for the complete absence of oral parasites among the studied population. The absence of any form of oral parasite from the observed lesions was amazing although promising in the eventual attempt to control microbes causing oral lesions among people living with HIV in Africa. To assess the role of antimicrobial agents in keeping the lesions free of parasites, patients who were taking any anti-parasitic agents were excluded from the study. Therefore complete absence of parasites from the oral lesions identified among the studied population may definitely not be due to the effect of anti-parasitic therapy. The population of TASO HIV/AIDS patients studied was mainly from Masaka, Rukunguri, Bushenyi (Katungu, Mitoma and Kigarama), Mbarara town (and Ibwanda and Nyihanga) towns and villages of South Western Uganda where there is inadequate public and personal hygiene, a factor reported by Despommier et al., 25, to predispose inhabitants to oral infection by maggots (Myiasis) transmitted by high fecundity flies. Halitosis and history of mouth-breathing were common mostly among the studied population of HIV patients with advanced oral Kaposi sarcoma. It was a surprise that we could not get any parasite from the studied population because mouth breathing and halitosis have been reported to predispose people to oral myiasis 34. Absence of any form of oral parasites in the oral mucosa of the studied immunocompromised population is contrary to the report of Wirtz and Azad 35 who noted that the human myiasis infestations commonly occur in the skin, lip, nose, mouth, ear, gastrointestinal tract, anal and sexual orifices and urinary passages. During direct microcopy of smears made from oral samples, we looked for suckers (and hooks) in the cephalic region and digitating walls in a ductal region to have indicated possible Cysticercosis but did not see any. There were no indication of Tenia species oncospheres or laval form present in oral tissues also to have indicated cysticercosis despite the prevailing poor personal and environmental hygienic conditions in the studied population and locations. Again, despite the presence of red, slightly edematous, hyperplastic mucositis and in selected cases, gingival bleeding and pain in the studied population suggesting possible presence of T. saginata as reported by Tzerbos 23, it was not clear why there was no oral Tenia species among the HIV/AIDS patients studied. We also inspected the tongues, lips and entire buccal mucosa which should be the most common location of discrete, firm, non-tender, nodules beneath intact mucosa highly diagnostic of Tenia cyst 24, but we found none. Uganda is a cattle, sheep and goat raising country and the majority of the studied population is involved in cattle, sheep and goat raising activity as their main occupation. In view of the fact that Shuker 25 reported the distribution of echinococcosis to be most prominent in sheep- and cattle-raising countries throughout the world and because some of the patients complained of difficulty with swallowing, speech and mastication; we therefore inspected the tongue and the mandible, buccal mucosa and the infratemporal fossa for circumscribed, soft or firm, elastic, fluctuant painless swellings diagnostic of hydatid cyst which may be unilocular (E. granulosus) or multilocular (Echinococcus multilocularis), but found none. All patients with oral cancer were referred to a Cancer center in Kampala, the capital city of Uganda for attention. We could not collect biopsy specimen from patients to screen for possible presence of a modified, viable nurse cells of Trichinella spiralis mainly because TASO discourages invasive procedures with their HIV/AIDS patients. This would have enabled us to investigate the report of Cheung et al., 36, who suggested that the finding of T. spiralis in the biopsy specimens from patients with oral squamous cell carcinoma lesions involving the tongue and the floor of the mouth raises the issue of carcinogenesis. Cheung et al., 36, therefore discussed the possibility of carcinogenesis and indicated there may be a relationship between trichinosis and oral squamous cell carcinoma. We expected Leishmania sp oral infection to be present especially among patients with Kaposi sarcoma because of the presence of sand-fly vectors in the studied locations. This is because; oral leishmaniasis and Kaposi's sarcoma were reported in an AIDS patient by Michiels el., 37. The patient was a 28-year-old man with a large ulcerated polypoid mass 3 cm in diameter involving the right palatine tonsil and soft palate. A biopsy of the tonsil produced a diagnosis of Kaposi's sarcoma in which the Leishman-Donovan bodies consistent with L. donovani were demonstrated. We therefore inspected the oral cavity for non-specific signs of oral leishmaniasis such as swollen, easily bleeding gingiva and lesions in the cheeks, uvula and palate which may be edematous, red and fissured. We stained the smears of the oral lesions expecting to see amastigotes but there was none. Since no biopsy specimen was collected, we could not make a definite conclusion regarding oral leishmaniasis co-infection with Kaposi sarcoma. Due to prevalence of poor oral hygiene and periodontal disease among the studied population, we also expected to see Trichomonas tenax probably in the oral mucosa or salivary gland 38, but found none. Some case reports have described the occurrence of T. tenax in salivary glands 39. This study has demonstrated that parasites are absent and therefore not involved as etiologic microbial agents of observed oral lesions associated with HIV infected and AIDS patients living in South Western Uganda.
Acknowledgement This study was supported in part by Kampala International University, Western Campus. We are grateful to management and staff of The AIDS Support Organization both at the Headquarters in Kampala and in the three centers located in South Western Uganda for their support. We also thank all TASO clients whose consent and participation made this investigation possible.
References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09062t1.jpg] |
| |||||||||

{kind=link}