 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 4, December, 2009, pp. 270-274 Ergogenic effect of varied doses of coffee-caffeine on maximal aerobic power of young African subjects *Lamina S1, Musa DI2 1. Department of Medical Rehabilitation, Faculty of Health Sciences and Technology, University of Nigeria, Enugu
Campus, Nigeria Code Number: hs09064 Abstract Background: Caffeine one of the readily available stimulants consumed daily by more than 80% of the
world's population, making it the most
widely consumed drug in history. The objective of this study was to determine the effects of
different doses (5, 10 &15 mg.kg-1) of caffeine per kilogram body weight on maximal aerobic power of normal young black
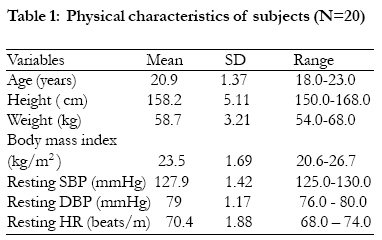
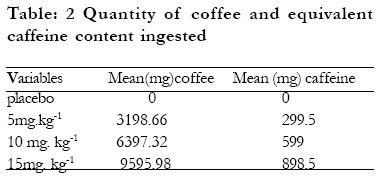
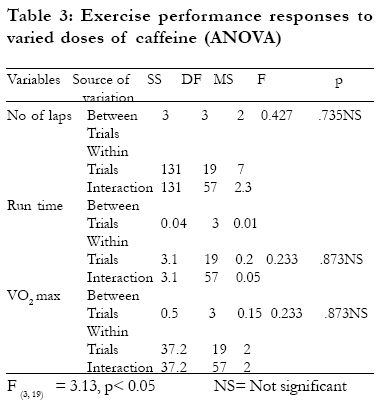
African (Nigerian) male adults. Key words: Caffeine; Ergogenic; Aerobic power. Introduction Caffeine (1,3,7- trimethyl-xanthine) is a methyl derivative of xanthine, one of the readily available stimulants consumed daily by more than 80% of the world's population, making it the most widely consumed drug in history. It is basically a Purina compound containing two condensed heterocyclic rings. It is a naturally occurring chemical found in over 60 different species of plant leaves, seeds and fruits. Specifically, much caffeine is found in coffee (Coffee arabica), tea, cola nuts (Cola acuminata). It is also found but in least quantity in cocoa (Theobroma cacao) 1-4. The ability of caffeine and other xanthines to aid sport performance is based on both the direct and indirect action on the heart or skeletal muscles, mediated through the nervous system, altered hormonal activities or shift in mobilization of substances (free fatty acid mobilization and glycogen sparing). There is also the possibility that the drug may alter the release, binding or activity of neurotransmitter in the brain, thereby affecting the perception of work intensity5. The controversy surrounding the use of caffeine as food beverages by laymen or use as an ergogenic aid by local, national and international athletes has drawn the attention of many scientists to research into the effects of this wonderful drug. Some Scientists2,6,7 view this aid as a justifiable extension of the body's natural capacities, while others8,9,10,11 see it as a dangerous and unethical violation of the code of fair play in sports. Due to the controversial reports of some scientists12,13,14,15 on the ergogenic effect of caffeine on performance, the International Olympic Committee (IOC) had a series of banned, un-banned and finally pegged the use of caffeine in sports competition to a tolerance limit of 12 ug,ml-1 urine2,16,17 Pasma, et al17 kovacs, et al18 and Bruce, et al19 reported that the doses below 6mg.kg-1 caffeine do not exceed the IOC urinary caffeine limit. However, in 2004 and to date, the World AntiDoping Agency (WADA) again removed caffeine from the list of banned substances20,21. Previous studies on the ergogenic effect of caffeine has been equivocal, mostly laboratory oriented and on white or other non African black subjects. However, reports have shown interracial and interpersonal differences in caffeine pharmacodynamics and pharmacokinetics6,22. Hence, the present study was therefore designed to investigate the ergogenic effect of varied doses of caffeine on black Africans (Nigerian subjects) using maximal aerobic field test (20 meter shuttle run test). MethodsSubjects Twenty male subjects of Bayero University Nigeria aged between 18-23 years participated. They were non athletes, non regular users of caffeine, non smokers and apparently healthy. Subjects were fully informed about the experimental procedure, risk and protocol. They were fully assured that the University Health Center will take care of any emergency that may occur. Subjects gave their informed consent in accordance with the American College of Sports Medicine guidelines (ACSM) 23, regarding the use of human subjects. Also, the ethical approval of the Faculty of Education, Bayero University, was given through the Ethical Committee. The subjects' physical (weight and height) characteristics were measured and recorded using standardized anthropometric protocol (International Society for the Advancement of Kinanthropometry (ISAK) 24. Design of the study Repeated measure design in which each subject served as his own control (Posttest placebo controlled design) was used. It is a double blind four randomized counter balanced cross over order. The ingestion of different doses (5, 10 & 15 mg.kg-1) of caffeine and placebo, coupled with exercise was separated by seven days' interval to avoid carry over effect25,26. Physiological measurement Subjects' systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate (HR) were monitored on the right arm as recommended by the manufacturer. The semi-automated BP monitor (Omron digital BP monitor model 11 EM-403c, Tokyo Japan) was used in the assessment of cardiovascular parameters. The measurement was done in the morning between 9am and 10 am each test day. Caffeine and placebo measurement The quantity of coffee to give the desired amount of caffeine needed (5, 10 and 15 mg.km-1) was measured using electronic weighing machine (Sartorous GMBH by Cottingen Germany). According to Eteng et al27 every 10.68 mg coffee (Capra Nescafe coffee) commonly found in Nigeria contains 1mg caffeine. Since pure caffeine was not readily available, Capra Nescafe coffee by Capra Nestle Company Abidjan, Cote De Voire was used. It is 100% pure instant soluble coffee. 0.1ml liquid food colour (coffee colour) by Ransons Exports, Faridaba Haryana India was used as Placebo. Both coffee doses and placebo were dissolved in 200 ml warm water22 and sweetened with artificial sweetener (Sweetex-saccharin by Crooks Healthcare Nottingham) as described by Engels et al28. Test Procedure The test was conducted between 8 am and 10 am, on arrival to the field (Bayero University Sports Complex) and following 10 minutes' rest in sitting position. Subjects SBP, DBP and HP were measured. Immediately subjects randomly ingested coffee doses (5, 10 and 15 mg kg-1) and placebo, subjects remain in sitting position for an hour (60 minutes). According to Robertson et al29. Caffeine peak plasma concentration are reached at approximately 60 minutes regardless of the dose. Immediately after 60 minutes of the post caffeine ingestion, subjects warmed up for about 5minutes (easy jogging and genera body stretching exercise) and got ready for the 20 meter shuttle run test (MST). The 20 MST was conducted on a leveled 20metre marked course with chalk at each end. The test was performed in accordance with one minute protocol using the Progressive Aerobic Cardiovascular Endurance Run (PACER) tape. The tape gave a 5 second count down (5, 4, 3, 2, 1) and instructed subjects to "begin". The 20 MST is a valid and reliable method of assessing cardiorespiratory fitness and endurance30 All the 20 participants (subjects) lined up behind the starting line. A partner was assigned to each subject to count the number of laps completed (a lag consisted of 20 meter distance). A the command "start"!, subjects ran in a straight line forth and back between restraining lines in accordance with the pace dictated by the audio signal emitted at a set intervals from the PACER tape. Subjects continued in this manner until they were unable to catch up with the sound of the beep for two consecutive times after which the test was terminated. The number of laps and time completed by each subject was recorded as his predicted cardiorespratory fitness score using the formula of Reunsbottom, Brewer and Williams31 as follows: VO2 max = 14.4 + 3.48 (minute completed) The total test duration was four weeks (once weekly) in a four randomized (5, 10, 15 mg.kg-1 and placebo) crossover counterbalanced manner. Statistical analysis Following data collection, the variables of interest were statistically analyzed. Mean and Standard Deviation were determined for all variables. Caffeine doses (5, 10 & 15 mg.kg-1) and placebo dose exercise performance (VO2 max, run time and number of laps) were statistically analyzed using repeated measured one way ANOVA. All statistical analysis was performed on an IBM compatible micro computer using the Statistical Package for the Social Science (SPSS) (Windows Version 16.0 Chicago IL USA). The probability level for all the above tests was set at 0.05 to indicate significance. Results Twenty males participated in this study. Subjects mean (SD) age, resting SBP, DBP and HR and were 20.9 (1.37) years, 127.85(1.42) mmHg, 79(1.17) mmHg and 70.4(1.88) beats/minute respectively. Detailed physical characteristics are depicted in table 1. Table 2 shows the mean amount of coffee and equivalent quantity of caffeine ingested. Five, 10 and 15mg/kg doses of coffee (caffeine) equivalent to 3,198.66mg (299.5mg), 6,397.32 (599mg) and 9595.98mg (898.5) respectively; while placebo was coffee and caffeine free. The result of the present study indicated no ergogenic effect of caffeine on short maximum endurance performance. Table 3 shows no significant effect of caffeine doses (5,10 & 15g/kg) over placebo on the number of exercise laps (F[3,19]=3.13, p=0.735); run time(F[3,19]=3.13, p=0.873) and VO2 max (F[3,19]=3.13, p=0.873). Discussion The purpose of the present study was to determine the effect of varied doses of caffeine on maximal aerobic power of normal young male African (Nigerian) adults. The study result showed no significant effect of caffeine doses over placebo dose on maximal aerobic power (VO2 max), run time and number of exercise laps. The non ergogenic effect of caffeine as reposted in the present study is in agreement with several studies32,33,34. However, other studies24,35 reported a contrary notion, that caffeine has ergogenic effect on endurance performance. between approximately 3199(300)mg to 9,596 (899)mg, which is equivalent to between 5 and 15 mg kg-1 body weight, constitute no ergogenic effect on subjects of black African (Nigerian) origin. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09064t2.jpg] [hs09064t1.jpg] [hs09064t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}