 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 4, December, 2009, pp. 279-283 Unmodified electroconvulsive therapy: changes in knowledge and attitudes of Nigerian medical students *James BO, Omoaregba OJ, Igberase OO, Olotu SO Department of Clinical Services, Federal Psychiatric Hospital, Benin City, Nigeria Code Number: hs09066 Abstract Background: The relevance of ECT as a treatment option for some psychiatric disorders continues to generate debate
in professional and lay circles. Scientific evidence as to the effectiveness of ECT (with anaesthesia) abounds. In some
developing countries, the process of change towards the full implementation and use of modified ECT has been slow. The
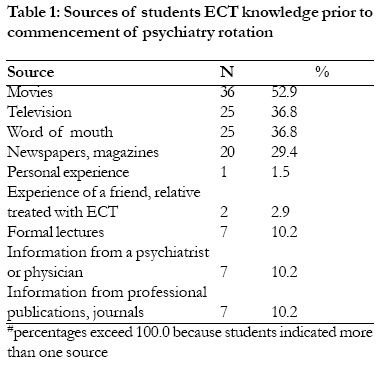
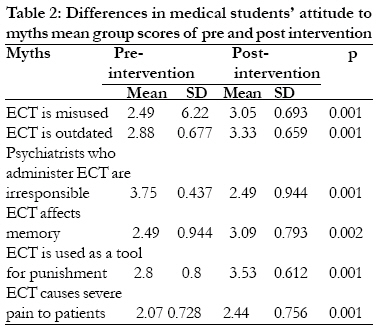
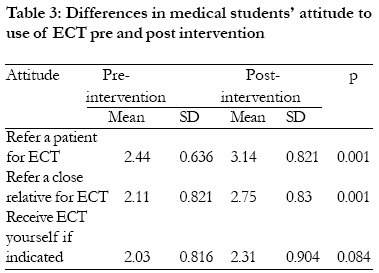
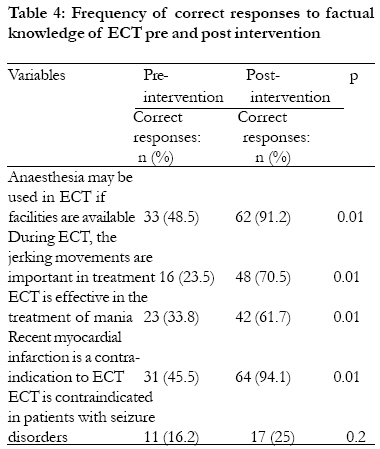
unmodified format is still used for largely economic reasons despite the ethical concerns it raises. Introduction Electroconvulsive therapy (ECT) involves the passage of an electrical stimulus to induce a central seizure with the aim of providing improvement in a patients' mental state under anaesthesia and muscle relaxation1. Among the physical therapies introduced before the advent of psychopharmacological agents in the 1950s, ECT still remains relevant in contemporary psychiatric care. Over the years, the knowledge that only the central seizure was necessary in providing symptom relief, that viewing the procedure administered without muscle relaxants and brief anaesthesia was barbaric, provoked patient anxiety and was associated with side effects (vertebral fractures, spontaneous seizures) led to the modification of the procedure with short acting anaesthesia and muscle relaxation. When administered by qualified personnel using strict guidelines, ECT is safe and effective, especially in situations where rapid treatment response is required2-5. The use of ECT in Nigeria dates back to the mid 1970s6, and unlike in developed countries, ECT is used in many centres in its unmodified or direct form6-9. An earlier attempt to introduce the modified form of ECT was unsuccessful due to the cost of the procedure to end-users and a dearth of qualified anaesthetists10. In recent times, there has been a push by professional groups to commence modified ECT in institutions that train psychiatry residents as a pre-requisite for accreditation or re-accreditation11. Though, a small minority of hospitals in the country now offer modified ECT, it remains to be seen if this format is routinely used. Since the last national audit on ECT use was reported 22 years ago7, new research to enumerate the current state of ECT practice is needed The World Health Organisation recommends that as much as possible. ECT be administered in its modified format12, and in developing countries where psychiatrists still use unmodified ECT, ethical concerns naturally dominate the discourse. Undoubtedly, unmodified ECT is fraught with unnecessary complications and in the presence of a better option it stands to reason that proposals to outlaw or discard unmodified ECT have basis. Proponents for the continued use of unmodified ECT argue that firstly, the magnitude of the side effects attributable from it as reported in Western literature may have been overstated in the light of recent evidence13-15. Ohaeri et al16 reported that in a small cohort of Nigerian patients, objective evidence for internal tissue damage from unmodified ECT using serial measurements of acute phase reactants (C-reactive protein, á-2-macroglobulin, ceruloplasmin, factor B, C-4 protein, C-3 protein, transferin and á-1-antitrypsin) was lacking, as these reactants did not change significantly during treatment with unmodified ECT. Similarly, Ikeji et al17 reported that in a sample of patients managed for schizophrenia mania and severe depression who had received unmodified ECT, objective memory assessments showed a return to pre-ECT scores within 4 weeks and these scores were comparable to controls (patients who did not receive ECT). In India, Tharyan and his colleagues18 conducted an 11 year retrospective review comparing 332 modified ECT treatments to 13,265 unmodified ECT treatments and observed that the incidence of cardiac arrests were higher with the modified type (0.9%) compared to the unmodified type (0.07%). However, the prevalence of 0.09% and 0.5% for fractures and myalgia respectively though lower than would have been expected is worrying. Secondly, most patients in developing countries cannot afford to pay for modified ECT13. Thirdly, the monopoly of scarce qualified anaesthetists by surgeons meant that modified ECT sessions cannot be planned effectively. Furthermore, in resource poor settings, psychiatrists faced with the ethical dilemma of using unmodified ECT in cases of patients with life threatening psychiatric emergency that will benefit from this form of ECT, may prefer it to no-ECT13,14. Thus, in Nigeria, it may be inferred that mental health professionals are faced with similar constraints and economic reasons may be the single most important factor as to why the continued use of unmodified ECT is still used among this group, even when they favour a rapid change to modified ECT19. Attitudes of patients, mental health professionals and lay persons toward ECT have yielded varying results. These variations often reflect the degree of knowledge of the procedure and type of specialty20,21. Psychiatrists generally hold positive views, intermediate are mental health nurses and least being medical students20. In Pakistan, it is believed that the unregulated use of ECT in its unmodified form may promote negative attitudes toward the procedure among patients and the general public22. Among medical students, negative views toward ECT became positive following a psychiatry clerkship23-26, suggesting that certain components of the clerkship program are important in changing attitudes. The purpose of this study was to determine whether a lecture on ECT, viewing the ECT procedure and following up a patient who had received ECT would effect a change in medical students' knowledge of and attitudes toward ECT. The authors hypothesized that pre-intervention knowledge and attitude scores would be poor, while though post-intervention knowledge scores should improve, their attitude scores should either worsen or remain the same because viewing the unmodified form of ECT (a component in our intervention) often promoted in the media and movies as barbaric and inhumane was to be viewed27. It would be interesting to see if arguments put forward for the use of unmodified ECT where the modified form is unavailable by specialists in resource poor settings would influence attitudes toward the procedure among future psychiatrists. Method Location The study was conducted at the Federal Neuropsychiatric Hospital, Uselu, Benin City, Nigeria. The hospital is a 256-bedded hospital, providing referral, in and out-patient services to a catchment area of over 6 million people in six neighbouring states. Electroconvulsive therapy is administered in its unmodified form at this hospital. Bilateral method of electrode placement is usually used with an Ectron Constant Current Series 5A ECT machine, with a dosage range of 50 to 700 millicoulombs at a constant current of 750 mA (Ectron Ltd, Letchworth, England). Subjects and study design Respondents were 5th year medical students at a private university in Benin City, Nigeria. Seventy two students on their clinical rotation in psychiatry at the Psychiatric Hospital, Benin City were approached after ethical approval for the study had been obtained from the hospitals' ethics committee. Sixty eight (94%) students agreed to participate in the study. All consenting students on the 2nd day of their 10-week posting received a 60 minute lecture on ECT which was not part of their teaching curriculum. The lecture was in a didactic format and comprised the history, indications, contraindications, complications and the current state of ECT practice in Nigeria. Just before the lecture was delivered, a questionnaire assessing the knowledge of and attitude towards ECT was administered. The students were asked for their sources of knowledge about ECT prior to commencement of their psychiatry rotation in the pre-intervention questionnaire. During the first week, respondents were divided into seven groups and viewed at least one live ECT session. Each group then followed up on a patient whose ECT session they had viewed and observed their clinical response over the next 4 weeks during teaching ward rounds. All patients were informed of the nature and purpose of the study prior to its onset and gave their consent. By the 5th week a post-intervention questionnaire was administered to evaluate knowledge and attitude changes toward unmodified ECT. Instrument The questionnaire on knowledge of and attitude toward ECT was adapted from a previously published work28. Attitudes to myths about ECT were assessed by six questions, each of which was rated on a Likert-type scale of 1-4 (1=strongly agree, 2=agree, 3=disagree, 4=strongly disagree). Five ECT knowledge questions were answered either yes, no or unsure. Lastly, three statements: how comfortable would you be (a) receiving ECT if you have depression not responding to medication (b) referring a close relative for ECT who has depression unresponsive to medication (c) referring a patient who has depression not responding to medication were asked. Responses to the last three statements were rated on a 1-4 scale (1=very uncomfortable, 2=uncomfortable, 3=comfortable, 4=very comfortable) Statistical analysis Data analysis was done using SPSS version 11.0 (SPSS Inc.). Above median group mean scores for the first six attitudes to myths statements indicated positive attitudes. The statement `psychiatrists who administer ECT are irresponsible' was reverse scored. Similarly, for the last three attitude statements above median group mean score represented positive attitudes. Differences in the mean group scores pre and post intervention were performed using the paired sample t-test. Differences in frequency of correct knowledge responses before and after the intervention were done using the chi-squared test. Statistical significance was set at 0.05 Results The mean age of the respondents was 23.5±1.8 years. Majority (57.4%) were females. The sources of knowledge of ECT prior to commencement of their psychiatry rotation are shown in Table 1. The movies (52.9%), television (36.8%) and print media (29.4%) were their commonest sources. The students' pre- and post-intervention attitude and knowledge scores are shown in Tables 2, 3 and 4. Mean post-test scores for the attitudes to myths about ECT statements were significantly higher than pre-test scores for all six statements. The percentage of correct responses to the knowledge questions was higher after the intervention, with statistically significant improvement in four of the five knowledge statements. For the last three attitude statements, all mean post-test scores were higher than mean pre-test scores but significant differences was noted in the two of the three statements. Discussion The major sources of information about ECT prior to commencement of their psychiatry rotation were movies and the print media. The study by Warnell et al28 on medical students in California, USA made similar observations. Expectedly the knowledge of ECT increased after our intervention. Baseline knowledge as evidenced by percentage of correct responses was poor and may be explained by the small fraction of students who had received correct information about ECT prior to their posting. Szuba et al23, Chanpattana et al29 and Warnell et al28 also observed the positive effect of a psychiatry clerkship or training on improving levels of knowledge about ECT among students. We observed that after the intervention, attitudes toward ECT improved significantly. Respondents were more comfortable referring persons for the procedure, though only a small increase was noted among students who were willing to receive ECT themselves. A 90minute lecture in Greece improved students attitudes toward ECT26, while a clerkship in the USA had similar effects28. It does appear that viewing the unmodified form of ECT did not adversely affect the students' attitudes. Perhaps, one component of our intervention - following up on the clinical outcomes of patients who had received ECT, had a profound effect on changing their attitudes. Taking a closer look, though a significant change in attitude concerning the statement `ECT causes severe pain to patients' was observed, post intervention attitude scores were still negative and was evidenced by their below median scores. This reflects the attitudes of most professionals that the procedure is barbaric with reactions to it being often emotionally charged14. It will be interesting to see what recipients (patients) of unmodified ECT feel about the procedure and contrast it with the views of professionals. Similarly, though the medical students were more comfortable referring a patient for the procedure following our intervention, perhaps more reflective of true attitudinal change is the likelihood of the medical students to refer close relatives or to receive the procedure themselves when indicated. We observed that attitudinal change concerning the statement `would you refer a close relative' was positive and significant; however this was just above median. Post intervention score for the statement `would you receive ECT if indicated' was below median indicating reluctance by our respondents to receive the procedure even after observing the beneficial effects in patients they followed up. Our study has some implications; firstly, our intervention had a significant impact on improving knowledge of respondents about ECT, secondly it helped changed attitude to myth generated in the media about the procedure. Thirdly, viewing the unmodified form of ECT and observing the beneficial effects in patients did not improve their acceptability of the procedure. Study limitations This study had some limitations. Ideally, we should have assessed in a true experimental design the effects of the individual components of our intervention. However in real situations interventions during clerkships or clinical rotations usually incorporate more than one factor28,29. Other limitations of this study werethe small sample size which limits its generalization and the fact that a short intervention span of 4 weeks cannot predict attitudes of students over time. Lastly, results of this study would have been stronger if a control group of students who did not receive our intervention were included. However, this study is one that compares attitudes of medical students to the unmodified type of ECT to studies in which medical students viewed the modified type. Conclusion Exposure of medical students to ECT and lectures are important in changing negative attitudes during clerkships and should be incorporated in their teaching curriculum. We may infer that future psychiatrists would prefer the modified form of ECT and acceptability would be better with this format. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09066t4.jpg] [hs09066t2.jpg] [hs09066t3.jpg] [hs09066t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}